Mastering Dorsal Wrist Approach: The Side of Lister Tubercle Revealed
Key Takeaway
Learn more about Mastering Dorsal Wrist Approach: The Side of Lister Tubercle Revealed and how to manage it. The dorsal approach exposes wrist extensor tendons, dorsal carpus, and proximal metacarpals, enabling procedures like synovectomy, wrist fusion, tumor excision, and fracture fixation. An 8-cm longitudinal incision is typically made on the dorsal wrist, guided by anatomical landmarks such as the radial styloid and areas around the side of lister tubercle, to ensure optimal surgical access.
Introduction and Epidemiology
The dorsal approach to the wrist remains a foundational surgical exposure in orthopedic surgery, providing unparalleled visualization of the distal radius, the carpus, and the complex network of extensor tendons. Historically, the dorsal approach was the primary workhorse for the open reduction and internal fixation of distal radius fractures. However, the advent of volar locking plates shifted the paradigm due to the high incidence of extensor tendon irritation and rupture associated with early-generation dorsal hardware. Despite this shift, the dorsal approach remains indispensable for a myriad of complex wrist pathologies.
Epidemiologically, conditions necessitating a dorsal approach are prevalent across diverse patient demographics. Rheumatoid arthritis, which frequently requires dorsal tenosynovectomy and wrist stabilization, affects approximately 0.5 to 1 percent of the global population. Carpal fractures and dislocations, particularly scaphoid fractures and transscaphoid perilunate fracture-dislocations, predominantly affect young, active males following high-energy trauma. Furthermore, the dorsal approach is the gold standard for procedures such as proximal row carpectomy, total wrist arthrodesis, and the management of dorsal shear fractures of the distal radius. Mastery of this approach requires a profound understanding of the dorsal capsuloligamentous structures, the extensor compartments, and the delicate neurovascular anatomy to optimize functional outcomes and minimize iatrogenic morbidity.
Surgical Anatomy and Biomechanics
A rigorous understanding of dorsal wrist anatomy is paramount for safe and effective surgical execution. The dorsal wrist is characterized by a thin soft-tissue envelope, making the underlying structures highly palpable but equally vulnerable to surgical trauma and hardware prominence.
Osteology and Landmarks
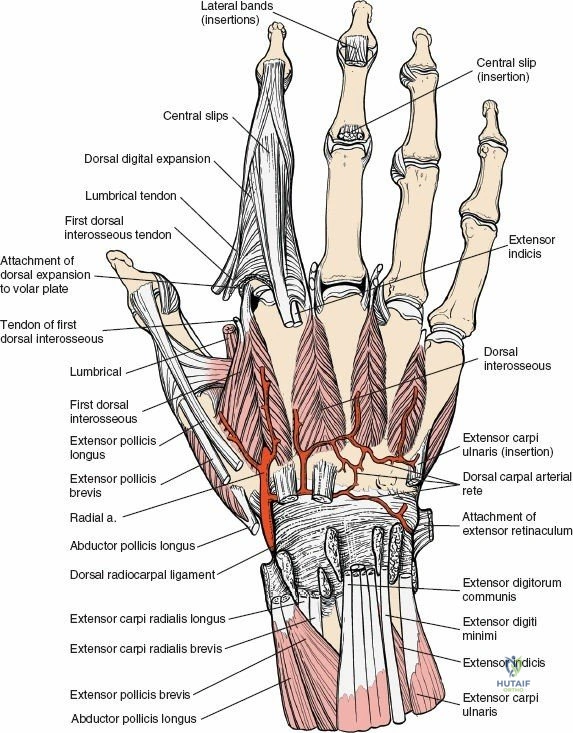
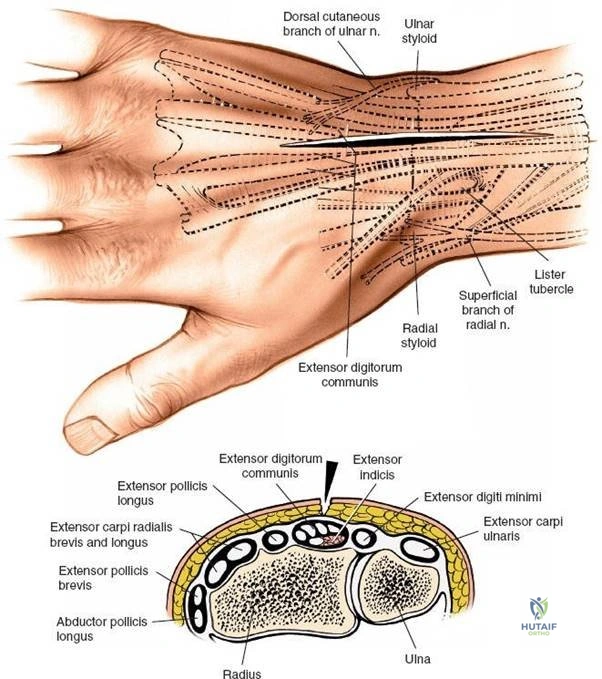
The primary osseous landmark of the dorsal wrist is Lister tubercle, a bony prominence located on the dorsal surface of the distal radius. It serves as a critical anatomical pulley for the extensor pollicis longus tendon. The radial styloid represents the most distal extension of the lateral radius, while the ulnar styloid is palpable on the dorsal aspect of the distal ulna. The dorsal rim of the distal radius acts as a buttress against dorsal carpal subluxation. The carpal bones, particularly the scaphoid, lunate, and triquetrum, form the proximal carpal row, which articulates with the distal radius and the triangular fibrocartilage complex.
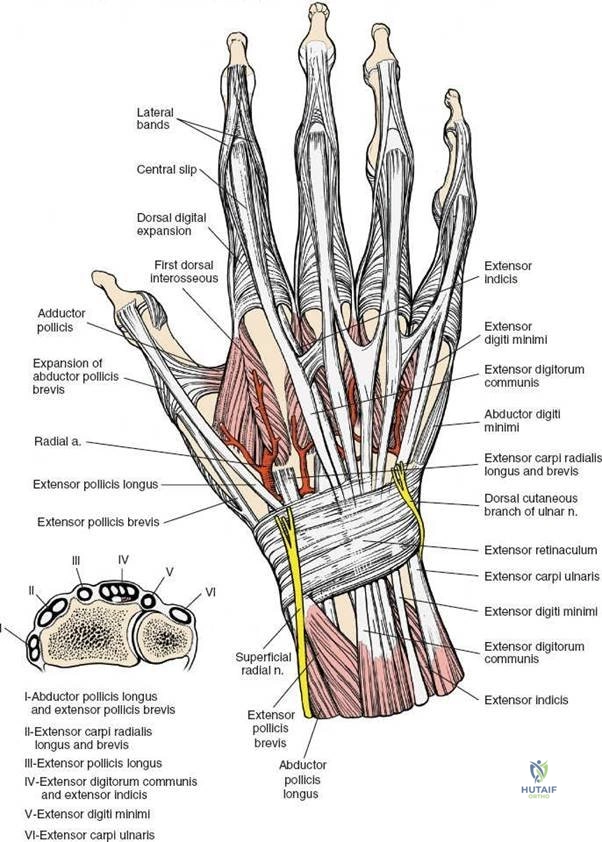
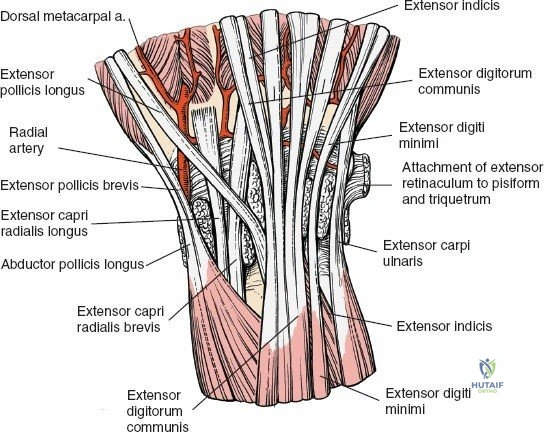
Extensor Compartments of the Wrist
The extensor retinaculum is a specialized fascial band that prevents bowstringing of the extensor tendons. It is partitioned by septa into six distinct fibro-osseous compartments:
* First Compartment: Abductor pollicis longus and extensor pollicis brevis.
* Second Compartment: Extensor carpi radialis longus and extensor carpi radialis brevis.
* Third Compartment: Extensor pollicis longus, which courses obliquely around Lister tubercle.
* Fourth Compartment: Extensor digitorum communis and extensor indicis proprius.
* Fifth Compartment: Extensor digiti minimi.
* Sixth Compartment: Extensor carpi ulnaris.
Neurovascular Structures
The cutaneous innervation of the dorsal wrist is supplied by the superficial sensory branch of the radial nerve radially and the dorsal sensory branch of the ulnar nerve ulnarly. These nerves are highly susceptible to traction injury during superficial dissection. Deep innervation to the wrist capsule is provided by the terminal branches of the posterior interosseous nerve and the anterior interosseous nerve. The posterior interosseous nerve resides in the floor of the fourth extensor compartment and provides critical proprioceptive feedback; it is often targeted for neurectomy in chronic wrist pain syndromes. Vascular supply to the dorsal carpus is derived from the dorsal radiocarpal arch, fed by branches of the radial and ulnar arteries.
Carpal Kinematics and Biomechanics
The dorsal radiocarpal ligament and the dorsal intercarpal ligament form a horizontal "V" configuration that provides dynamic stability to the proximal carpal row. The dorsal radiocarpal ligament originates from the dorsal rim of the radius and inserts onto the lunate and triquetrum, preventing volar translation of the carpus. Preservation or meticulous repair of these ligaments during capsulotomy is essential to prevent postoperative carpal instability, specifically dorsal intercalated segment instability or volar intercalated segment instability.
Indications and Contraindications
The decision to utilize a dorsal approach hinges upon the specific anatomical location of the pathology and the required trajectory for internal fixation or excision.
| Pathology Type | Operative Indications for Dorsal Approach | Non Operative Indications |
|---|---|---|
| Distal Radius Fractures | Dorsal Barton fractures, displaced intra-articular dorsal lip fractures, dorsal comminution requiring fragment-specific fixation | Nondisplaced fractures, extra-articular fractures amenable to closed reduction and casting, severe osteopenia precluding fixation |
| Carpal Trauma | Transscaphoid perilunate dislocations, dorsal perilunate dislocations, scaphoid nonunion requiring dorsal bone grafting | Nondisplaced carpal fractures, stable ligamentous sprains |
| Inflammatory Arthropathy | Rheumatoid arthritis with severe extensor tenosynovitis, impending extensor tendon rupture, need for dorsal stabilization or Darrach procedure | Mild tenosynovitis responsive to disease-modifying antirheumatic drugs and corticosteroid injections |
| Degenerative Conditions | Scapholunate advanced collapse or scaphoid nonunion advanced collapse requiring proximal row carpectomy or four-corner fusion | Early-stage osteoarthritis managed with bracing and intra-articular injections |
| Neoplastic Conditions | Benign or malignant tumors of the dorsal distal radius, dorsal carpus, or extensor tendons (e.g., giant cell tumor of tendon sheath) | Small, asymptomatic, non-progressive benign cysts (e.g., occult dorsal ganglions) |
Relative contraindications for the dorsal approach include isolated volar pathology (e.g., volar shear fractures, volar perilunate dislocations) and severely compromised dorsal soft tissues due to prior trauma, burn contractures, or active infection. In cases of distal radius fractures with significant volar displacement, a volar approach is strictly indicated.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning includes a comprehensive radiographic evaluation. Standard posteroanterior, lateral, and oblique radiographs of the wrist are mandatory. Computed tomography is highly recommended for intra-articular distal radius fractures to map articular step-offs, gap formations, and the exact location of dorsal fragments. Magnetic resonance imaging is indicated for evaluating ligamentous injuries, avascular necrosis of the carpus, and soft tissue neoplasms.
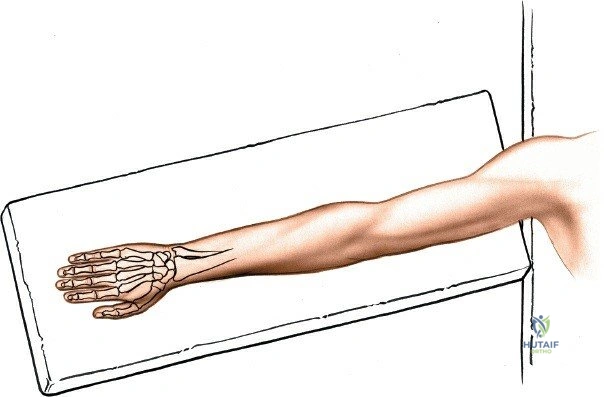
The patient is positioned supine on the operating table. The affected upper extremity is extended onto a radiolucent hand table or arm board to facilitate intraoperative fluoroscopy. The forearm is fully pronated to present the dorsal aspect of the wrist to the surgeon. A well-padded pneumatic tourniquet is applied to the proximal arm. Following standard surgical skin preparation and draping, the limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to the appropriate pressure (typically 250 mmHg or 100 mmHg above systolic blood pressure). Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Detailed Surgical Approach and Technique
The dorsal approach can be tailored to access specific columns of the distal radius or specific carpal intervals. The following steps detail a comprehensive, extensile exposure.
Landmarks and Incision
The surgeon begins by palpating the radial styloid laterally, the ulnar styloid medially, and Lister tubercle centrally on the distal radius.
A longitudinal incision of approximately 8 cm is made on the dorsal aspect of the wrist. The incision is centered precisely over Lister tubercle, crossing the radiocarpal joint midway between the radial and ulnar styloids. The incision begins 3 cm proximal to the radiocarpal joint and extends approximately 5 cm distal to it. While transverse incisions offer superior cosmesis, longitudinal incisions are preferred for trauma and complex reconstructions as they are extensile and provide superior exposure of the extensor compartments. The redundant and pliable nature of the dorsal wrist skin ensures that a longitudinal incision crossing the wrist creases rarely results in functional contracture.
Superficial Surgical Dissection
The skin and subcutaneous fat are incised in line with the skin incision. Meticulous hemostasis is achieved using bipolar electrocautery. During this superficial dissection, extreme caution must be exercised to identify and protect the superficial sensory branches of the radial nerve radially and the dorsal sensory branches of the ulnar nerve ulnarly. Large dorsal bridging veins should be preserved when possible to minimize postoperative edema; however, veins directly obstructing the surgical field may be ligated.
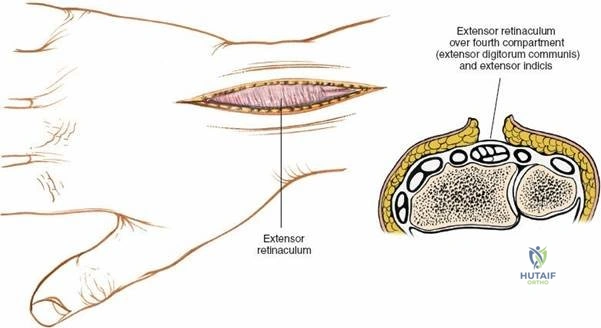
Deepening the dissection exposes the extensor retinaculum. The retinaculum is a thick, transverse band of fascia that spans the dorsal wrist. The borders of the six extensor compartments are visually identified.
Deep Surgical Dissection and Compartment Management
The deep dissection is dictated by the specific pathology being addressed. Access to the radiocarpal joint and distal radius typically involves mobilization of the third extensor compartment.
The third extensor compartment, housing the extensor pollicis longus tendon, is opened longitudinally. The incision is made on the ulnar side of Lister tubercle. The extensor pollicis longus tendon is mobilized and retracted radially. This exposes the floor of the third compartment and Lister tubercle.
For broader exposure of the distal radius, a subperiosteal elevation is performed. The second compartment tendons (extensor carpi radialis longus and brevis) are elevated radially, and the fourth compartment tendons (extensor digitorum communis and extensor indicis proprius) are elevated ulnarly. Lister tubercle can be excised with a rongeur or osteotome if a flat surface is required for the application of a dorsal plate.
Capsulotomy Techniques
When access to the carpus or the radiocarpal joint is required, a capsulotomy is performed. The choice of capsulotomy is critical to preserve carpal stability.
The Berger ligament-sparing capsulotomy is the gold standard. This technique involves creating a radially based, V-shaped flap of the dorsal wrist capsule. The incision follows the orientation of the dorsal intercarpal ligament proximally and the dorsal radiocarpal ligament distally. The apex of the flap is located ulnarly, near the triquetrum. This flap is carefully elevated off the underlying carpal bones, providing excellent visualization of the scaphoid, lunate, and radiocarpal articulation. Upon completion of the intra-articular procedure, the capsular flap is repaired meticulously with non-absorbable sutures to restore dorsal carpal stability.
Internervous Planes
A unique anatomical feature of the dorsal approach to the wrist is the absence of a true internervous plane. All muscles whose tendons are manipulated during this approach (extensor carpi radialis longus/brevis, extensor pollicis longus, extensor digitorum communis) share a common innervation from the posterior interosseous nerve. However, because the motor branches of the posterior interosseous nerve innervate these muscle bellies far proximally in the forearm (near the elbow), the intermuscular planes at the level of the wrist can be utilized safely without risk of denervation.
Reduction and Fixation Principles
For distal radius fractures, once the fracture site is exposed, hematoma and soft tissue interposition are cleared. The fracture is reduced under direct vision, utilizing traction, ligamentotaxis, and direct manipulation with dental picks or elevators. Provisional fixation is achieved with Kirschner wires. If dorsal plating is indicated, low-profile, anatomically contoured plates are utilized. The plate is applied directly to the bone, beneath the extensor tendons. Fragment-specific fixation may involve the use of small pin-plates or wire forms to capture specific dorsal ulnar or dorsal radial fragments.
Following hardware placement or carpal reconstruction, the extensor retinaculum is repaired. However, to prevent hardware-induced tendon attrition, the extensor pollicis longus tendon is frequently left transposed in the subcutaneous tissues, outside of the retinaculum. The retinaculum is then repaired beneath the extensor pollicis longus tendon, providing a smooth fascial layer over the dorsal hardware.
Complications and Management
The dorsal approach, while providing excellent exposure, is associated with specific complications, primarily related to the extensor tendons and cutaneous nerves.
| Complication | Incidence Rate | Etiology and Clinical Presentation | Management and Salvage Strategies |
|---|---|---|---|
| Extensor Tendon Irritation or Rupture | 3% to 10% (historically higher with older plates) | Friction of tendons (especially EPL and EDC) against prominent dorsal hardware or sharp bone edges. Presents as pain, crepitus, or sudden loss of active extension. | Prevention: Use low-profile plates, leave EPL transposed subcutaneously. Salvage: Hardware removal, tendon transfer (e.g., EIP to EPL transfer for EPL rupture). |
| Superficial Nerve Injury or Neuroma | 2% to 5% | Iatrogenic traction or laceration of the SBRN or DBUN during superficial dissection. Presents as paresthesia, hypersensitivity, or a positive Tinel sign. | Prevention: Meticulous superficial dissection. Salvage: Neuroma excision and implantation of the nerve stump into deep muscle or bone. |
| Joint Stiffness and Capsular Contracture | 10% to 15% | Prolonged immobilization, excessive capsular scarring, or failure to repair the capsular flap anatomically. Presents as restricted flexion/extension arc. | Prevention: Rigid internal fixation allowing early active ROM. Salvage: Aggressive hand therapy, dynamic splinting, or surgical capsulotomy for refractory cases. |
| Carpal Instability | 1% to 3% | Failure to properly repair the dorsal radiocarpal or dorsal intercarpal ligaments during capsulotomy. Presents as midcarpal pain, clunking, or radiographic DISI/VISI. | Prevention: Use ligament-sparing capsulotomy techniques (Berger flap). Salvage: Ligament reconstruction or limited intercarpal arthrodesis. |
| Complex Regional Pain Syndrome | 2% to 7% | Exaggerated inflammatory and neuropathic response to surgery. Presents as severe pain, swelling, vasomotor instability, and trophic changes. | Prevention: Atraumatic technique, adequate postoperative analgesia. Salvage: Multidisciplinary approach, gabapentinoids, sympathetic nerve blocks, aggressive therapy. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is highly dependent on the specific procedure performed, the stability of the fixation, and the quality of the patient's bone and soft tissues. The following represents a generalized protocol for a patient who has undergone stable open reduction and internal fixation of a distal radius fracture via a dorsal approach.
Phase 1: Immediate Post Operative Period (Weeks 0 to 2)
The primary goals during this phase are edema control, pain management, and protection of the surgical site. The patient is placed in a bulky, non-circumferential volar resting splint with the wrist in slight extension. Immediate active range of motion of the fingers, thumb, elbow, and shoulder is initiated to prevent stiffness and promote venous return. Tendon gliding exercises are emphasized to prevent adhesions of the extensor tendons over the surgical site. Sutures are typically removed at 10 to 14 days.
Phase 2: Early Mobilization (Weeks 2 to 6)
If rigid fixation was achieved, the bulky splint is transitioned to a custom-molded thermoplastic splint, which is removed for hygiene and structured therapy sessions. Active and active-assisted range of motion of the wrist (flexion, extension, pronation, supination) is initiated. Passive stretching is generally avoided during this early phase to prevent hardware failure or displacement of fracture fragments. Scar massage and desensitization techniques are implemented once the incision is fully healed.
Phase 3: Strengthening and Functional Restoration (Weeks 6 to 12)
Radiographic evaluation is performed at 6 weeks to confirm clinical and radiographic union. Once union is progressing satisfactorily, the protective splint is discontinued. Progressive resistive exercises are introduced, starting with isometric strengthening and advancing to isotonic exercises using light weights and resistance bands. Proprioceptive training and work-specific functional activities are incorporated. Full functional recovery, particularly regarding grip strength and terminal range of motion, may take up to one year.
Summary of Key Literature and Guidelines
The evolution of the dorsal approach to the wrist is well-documented in the orthopedic literature. The anatomical basis for the ligament-sparing capsulotomy was definitively described by Berger et al., who mapped the dorsal radiocarpal and intercarpal ligaments, demonstrating that a carefully designed capsular flap prevents postoperative carpal instability.
The management of extensor tendons during dorsal plating has been a subject of extensive research. Studies by Ring and Jupiter highlighted the unacceptably high rates of extensor tendon rupture with early-generation, thick dorsal plates, leading to the widespread adoption of the volar approach. However, contemporary biomechanical and clinical studies evaluating low-profile, fragment-specific dorsal plating systems have demonstrated significantly reduced rates of tendon complications, provided that meticulous surgical technique is employed, including the routine subcutaneous transposition of the extensor pollicis longus tendon.
Current guidelines from the American Academy of Orthopaedic Surgeons on the management of distal radius fractures recognize both volar and dorsal approaches as valid, emphasizing that the choice of approach must be dictated by the specific fracture morphology. The dorsal approach remains the undisputed gold standard for addressing dorsal comminution, dorsal Barton fractures, and complex carpal pathology requiring direct visualization of the radiocarpal and midcarpal joints. Continuous advancements in low-profile implant technology and a deeper understanding of dorsal wrist kinematics ensure that the dorsal approach remains a critical tool in the armamentarium of the modern orthopedic surgeon.
