Comprehensive Introduction and Patho-Epidemiology
The wrist and hand represent a marvel of biomechanical engineering, functioning as a highly complex, intercalated terminal effector organ that facilitates both powerful prehension and delicate fine motor manipulation. Surgical approaches to this region demand an uncompromising mastery of its intricate three-dimensional anatomy, as the dense concentration of neurovascular, tendinous, and osteoarticular structures leaves virtually no margin for error. In this definitive chapter, we will comprehensively explore the essential surgical approaches required to uncover every aspect of the wrist, with a particular emphasis on the dorsal approach, its utilitarian extensions, and the broader topographical surgical anatomy of the hand. Historically, the dorsal approach to the wrist was the workhorse for distal radius fracture fixation; however, the evolution of fixed-angle volar locking plates has shifted the paradigm. Nevertheless, the dorsal approach remains absolutely indispensable for the management of rheumatoid synovitides, carpal instability, perilunate fracture-dislocations, proximal row carpectomies, and total wrist arthrodeses.
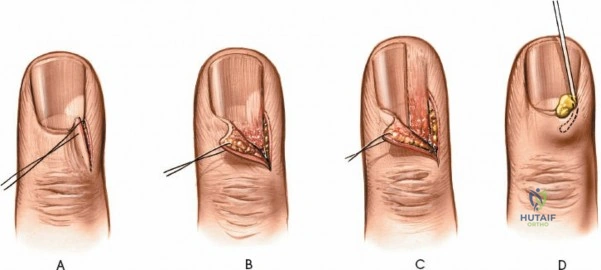
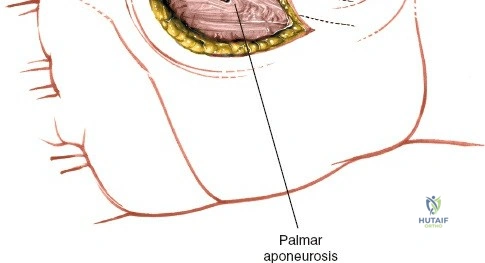
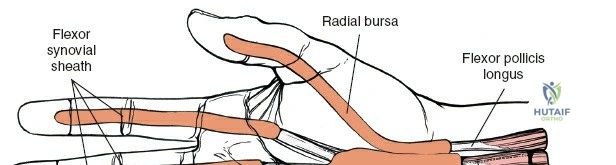
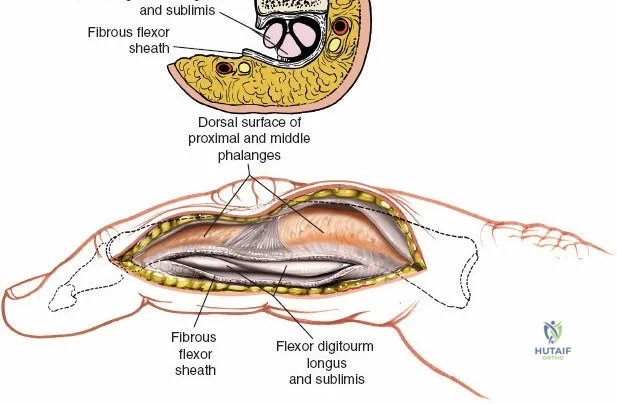
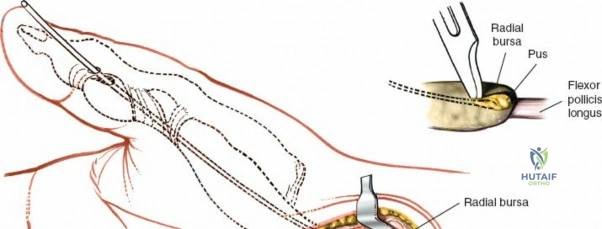
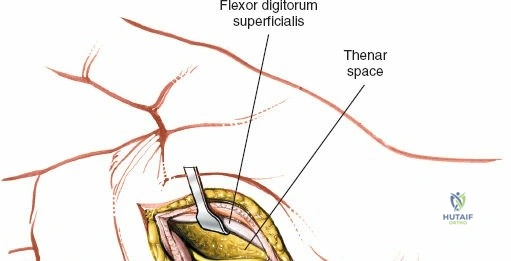
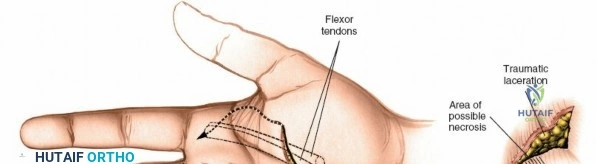
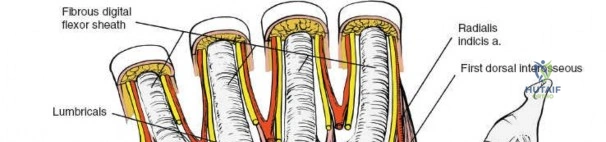
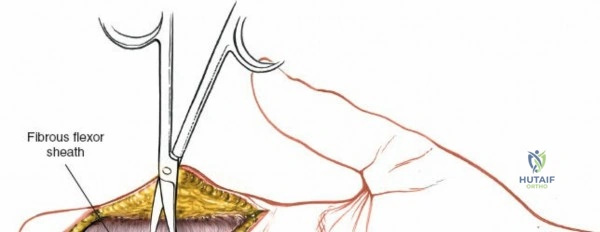
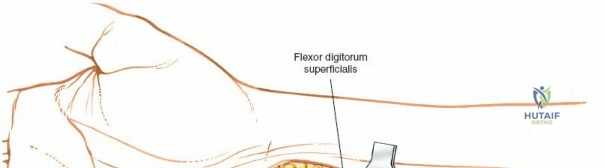
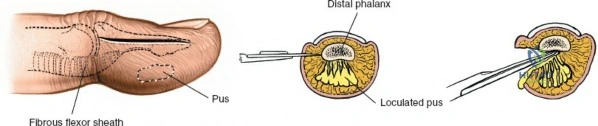
The epidemiology of wrist and hand pathology dictates that orthopedic surgeons will frequently encounter trauma, degenerative conditions, and deep space infections within this anatomical territory. Distal radius fractures account for approximately one-sixth of all fractures evaluated in emergency departments, with a bimodal distribution affecting high-energy trauma in the young and low-energy osteoporotic falls in the elderly. Concurrently, inflammatory arthropathies, particularly rheumatoid arthritis, frequently target the radiocarpal and midcarpal joints, leading to progressive carpal collapse, ulnar translocation, and devastating extensor tendon ruptures (Vaughan-Jackson syndrome). Infection within the hand, while mitigated by the advent of modern intravenous antimicrobial therapy, remains a formidable clinical challenge. Paronychia and felons (pulp space infections) constitute the vast majority of surgical infections, but the surgeon must remain vigilant for purulent flexor tenosynovitis and deep space infections (thenar, midpalmar, and web spaces) that threaten the viability of the entire hand.
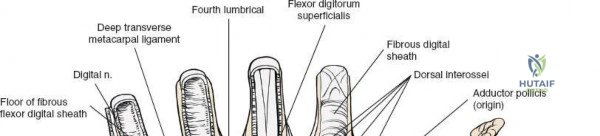
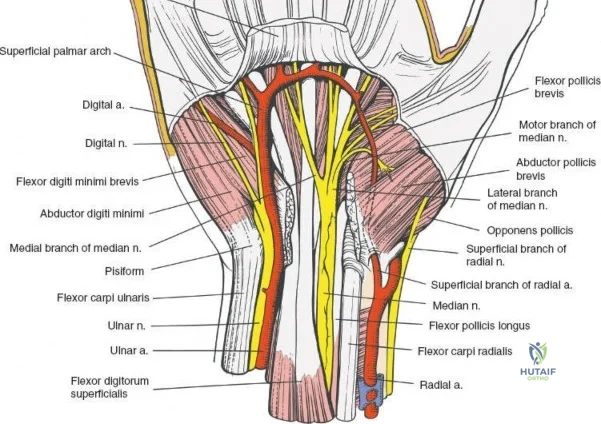
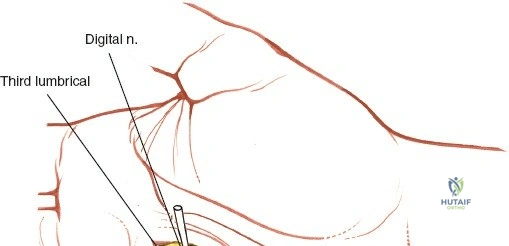
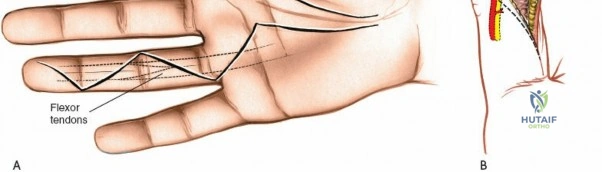
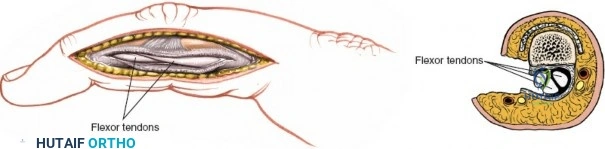
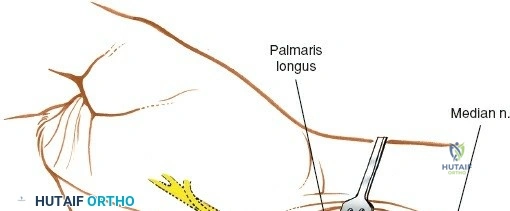
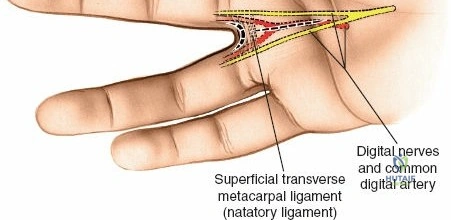
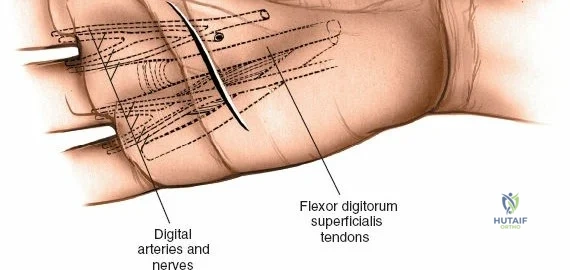
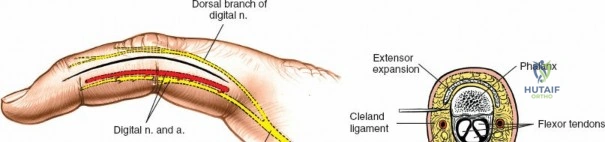
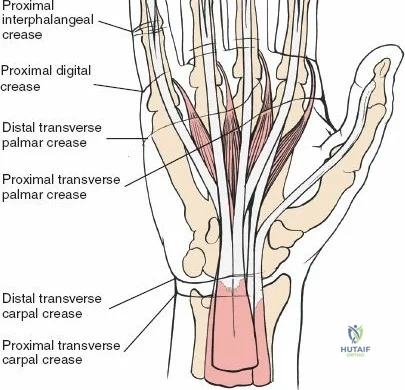
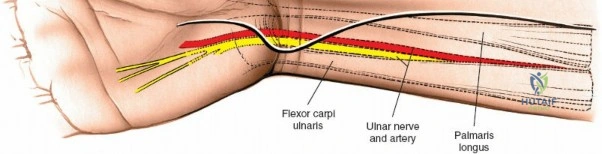
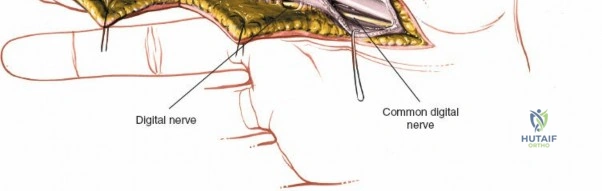
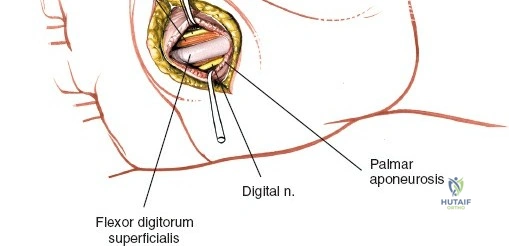
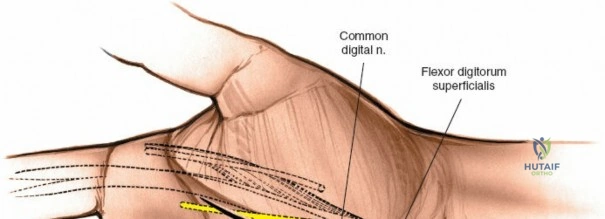
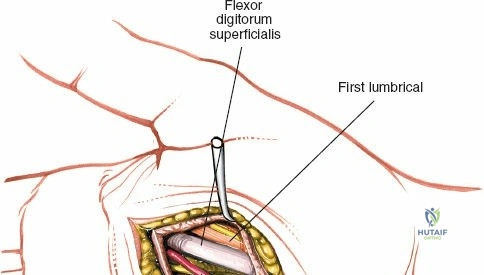
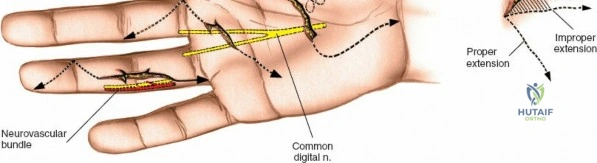
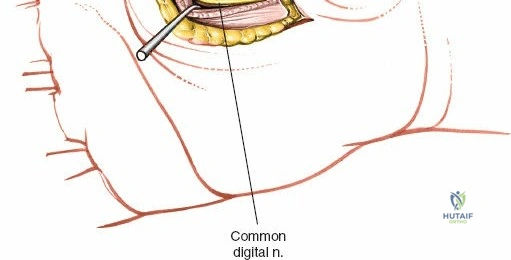
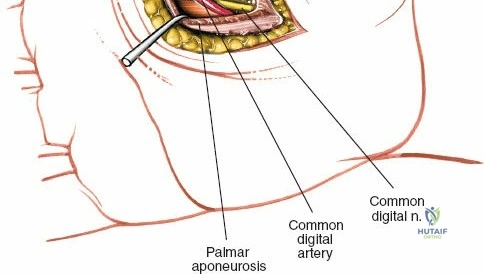
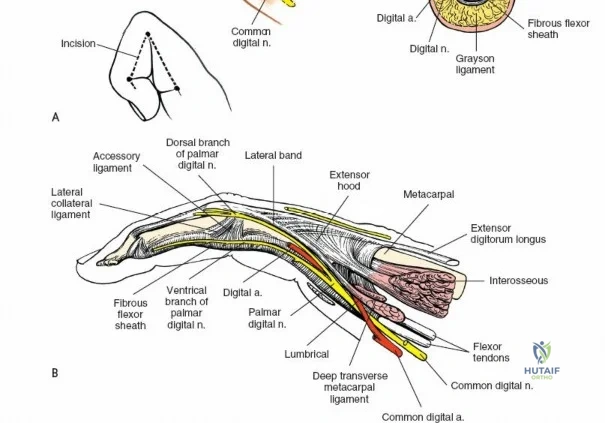
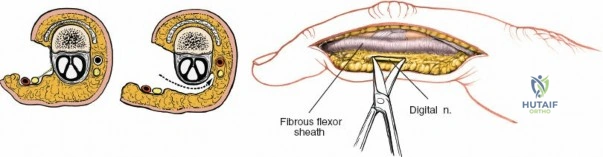
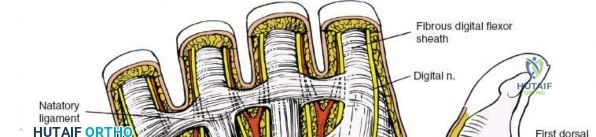
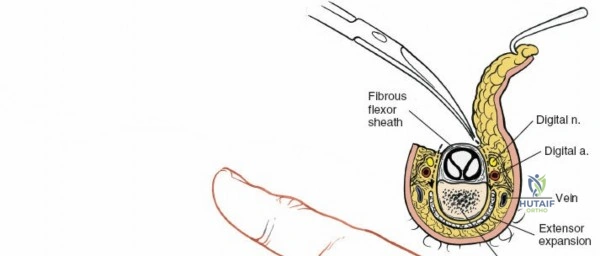
Throughout the surgical management of the hand and wrist, the foundational principle is that clinical findings direct the diagnosis, but profound anatomical knowledge prevents catastrophic iatrogenic injury and ensures comprehensive treatment. The majority of wounds encountered in hand surgery arise from unpredictable trauma rather than meticulously planned surgical incisions. Therefore, understanding the topographic anatomy is paramount. For instance, arterial hemorrhage from a digital artery strongly implies concomitant injury to the adjacent digital nerve, as the nerve lies volar to the artery in the digit. Such nuanced understanding prevents the surgeon from overlooking a neurapraxia or axonotmesis during a brief emergency department examination. In total, over eighteen distinct approaches to the wrist and hand are utilized in modern practice, encompassing neural decompressions, flexor tendon explorations, scaphoid fixations, and sepsis drainage, all of which rely on the foundational anatomical principles detailed herein.

Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Anatomy of the Wrist
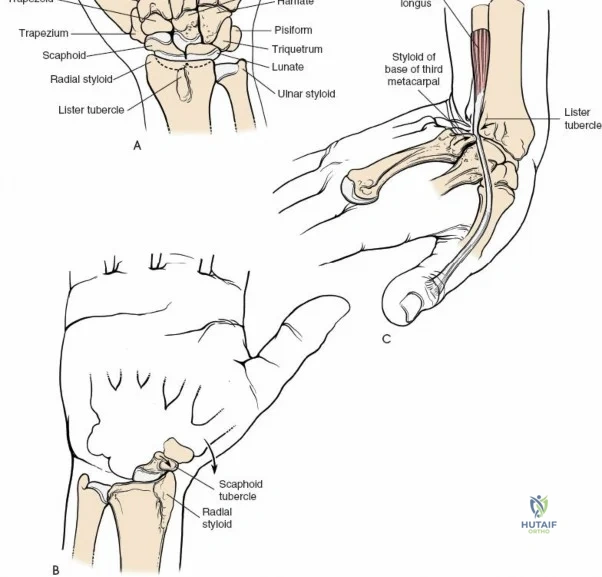
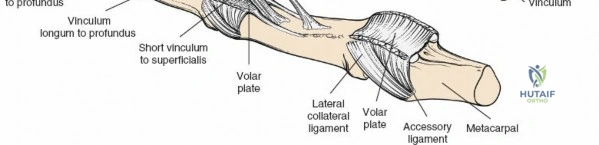
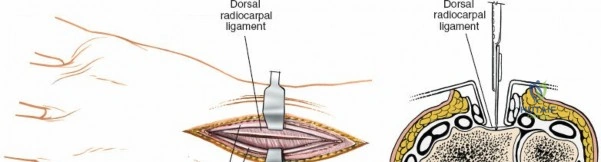
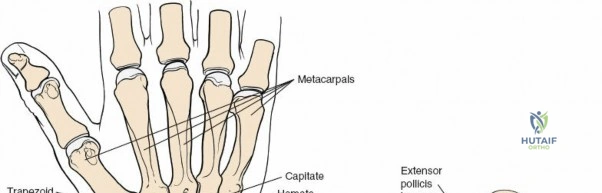
The wrist is not a single joint but a complex articulation comprising the radiocarpal, midcarpal, and distal radioulnar joints (DRUJ). The distal radius presents two primary articular fossae—the scaphoid and lunate fossae—separated by the interfossal ridge. The dorsal rim of the distal radius is characterized by Lister's tubercle, a critical bony landmark that acts as a fulcrum for the extensor pollicis longus (EPL) tendon. The carpus itself is arranged in two distinct rows: the proximal row (scaphoid, lunate, triquetrum), which acts as an intercalated segment devoid of direct tendinous insertions, and the distal row (trapezium, trapezoid, capitate, hamate), which functions as a rigid unit coupled to the metacarpal bases. The kinematics of the wrist rely on the delicate balance of intrinsic ligaments (e.g., scapholunate interosseous ligament) and extrinsic capsular ligaments (e.g., dorsal radiocarpal and dorsal intercarpal ligaments), which form a vital dorsal V-shaped stabilizer against volar carpal subluxation.

Dorsal Extensor Compartments and Retinacular Anatomy
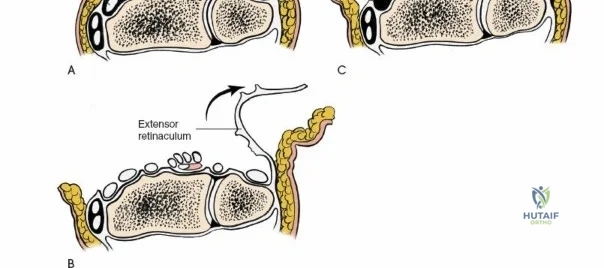
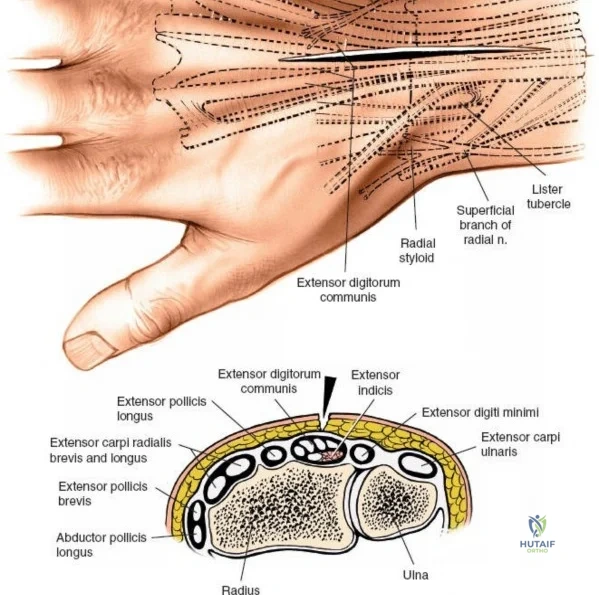
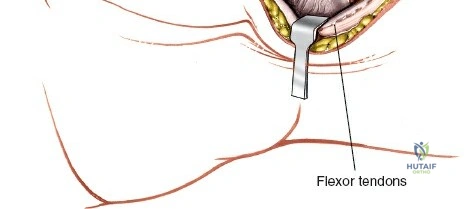
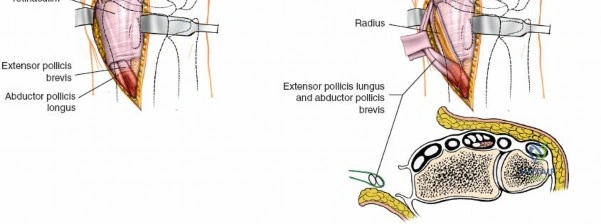
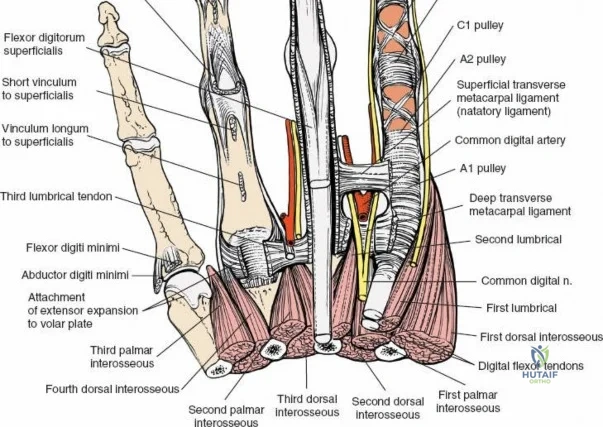
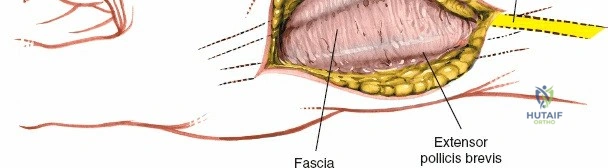
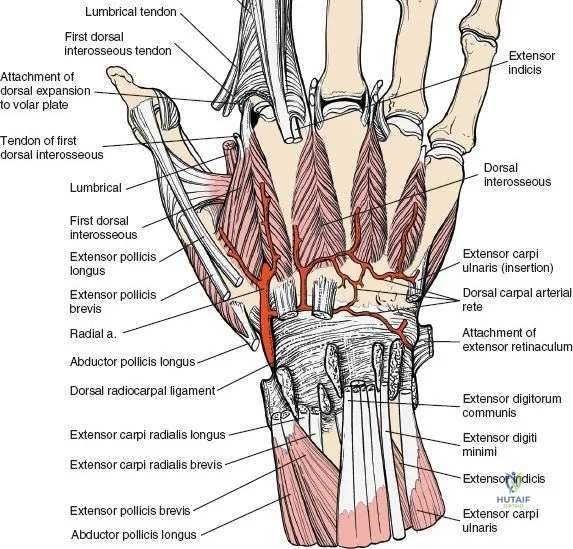
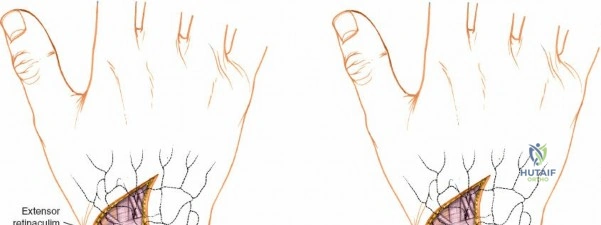
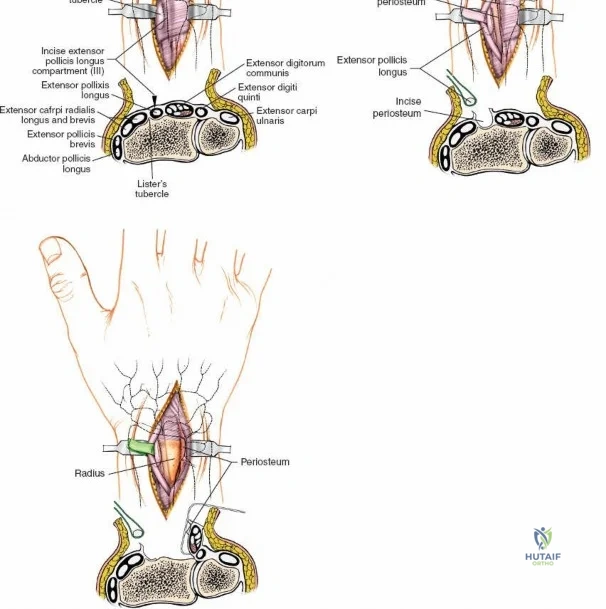
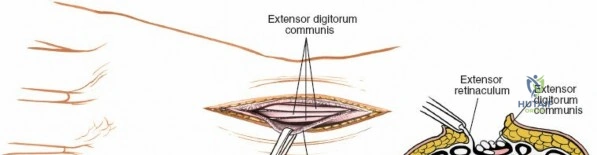
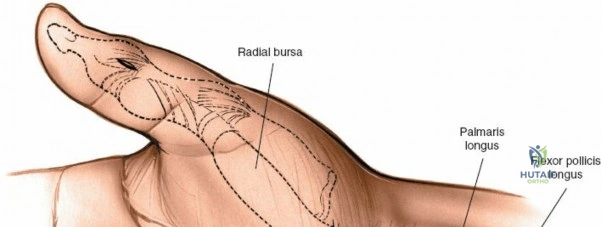
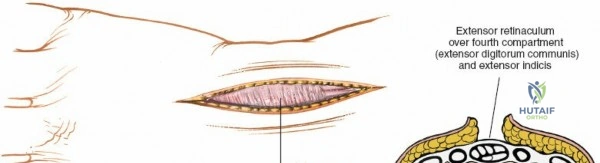
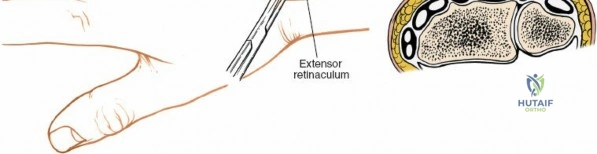
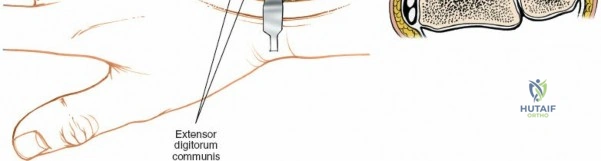
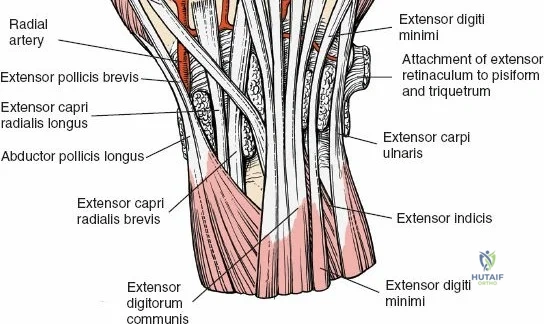
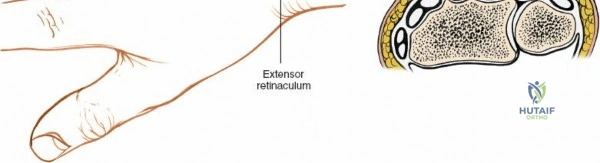
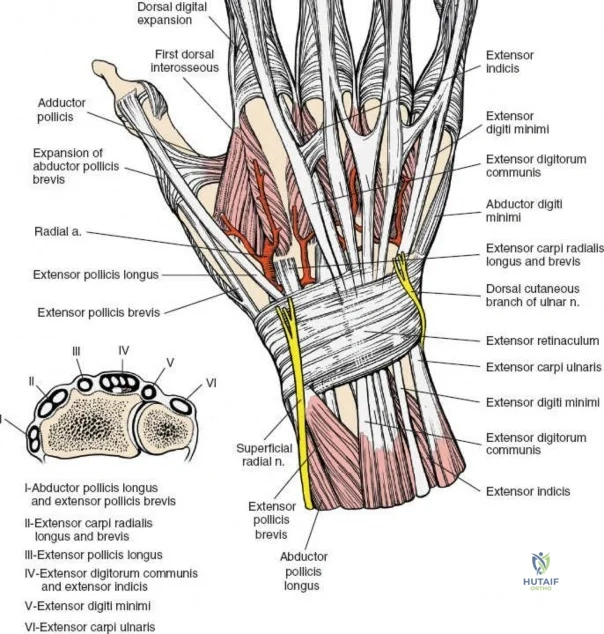
The dorsal approach to the wrist necessitates a flawless understanding of the extensor retinaculum and the six dorsal extensor compartments. The extensor retinaculum is a specialized fascial band that prevents bowstringing of the extensor tendons during wrist extension. The first compartment, located on the radial border, houses the abductor pollicis longus (APL) and extensor pollicis brevis (EPB). The second compartment contains the extensor carpi radialis longus (ECRL) and brevis (ECRB). The third compartment, uniquely angled around Lister's tubercle, contains the EPL. The fourth compartment, the broadest of the six, houses the extensor digitorum communis (EDC) and the extensor indicis proprius (EIP). The fifth compartment contains the extensor digiti minimi (EDM), located directly over the DRUJ, and the sixth compartment contains the extensor carpi ulnaris (ECU), which plays a critical role in stabilizing the ulnar aspect of the wrist.

Neurovascular Topography of the Hand and Wrist
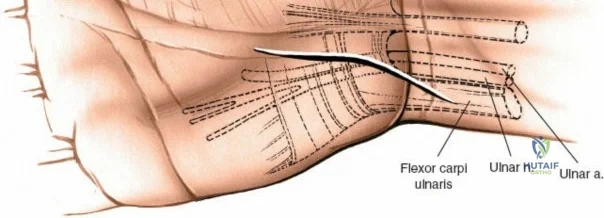
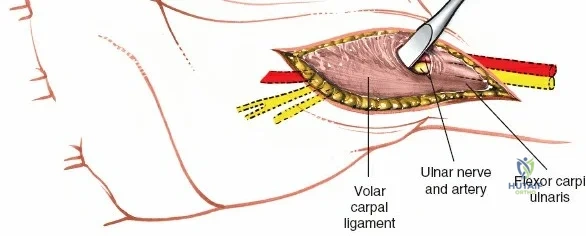
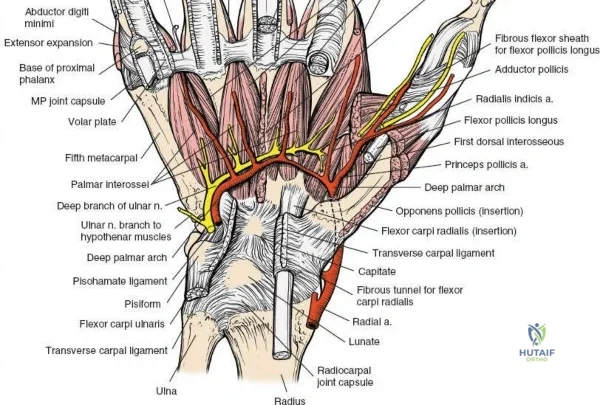
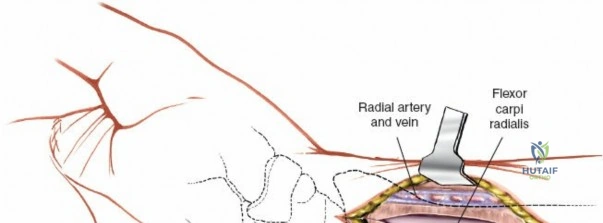
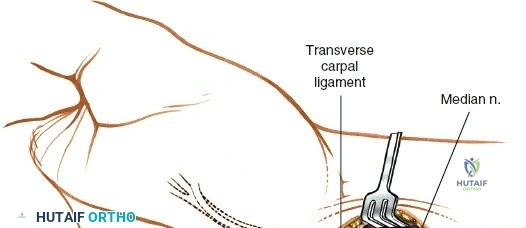
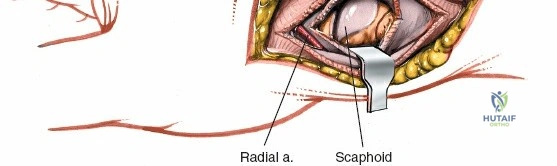
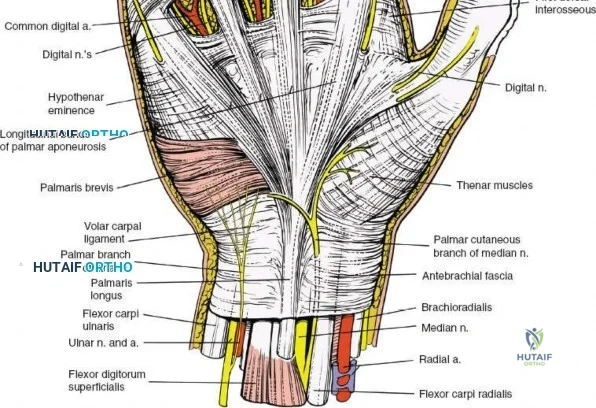
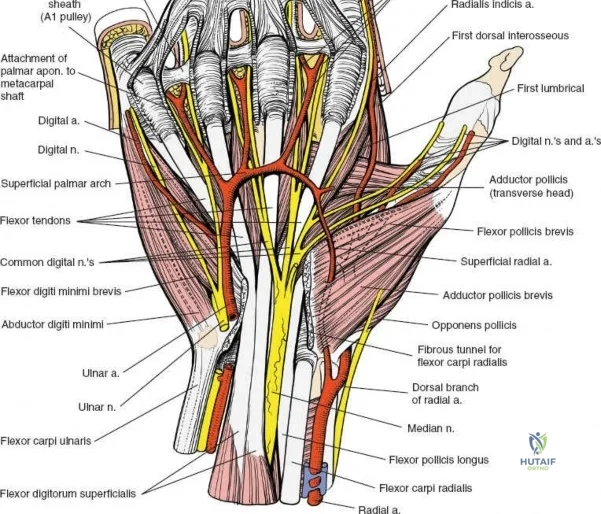
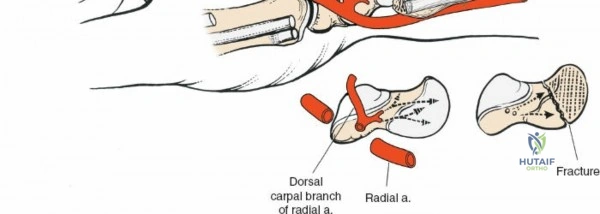
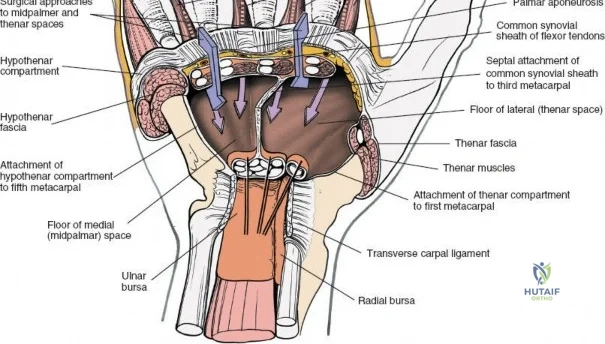
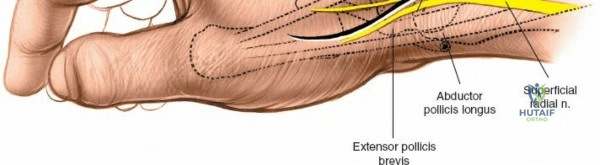
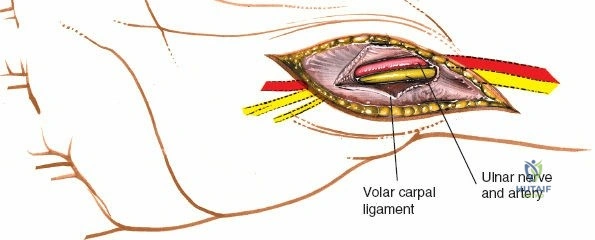
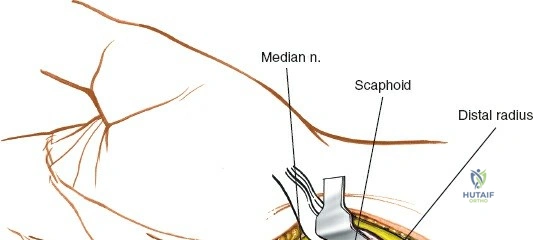
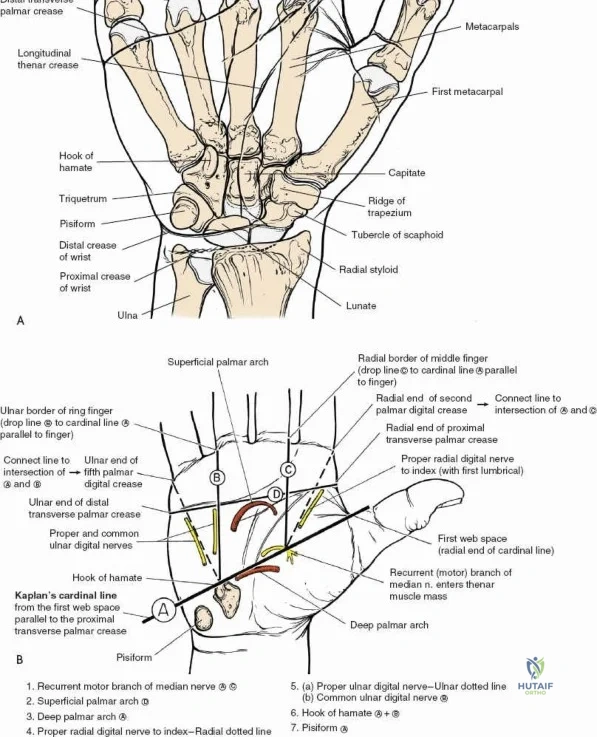
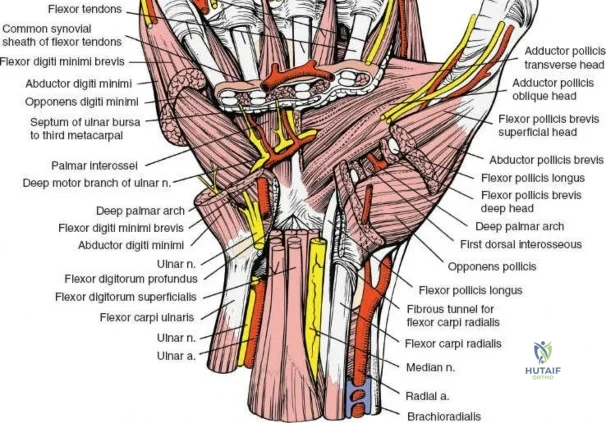
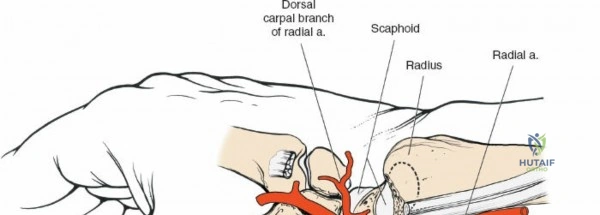
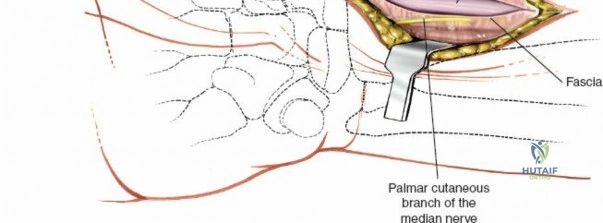
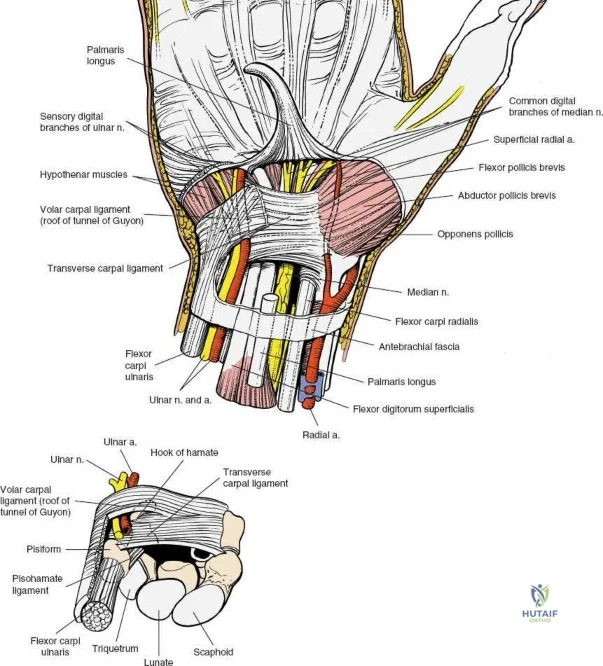
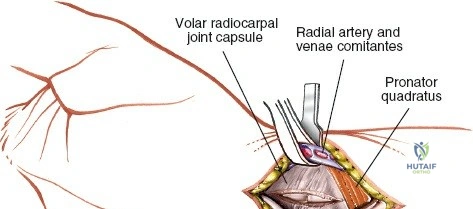
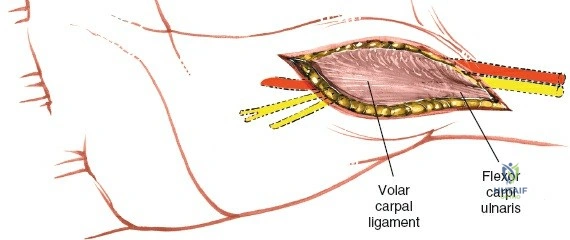
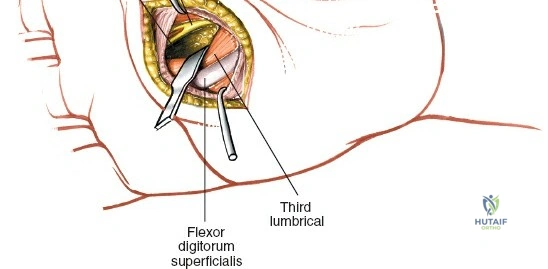
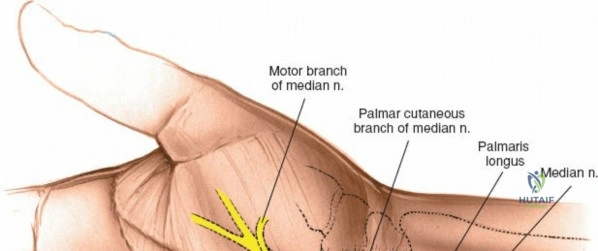
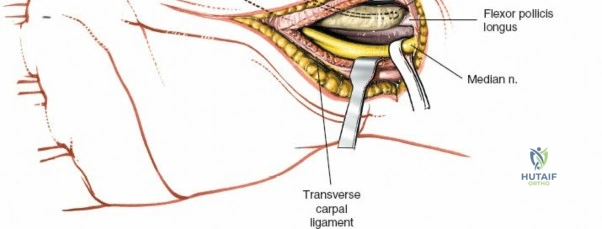
The neurovascular supply to the hand is an intricate web that demands meticulous preservation during any surgical approach. On the dorsum, the superficial branch of the radial nerve (SBRN) emerges from beneath the brachioradialis approximately 9 cm proximal to the radial styloid, arborizing into delicate branches that provide sensation to the dorsal radial aspect of the hand. The dorsal sensory branch of the ulnar nerve (DSBUN) crosses the ulnar styloid to supply the dorsal ulnar hand. In the deep palmar spaces, understanding the vascular supply is critical, particularly the retrograde blood supply of the scaphoid. The radial artery gives off dorsal carpal branches that enter the scaphoid at its distal pole and waist, leaving the proximal pole entirely dependent on intraosseous retrograde flow, explaining the high rates of avascular necrosis in proximal pole fractures. Furthermore, the deep palmar space is divided into the thenar (lateral) and midpalmar (medial) spaces by a fibrous septum attaching to the third metacarpal, dictating the pathways of deep space purulence.
Exhaustive Indications and Contraindications
The decision to utilize a specific surgical approach to the wrist is dictated by the pathology, the required exposure, and the condition of the overlying soft tissues. The dorsal approach is exceptionally versatile, providing unparalleled access to the extensor tendons, the dorsal carpus, and the proximal metacarpals. It is the gold standard for procedures requiring direct visualization of the radiocarpal and midcarpal joints, such as total wrist arthrodesis, proximal row carpectomy (PRC), and four-corner fusion. In the realm of trauma, it is indicated for displaced intra-articular dorsal lip fractures of the radius (dorsal Barton's), dorsal radiocarpal dislocations, and transscaphoid perilunate fracture-dislocations where direct reduction of the dorsal lunate is mandatory. Furthermore, in rheumatoid arthritis, the dorsal approach is obligatory for dorsal tenosynovectomy, Darrach procedures, and the transfer of tendons to reconstruct ruptured extensors.

Conversely, the dorsal approach is relatively contraindicated for routine, simple extra-articular distal radius fractures, which are now predominantly managed with volar locking plates to avoid extensor tendon irritation and hardware prominence. It is absolutely contraindicated in the presence of severe dorsal soft tissue compromise, active dorsal skin infections, or massive dorsal crush injuries where creating a surgical flap would precipitate skin necrosis. In complex intra-articular fractures with significant volar comminution (volar shear fractures), a dorsal approach alone is insufficient and may lead to catastrophic failure of fixation; a volar or combined approach is necessitated.
| Indication Category | Specific Pathologies / Procedures | Relative / Absolute Contraindications |
|---|---|---|
| Degenerative / Inflammatory | Rheumatoid dorsal tenosynovectomy, Vaughan-Jackson repair, Total wrist arthrodesis, Proximal row carpectomy, Four-corner fusion. | Active soft tissue infection (Absolute), Severe dorsal skin atrophy precluding closure (Relative). |
| Trauma / Fractures | Dorsal Barton's fractures, Transscaphoid perilunate dislocations, Dorsal radiocarpal dislocations, Scaphoid nonunion (dorsal approach for proximal pole). | Volar shear fractures (Absolute for dorsal-only), Routine extra-articular distal radius fractures (Relative). |
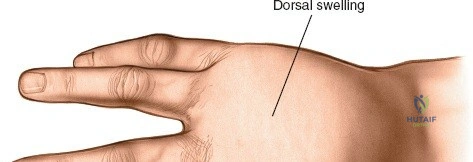
| Oncology / Cysts | Excision of dorsal wrist ganglions, Resection of distal radius tumors (giant cell tumors), Carpal boss excision. | Volar-based tumors requiring palmar neurovascular dissection (Absolute). |
| Infection | Drainage of dorsal subcutaneous abscesses, Septic arthritis of the radiocarpal joint. | Palmar deep space infections requiring volar drainage (Absolute). |


Pre-Operative Planning, Templating, and Patient Positioning
Diagnostic Imaging and Templating
Meticulous pre-operative planning begins with high-quality orthogonal radiographs of the wrist, including posteroanterior (PA), lateral, and specialized views such as the scaphoid view or clenched-fist PA to evaluate dynamic scapholunate instability. For complex intra-articular fractures or carpal dislocations, a fine-cut non-contrast computed tomography (CT) scan with 3D reconstructions is mandatory to delineate articular comminution, fragment size, and step-offs. Magnetic resonance imaging (MRI) is reserved for evaluating the integrity of the interosseous ligaments, the triangular fibrocartilage complex (TFCC), and the vascular status of the scaphoid or lunate (e.g., Kienböck's disease). Digital templating software should be utilized to select appropriate plate sizes, anticipate screw trajectories, and plan the extent of bony resection in procedures like proximal row carpectomy or ulnar shortening osteotomy.
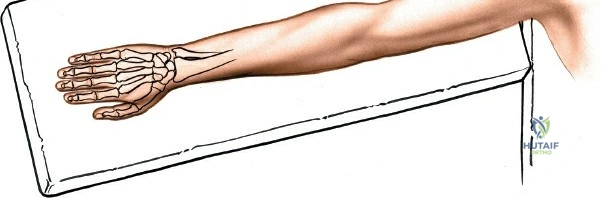
Positioning and Tourniquet Application
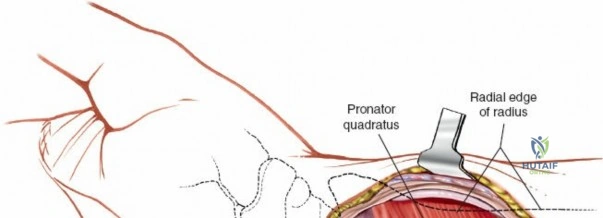
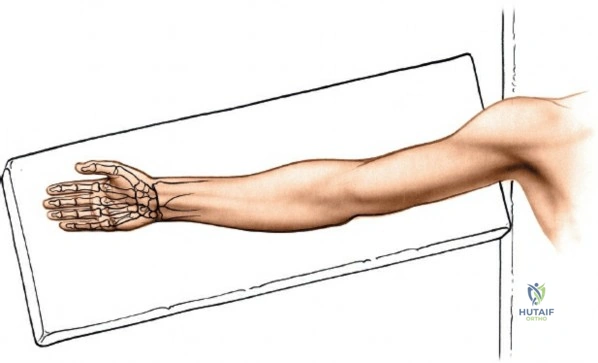
Optimal patient positioning is critical for surgical ergonomics and exposure. The patient is placed supine on the operating table. The operative upper extremity is extended onto a radiolucent hand table to facilitate unobstructed intraoperative fluoroscopy. The arm is exsanguinated using a soft rubber Esmarch bandage, and a pneumatic tourniquet applied to the proximal arm is inflated to 250 mmHg (or 100 mmHg above systolic blood pressure) to ensure a bloodless surgical field. The forearm is pronated for the dorsal approach. The surgeon typically sits in the axilla, facing the hand, with the surgical assistant seated opposite. A sterile stockinette and extremity drape are applied, allowing full mobilization of the elbow, wrist, and digits during the procedure.

Step-by-Step Surgical Approach and Fixation Technique
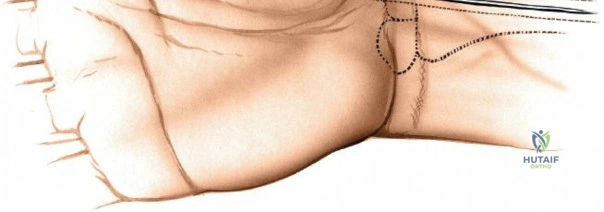
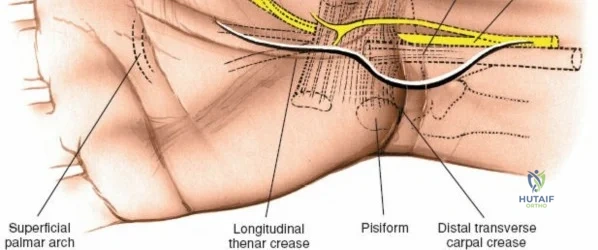
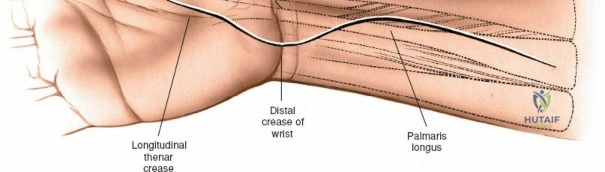
Landmarks and Incision Strategy
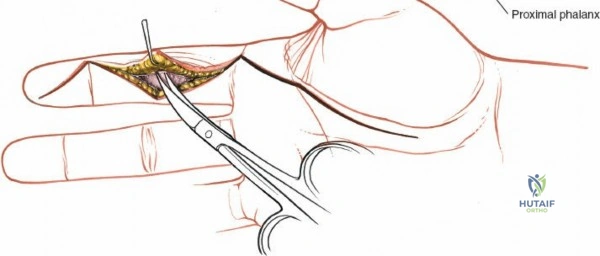
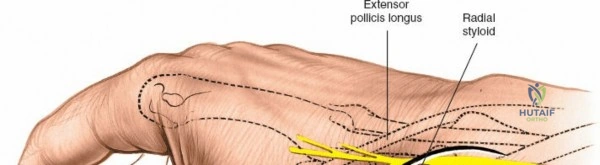
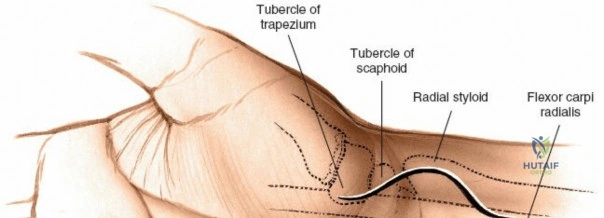
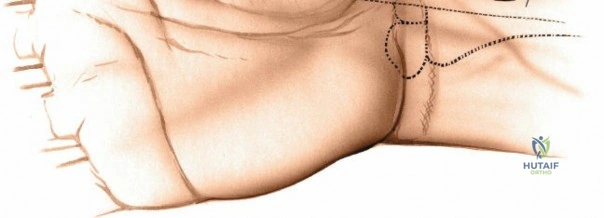
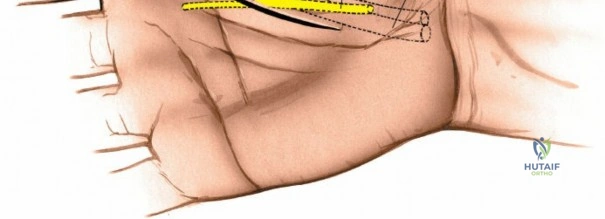
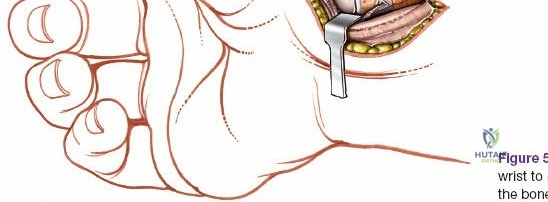
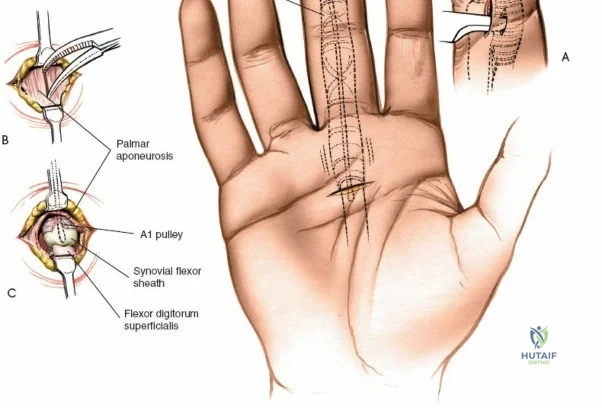
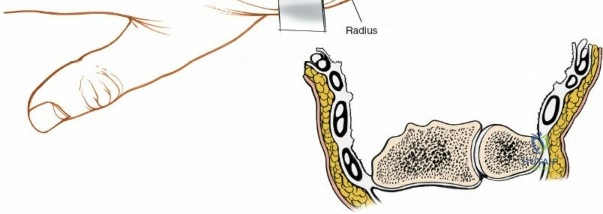
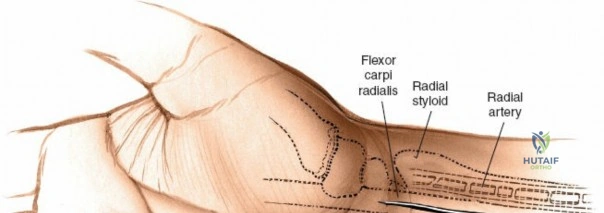
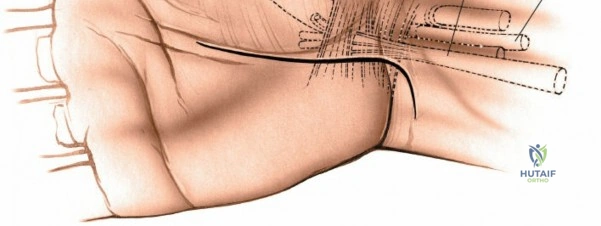
The dorsal approach relies on precise identification of bony landmarks. The surgeon must systematically palpate the radial styloid (the most distal extension of the lateral radius), the ulnar styloid, and Lister's tubercle on the dorsal radius. For a standard dorsal exposure, an 8-cm longitudinal incision is centered over the wrist joint, crossing midway between the radial and ulnar styloids. The incision begins approximately 3 cm proximal to the radiocarpal joint line and extends 5 cm distally over the carpus and proximal metacarpals. Despite crossing a major transverse skin crease at a right angle, the redundant and pliable nature of the dorsal skin prevents the formation of restrictive flexion contractures. In cases of specific pathology, such as an isolated scaphoid fracture or an isolated radial column injury, the incision may be biased radially or curved slightly to accommodate the underlying anatomy.

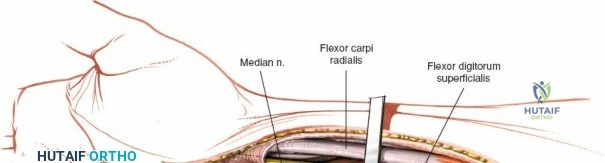
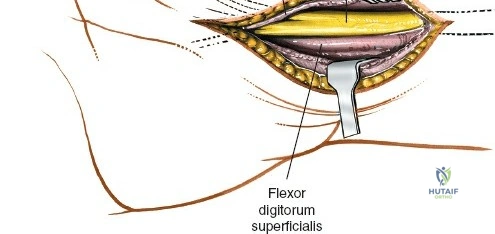
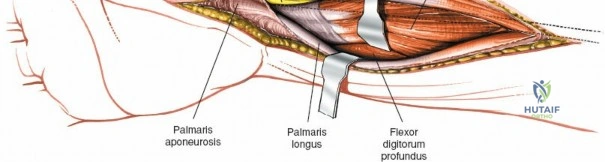
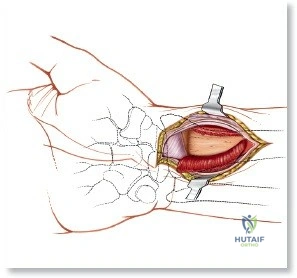
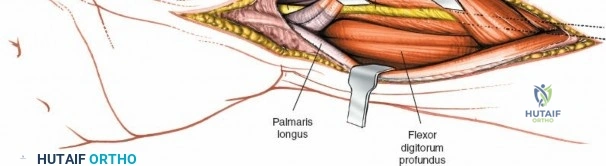
Superficial Dissection and Internervous Planes
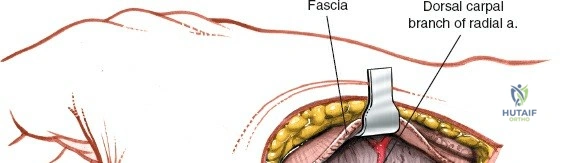
Unique to the dorsal approach to the wrist is the absence of a true internervous plane. The extensor muscles encountered are all innervated by the posterior interosseous nerve (PIN), a branch of the radial nerve. Because the motor branches enter the muscle bellies far proximally in the proximal forearm, the intermuscular planes at the level of the wrist can be developed safely without risk of denervation. The superficial dissection begins by sharply incising the skin and meticulously spreading the subcutaneous fat using blunt dissection to avoid injuring the delicate longitudinal superficial veins and the arborizing branches of the SBRN radially and the DSBUN ulnarly. The subcutaneous tissue is elevated to expose the dense, transverse fibers of the extensor retinaculum, which spans the six dorsal compartments.
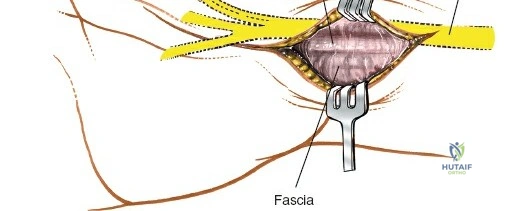
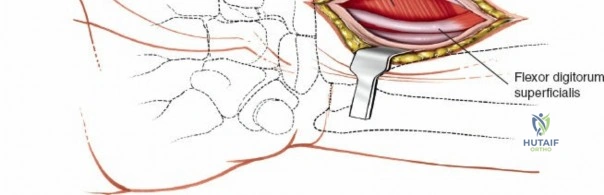
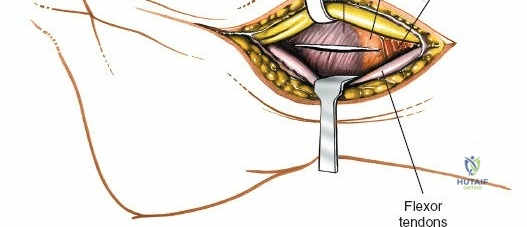
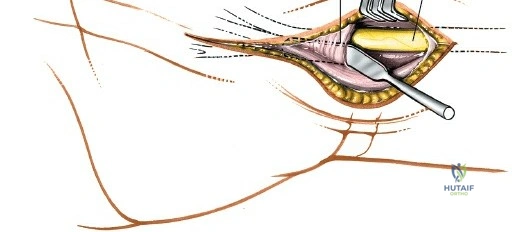
Deep Dissection: Synovectomy and Compartment Management
The deep dissection is entirely tailored to the specific surgical objective. When performing a tenosynovectomy for rheumatoid arthritis, the extensor retinaculum must be managed with care so it can be utilized later to shield the tendons from irregular, eroded bone. The retinaculum is typically incised over the second compartment (ECRL and ECRB). The ulnar edge of the retinaculum is then elevated, and the septa separating the third, fourth, fifth, and sixth compartments are sharply divided, sequentially deroofing the compartments ulnarward. The radial edge is similarly elevated to deroof the first compartment. Following thorough excision of the hypertrophic, invasive tenosynovium, the preserved extensor retinaculum is transposed deep to the extensor tendons, sutured to the joint capsule or periosteum, creating a smooth gliding surface that prevents future attritional tendon ruptures.
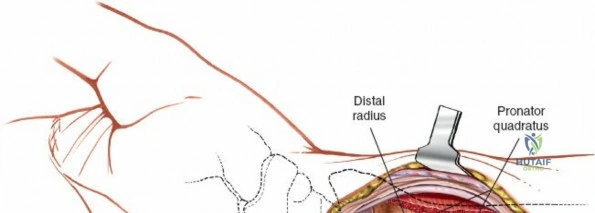
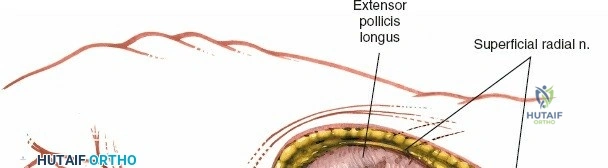
Exposure of the Intermediate and Radial Columns
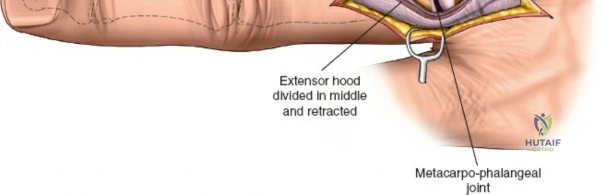
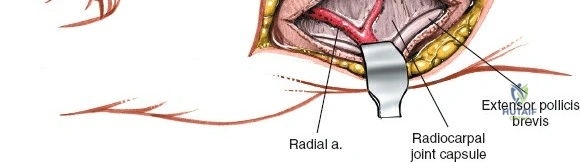
For fracture fixation, the distal radius is conceptualized in three columns: radial, intermediate, and ulnar. To expose the intermediate column, Lister's tubercle is palpated, and the third extensor compartment is opened via an angled incision. The EPL tendon is mobilized from its sheath and retracted radially using a vessel loop. The floor of the third compartment and the intact fourth compartment are then elevated subperiosteally as a single unit, reflecting the EDC and EIP ulnarward. This exposes the broad, flat dorsal surface of the intermediate column, ideal for plate application. If access to the radial column is required, the skin flap is retracted radially. The first compartment is identified, and the retinaculum is incised at the musculotendinous junction of the APL and EPB. Retracting these tendons further radially exposes the radial styloid and the scaphoid fossa, allowing for buttress plating of radial styloid shear fractures.
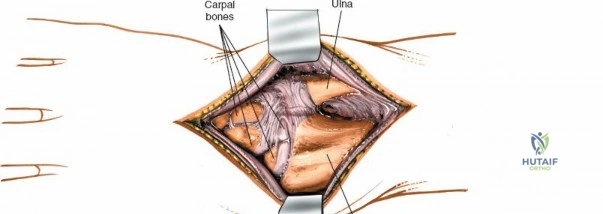
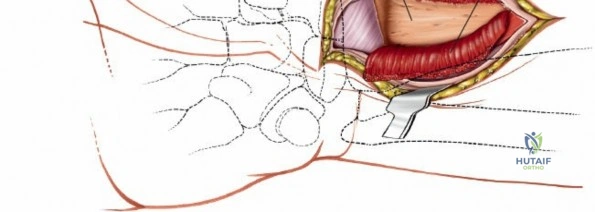
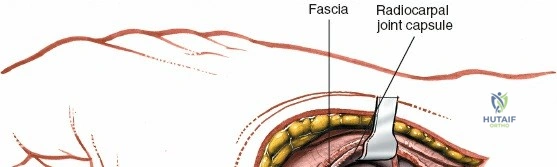
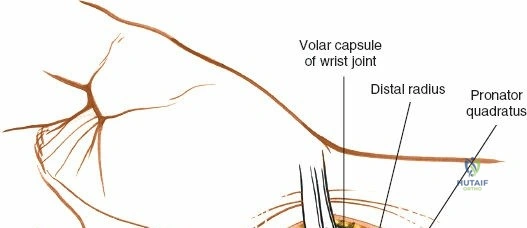
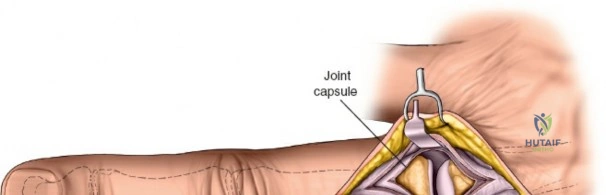
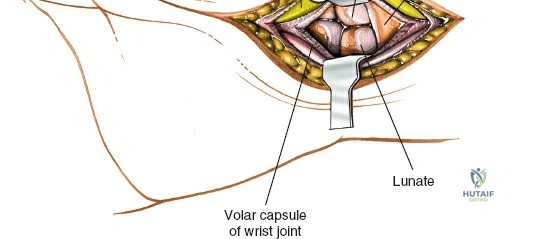
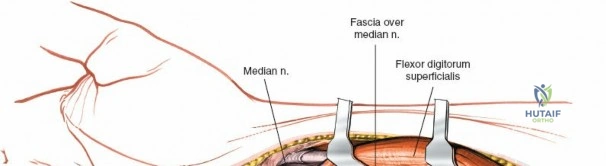
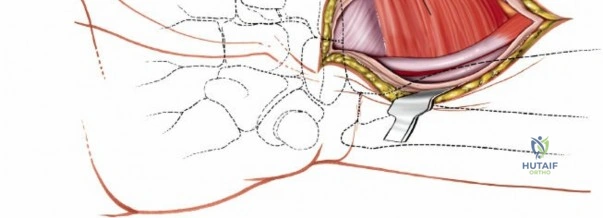
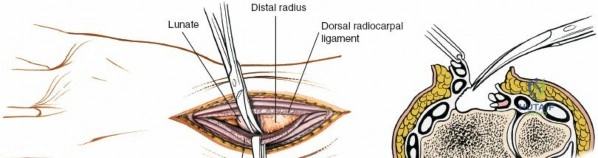
Full Articular Exposure and Capsulotomy
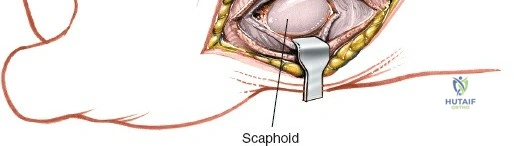
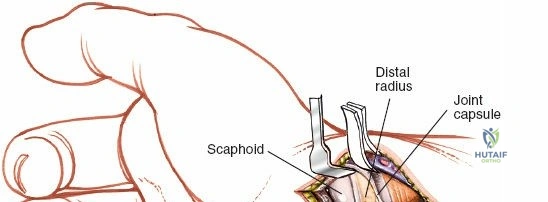
When complete exposure of the radiocarpal and midcarpal joints is necessary—such as in total wrist arthrodesis, proximal row carpectomy, or open reduction of a perilunate dislocation—a more expansile deep dissection is required. The extensor retinaculum is incised over the fourth compartment, and the EDC and EIP tendons are mobilized and retracted. This exposes the dorsal wrist capsule, primarily the robust dorsal radiocarpal ligament. A capsulotomy is performed; historically, a ligament-sparing T-shaped or H-shaped incision is utilized, though a V-shaped flap based distally on the carpus is highly effective for exposing the proximal row. The capsular flaps are elevated subperiosteally from the dorsal rim of the radius and the carpal bones. Retraction of the ECRL and ECRB radially further enhances visualization of the scaphoid and trapezium. Upon completion of the intra-articular procedure, meticulous, watertight closure of the dorsal capsule is imperative to prevent postoperative carpal instability and to provide a barrier between the hardware and the extensor tendons.

Complications, Incidence Rates, and Salvage Management
The dorsal approach to the wrist, while providing unparalleled exposure, is fraught with potential complications, primarily related to the delicate soft tissue envelope and the proximity of the extensor tendons to the bony architecture. The most notorious complication is extensor tendon irritation, tenosynovitis, and eventual attritional rupture, most commonly affecting the EPL tendon. This occurs due to friction against prominent dorsal hardware, inadequate repair of the extensor retinaculum, or ischemic necrosis of the tendon following mobilization. Incidence rates of hardware-related tendon complications in dorsal plating historically approached 20-30%, which catalyzed the modern shift toward volar plating for distal radius fractures. Modern low-profile dorsal plates have reduced this incidence, but meticulous surgical technique remains the primary defense.

Neurologic complications are also significant. Iatrogenic injury to the sensory branches of the radial nerve (SBRN) or the dorsal sensory branch of the ulnar nerve (DSBUN) during superficial dissection can result in debilitating, painful neuromas. The incidence of transient neurapraxia due to aggressive retraction can be as high as 10%. Furthermore, postoperative stiffness is a nearly universal challenge following extensive dorsal capsulotomies, resulting from capsular scarring and loss of the dorsal V-ligamentous compliance. Infections, while relatively rare (1-3%), can be devastating if they penetrate the radiocarpal joint, necessitating emergent operative debridement and targeted intravenous antibiotics.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| EPL Tendon Rupture | 3 - 8% | Retinacular transposition deep to tendon; use of low-profile hardware; avoiding prominent screw tips. | Extensor indicis proprius (EIP) to EPL tendon transfer. |
| SBRN / DSBUN Neuroma | 2 - 5% | Meticulous blunt dissection in subcutaneous fat; gentle retraction with vessel loops; avoiding thermal injury. | Neuroma excision and burying proximal stump into brachioradialis or pronator quadratus muscle belly. |
| Postoperative Stiffness | 15 - 25% | Meticulous capsular repair; rigid internal fixation allowing early active range of motion (ROM). | Intensive occupational therapy; dynamic splinting; late surgical capsulotomy or tenolysis. |
| Hardware Prominence | 10 - 20% | Utilizing modern, low-profile, anatomically contoured titanium plates; countersinking screws. | Elective hardware removal after definitive osseous union (typically 6-12 months post-op). |

Phased Post-Operative Rehabilitation Protocols
Rehabilitation following a dorsal approach to the wrist is highly contingent upon the underlying procedure performed, but generally adheres to a phased protocol designed to balance tissue healing with the prevention of debilitating stiffness. In the immediate post-operative phase (Days 0-14), the primary goals are edema control, pain management, and protection of the surgical repair. The wrist is typically immobilized in a bulky Jones dressing reinforced with a volar plaster splint, positioning the wrist in slight extension (20 degrees) to optimize the resting tension of the flexor and extensor units. Crucially, immediate active range of motion of the digits, elbow, and shoulder is initiated to prevent composite stiffness and promote venous and lymphatic return.
The intermediate phase (Weeks 2-6) begins following suture removal. If rigid internal fixation was achieved (e.g., locked plating of a distal radius fracture), the patient is transitioned to a removable custom thermoplastic splint. Under the guidance of a certified hand therapist, active and active-assisted range of motion exercises for the wrist and forearm (pronation/supination) are commenced. Passive stretching is strictly avoided during this phase to prevent stretching of the dorsal capsular repair or displacement of healing fractures. Modalities such as fluidotherapy and scar massage are introduced to mitigate the formation of restrictive dorsal adhesions.
The advanced phase (Weeks 6-12 and beyond) focuses on progressive strengthening, endurance, and return to functional activities. Radiographic confirmation of osseous union dictates the initiation of progressive resistance exercises using putty, hand grippers, and weighted supination/pronation drills. Dynamic or static progressive splinting may be employed if significant deficits in wrist flexion or extension persist. For patients who underwent salvage procedures such as total wrist arthrodesis, rehabilitation focuses entirely on maximizing digital dexterity and grip strength, as radiocarpal motion is permanently eliminated. Maximum medical improvement is typically not realized until 9 to 12 months post-operatively.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the dorsal approach to the wrist is deeply chronicled in orthopedic literature, reflecting a continuous refinement of technique to mitigate complications while maximizing surgical exposure. Landmark biomechanical studies by Berger et al. elucidated the critical importance of the dorsal radiocarpal and dorsal intercarpal ligaments, establishing the standard for ligament-sparing capsulotomies that preserve carpal kinematics. Their work demonstrated that indiscriminate division of the dorsal capsule leads to profound midcarpal instability and late degenerative changes.
In the realm of trauma, the shift from dorsal to volar plating for distal radius fractures was heavily influenced by the clinical outcome studies of the early 2000s. Authors such as Jupiter and Ring highlighted the unacceptably high rates of extensor tendon tenosynovitis and rupture associated with early generation dorsal Pi-plates. However, subsequent literature by Ruch and others has reaffirmed the absolute necessity of the dorsal approach for specific fracture patterns, notably dorsal shear fractures and highly comminuted intra-articular fractures where volar fixation cannot adequately buttress the dorsal lunate facet. Modern guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) advocate for a pathology-specific approach, reserving the dorsal approach for cases where direct dorsal visualization is mechanically and anatomically mandated.
Furthermore, the management of the rheumatoid wrist remains heavily reliant on the principles established by Millender and Nalebuff in the 1970s. Their seminal papers on dorsal tenosynovectomy and the prophylactic transposition of the extensor retinaculum remain the gold standard for preventing the devastating cascade of extensor tendon ruptures. Contemporary long-term outcome studies continue to validate their techniques, demonstrating that timely dorsal synovectomy not only preserves tendon integrity but also significantly delays the progression of radiocarpal destruction, underscoring the enduring relevance of the dorsal approach in modern orthopedic surgery.
Clinical & Radiographic Imaging Archive