Fractional Lengthening of the Flexor Carpi Radialis and Finger Flexors
Key Takeaway
Fractional lengthening of the flexor carpi radialis and finger flexors is a cornerstone surgical intervention for managing spastic flexion contractures of the wrist and hand. By selectively dividing the aponeurosis while preserving the underlying muscle fibers, surgeons can achieve controlled elongation of the muscle-tendon unit. This guide details the biomechanical principles, step-by-step surgical approaches, and postoperative protocols necessary to optimize functional outcomes and prevent recurrence.
Comprehensive Introduction and Patho-Epidemiology
Spastic flexion contractures of the wrist and fingers represent a profound source of functional impairment, hygienic difficulty, and cosmetic deformity in patients afflicted with upper motor neuron syndromes. Conditions such as cerebral palsy, traumatic brain injury, severe cervical myelopathy, and post-stroke spastic hemiplegia frequently culminate in a predictable pattern of upper extremity dysfunction. The flexor carpi radialis (FCR), flexor digitorum superficialis (FDS), and flexor digitorum profundus (FDP) are the primary anatomical structures implicated in these debilitating deformities. The pathophysiology begins as a dynamic state of hypertonia, driven by the loss of descending cortical inhibition to the alpha and gamma motor neurons, leading to an exaggerated stretch reflex and sustained muscular contraction.
Over time, this relentless dynamic spasticity transitions into a fixed myostatic contracture. At the cellular and molecular level, the chronically shortened muscle undergoes profound phenotypic alterations. There is a documented loss of serial sarcomeres, an increase in the ratio of collagen to muscle fibers, and a thickening of the extracellular matrix. The rheological properties of the muscle-tendon unit are fundamentally altered, rendering the tissue inelastic and fibrotic. Once this structural shortening occurs, conservative measures—including aggressive orthotic management, physical therapy, serial casting, and targeted botulinum toxin injections—lose their efficacy. At this critical inflection point, surgical intervention becomes an absolute necessity to restore biomechanical balance and prevent secondary joint ankylosis, skin maceration, and profound functional loss.
Historically, surgeons relied on traditional Z-lengthening (step-cut lengthening) of the flexor tendons to correct these deformities. However, Z-lengthening often yields unpredictable results, frequently leading to profound iatrogenic weakness, extensive peritendinous adhesion formation, and the devastating complication of over-lengthening, which creates an uncorrectable extension deformity. In stark contrast, fractional lengthening (fractional recession) and the more extensive proximal flexor slide (the Inglis and Cooper technique) have emerged as the gold-standard, evidence-based techniques. These procedures are meticulously designed to restore the biomechanical balance of the wrist and hand while preserving the intrinsic continuity and functional strength of the musculotendinous units.
The epidemiological burden of spastic upper extremity contractures is substantial. In the post-stroke population, it is estimated that up to 30% to 40% of survivors will develop some degree of spasticity, with a significant cohort progressing to fixed contractures if not aggressively managed. Similarly, in the cerebral palsy population, particularly those with spastic hemiplegia or quadriplegia, upper extremity involvement is nearly ubiquitous. The societal and individual costs associated with loss of independence, the need for continuous caregiver assistance for basic hygiene (such as cleaning the palmar crease to prevent fungal infections and skin breakdown), and the psychological impact of the deformity underscore the critical importance of mastering these advanced surgical lengthening techniques.
Detailed Surgical Anatomy and Biomechanics
The success of fractional lengthening is unequivocally predicated on a profound understanding of the unique microanatomy and fascial architecture of the forearm flexors. The flexor-pronator mass originates from the medial epicondyle of the humerus and the proximal ulna, transitioning into distinct muscle bellies in the proximal and middle thirds of the forearm. The critical anatomical feature utilized in fractional lengthening is the relationship between the muscle fibers and their investing fascia. The distal portion of the muscle belly in these units is enveloped by a dense, inelastic aponeurosis that progressively thickens distally to form the true tendinous insertion. This aponeurotic sleeve acts as a mechanical constraint, dictating the resting length of the muscle-tendon unit.
Biomechanically, fractional lengthening exploits this anatomical arrangement by strategically dividing the aponeurosis while meticulously preserving the underlying muscle fibers. By making a transverse incision exclusively through this aponeurotic fascia—proximal to the true musculotendinous junction—the surgeon releases the inelastic fibrous constraint. When passive tension (such as dorsiflexion of the wrist or extension of the digits) is subsequently applied, the underlying elastic muscle fibers stretch, causing the edges of the incised aponeurosis to separate. This creates a controlled "gap" that effectively lengthens the entire unit. Because the muscle fibers themselves remain in continuity, the sarcomere length-tension curve is shifted but not destroyed, thereby preserving the muscle's inherent tension-generating capacity.
For patients requiring the more extensive proximal flexor slide, the surgical anatomy shifts to the medial aspect of the elbow. The flexor-pronator origin is a complex confluence of tendinous insertions anchoring the pronator teres, FCR, palmaris longus (PL), flexor carpi ulnaris (FCU), and FDS to the medial epicondyle. Deep to this superficial group lies the FDP, originating from the proximal ulna and interosseous membrane. The biomechanical principle of the flexor slide involves the complete detachment of this origin, allowing the entire muscle mass to migrate distally. This distal slide effectively lengthens the muscle-tendon units without requiring distal incisions, making it exceptionally powerful for severe, global flexion-pronation contractures.
Crucial neurovascular relationships must be respected during these procedures. In the distal forearm, the palmar cutaneous branch of the median nerve lies in the superficial subcutaneous tissue between the FCR and PL, making it highly vulnerable during the standard volar incision. Deep to the FDS and superficial to the FDP lies the median nerve itself, accompanied by the anterior interosseous artery and nerve deeper still. Proximally, at the medial epicondyle, the ulnar nerve resides within the cubital tunnel, tethered by Osborne's ligament and the arcuate ligament of the FCU. Any proximal slide of the flexor mass will invariably place traction on the ulnar nerve unless it is completely released and anteriorly transposed, highlighting the intricate interplay between soft tissue balancing and peripheral nerve protection.
Exhaustive Indications and Contraindications
Thorough preoperative assessment is critical to differentiate between dynamic spasticity and fixed myostatic contracture, as this distinction dictates the entire treatment algorithm. Dynamic spasticity is characterized by increased tone that yields to slow, sustained passive stretching; it is often responsive to chemodenervation (Botox), oral antispasmodics, and rigorous splinting. Conversely, a fixed contracture is characterized by structural shortening of the muscle-tendon unit and joint capsule, which absolutely does not yield to passive stretching. This structural shortening is the primary and definitive indication for surgical lengthening. Surgeons must carefully evaluate the contribution of each muscle group using precise clinical metrics.
The Volkmann angle—defined as the specific angle of wrist flexion at which the fingers can be fully extended passively—must be meticulously measured to quantify the severity of the flexor tightness. If the fingers can only be extended when the wrist is flexed beyond 60 degrees, a severe contracture is present. Diagnostic nerve blocks (e.g., median or ulnar nerve blocks at the elbow utilizing bupivacaine) are invaluable adjuncts; they temporarily abolish dynamic spasticity, thereby unmasking the true extent of the underlying fixed contracture. Fractional lengthening is generally indicated for mild to moderate contractures where some voluntary motor control is preserved, and the goal is to enhance hand function or facilitate orthotic wear.
The proximal flexor slide is reserved for the most severe, recalcitrant cases. Indications include global spastic flexion contractures of the wrist and all digits, typically accompanied by a severe pronation deformity, where the Volkmann angle is exceptionally poor. These are often "hygiene-only" hands, where the primary goal is to open the palm to prevent skin maceration, recurrent infections, and pain, rather than to restore fine motor function. The flexor slide provides a massive, simultaneous release of all involved units, achieving a degree of lengthening that distal fractional techniques simply cannot match.
Contraindications must be rigorously respected to prevent catastrophic functional decline. Purely dynamic spasticity without fixed contracture is a strict contraindication to surgical lengthening, as it will likely result in profound weakness once the spasticity fluctuates or resolves. Furthermore, patients with profound extrapyramidal movement disorders, such as severe athetoid or dystonic cerebral palsy, are poor candidates; the unpredictable nature of their muscle tone often leads to rapid recurrence or reversal of the deformity (e.g., converting a flexion contracture into a severe extension deformity). Severe, fixed bony ankylosis of the wrist or small joints of the hand also contraindicates isolated soft tissue lengthening, necessitating osseous procedures such as proximal row carpectomy and total wrist arthrodesis instead.
| Parameter | Indications for Surgical Lengthening | Contraindications for Surgical Lengthening |
|---|---|---|
| Pathology Type | Fixed myostatic contracture unresponsive to therapy | Purely dynamic spasticity yielding to passive stretch |
| Volkmann Angle | Positive (fingers extend only with wrist flexion) | Negative (fingers extend fully with wrist in neutral) |
| Diagnostic Block | Residual contracture remains after nerve block | Complete resolution of contracture after nerve block |
| Neurologic Profile | Stable upper motor neuron lesion (Stroke, CP) | Progressive neurodegenerative disease; Severe Athetosis/Dystonia |
| Joint Status | Supple articular surfaces and joint capsules | Severe fixed bony ankylosis or advanced degenerative arthropathy |
| Patient Goals | Improved hygiene, orthotic tolerance, functional grasp | Unrealistic expectations of normal fine motor restoration |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for fractional lengthening and flexor slides requires a meticulous, multi-tiered approach that evaluates not only the flexor pathology but also the capacity of the antagonist extensors. The Zancolli classification of the spastic hand is frequently employed to categorize the severity of the deformity and guide surgical decision-making. A Zancolli Group I patient has active finger extension with the wrist in neutral, whereas a Group III patient has no active finger extension even with maximal wrist flexion. This classification helps the surgeon determine whether isolated lengthening is sufficient or if concomitant procedures, such as tendon transfers (e.g., FCU to EDC) or joint stabilizations, are required to augment extensor power once the flexors are released.
Electromyography (EMG) and dynamic motion analysis can provide invaluable objective data regarding muscle firing patterns, phase-appropriate activity, and the presence of co-contraction. In complex cases, fine-wire EMG during functional tasks can differentiate between muscles that are continuously firing due to spasticity and those that retain some degree of voluntary, phase-specific control. This distinction is critical; muscles with preserved voluntary control should be fractionally lengthened to preserve their function, whereas non-functional, severely spastic muscles may be candidates for complete tenotomy or transfer out of their deforming positions.
Patient positioning is critical for optimal surgical exposure and intraoperative assessment. The patient is placed supine on the operating table with the affected upper extremity extended on a radiolucent, well-padded hand table. A pneumatic tourniquet is applied to the proximal arm. Exsanguination is typically performed using an Esmarch bandage; however, in cases of extreme spasticity where the limb cannot be fully extended, gravity drainage for 3 to 5 minutes prior to tourniquet inflation may be necessary. The tourniquet is inflated to the appropriate pressure (typically 250 mm Hg or 100 mm Hg above the patient's systolic blood pressure). Loupe magnification (2.5x to 3.5x) and a headlight are highly recommended to ensure precise identification of the aponeurosis, fascial septa, and protection of adjacent micro-neurovascular structures.
Anesthetic considerations are paramount in these procedures. General anesthesia is typically preferred to ensure complete patient immobility and comfort. However, the anesthesiologist must be explicitly instructed to avoid the use of long-acting neuromuscular blocking agents (paralytics) after the initial intubation sequence. The surgical technique relies heavily on the surgeon's ability to assess the resting tension of the muscle-tendon units and observe the passive "slide" of the aponeurosis. Complete chemical paralysis will artificially lower the resting tone of the muscles, potentially leading to an underestimation of the contracture severity and resulting in inadequate surgical lengthening.
Step-by-Step Surgical Approach and Fixation Technique
Fractional Lengthening of the FCR and Finger Flexors
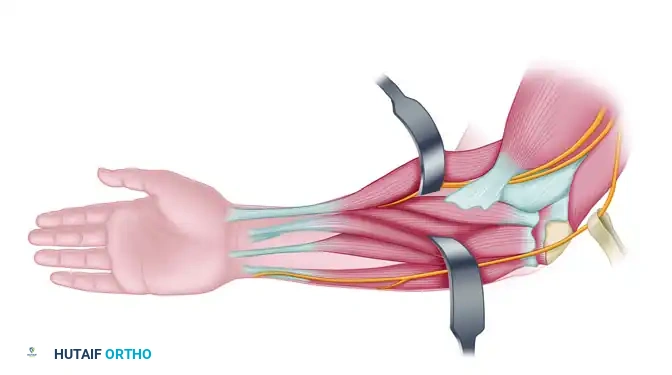
The incision for fractional lengthening is meticulously designed to avoid restrictive scarring. Begin by designing a curved volar incision over the distal forearm, starting approximately 3 cm proximal to the volar wrist crease and extending proximally for about 6 cm. A slightly curved or lazy-S incision is mandatory to prevent the formation of a linear scar contracture across the flexion crease of the forearm. Dissect through the subcutaneous tissue, utilizing bipolar electrocautery for hemostasis. Meticulous care must be taken to identify, isolate with a vessel loop, and retract the palmar cutaneous branch of the median nerve, which typically lies in the subcutaneous fat between the FCR and the palmaris longus (PL).
Once the superficial fascia is incised, identify the flexor carpi radialis (FCR) muscle. Trace the FCR proximally from its tendinous portion at the wrist up to the musculotendinous junction, continuing further proximally until the distinct, fleshy muscle belly is fully visualized. The distal portion of the muscle belly is surrounded by a distinct, silvery aponeurosis that thickens distally. Completely identify the FCR muscle circumferentially. Use a blunt instrument, such as a Freer elevator or a right-angle forceps, to gently separate the muscle from the underlying structures, ensuring no neurovascular elements are tethered to the deep surface of the muscle.
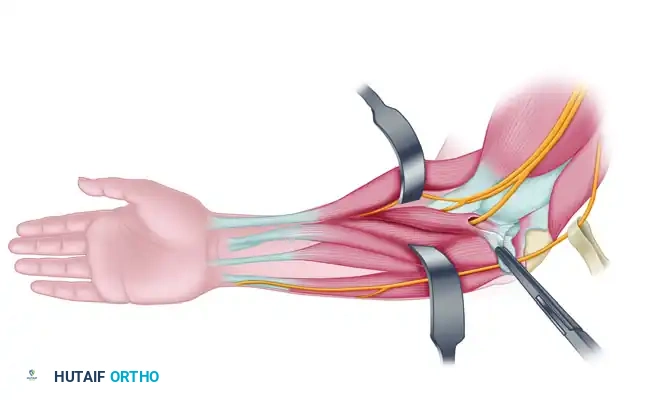
Make a precise transverse cut through the aponeurosis proximal to the musculotendinous junction using a scalpel (typically a #15 blade). The surgeon must cut only through the aponeurosis and not through the underlying red muscle fibers. However, it is equally critical to divide the aponeurosis completely from medial to lateral edge. If even a 1 mm band of the tendinous aponeurosis is left intact, the muscle-tendon unit will fail to lengthen. After the transverse cut is completed, passively place the wrist into maximal dorsiflexion. Observe the transverse cut in the aponeurosis widen, creating a V-shaped gap. If the desired length is not achieved, a second transverse cut (recession) may be made approximately 1.5 to 2 cm proximal to the first cut. This process is subsequently repeated for the FDS and, if necessary, the FDP, working from superficial to deep while rigorously protecting the median nerve.
The Flexor Slide (Inglis and Cooper Technique)
For severe, global spastic flexion contractures, the proximal flexor slide is executed. Begin the incision on the medial aspect of the volar side of the arm, starting approximately 5 cm proximal to the medial epicondyle. Continue the incision distally, crossing the elbow joint, to the midpoint of the forearm over the ulna.
Elevate thick fasciocutaneous flaps to expose the medial epicondyle, the cubital tunnel, and the proximal flexor-pronator mass. The ulnar nerve must be identified early in the procedure to prevent catastrophic iatrogenic injury. Locate the nerve proximal to the cubital tunnel and trace it distally. Release the ulnar nerve completely from the cubital tunnel by dividing the Osborne ligament and the arcuate ligament of the flexor carpi ulnaris (FCU). The nerve must be meticulously neurolysed and protected with a vessel loop throughout the entirety of the release.

With the ulnar nerve protected, direct attention to the medial epicondyle. Sharply incise the tendinous origins of the flexor-pronator muscles directly off the bone. The flexor carpi ulnaris (FCU) and the flexor digitorum profundus (FDP) muscles must be completely released from their origins on the medial epicondyle and the proximal ulna.
Use a periosteal elevator to strip the muscle origins distally. To ensure a complete and unhindered slide of the muscle mass, the lacertus fibrosus (bicipital aponeurosis) must be divided. Once the flexor mass has been allowed to slide distally, the ulnar nerve will be under tension if left in its anatomical bed. Therefore, the ulnar nerve must be transposed anteriorly into a well-vascularized subcutaneous bed to prevent traction neuritis. Extend the wrist and fingers to confirm that the flexor mass slides distally by the required amount (often 3 to 4 cm) and that the contracture is fully resolved. Closure involves meticulous hemostasis, placement of a closed suction drain if dead space is significant, and layered closure of the subcutaneous tissue and skin.
Complications, Incidence Rates, and Salvage Management
While fractional lengthening and flexor slides are highly effective, they carry specific surgical risks that the orthopaedic surgeon must actively mitigate. Intraoperative complications primarily involve iatrogenic nerve injury. The palmar cutaneous branch of the median nerve is at the highest risk during the volar forearm incision for fractional lengthening. Injury to this nerve results in painful neuromas and debilitating dysesthesias over the base of the thenar eminence. During the flexor slide, failure to adequately decompress and anteriorly transpose the ulnar nerve will almost certainly result in traction neuritis as the muscle mass shifts distally, leading to delayed-onset cubital tunnel syndrome and intrinsic hand weakness.
Inadequate lengthening is a frequent technical error, particularly among less experienced surgeons. This occurs if the aponeurosis is not completely divided from edge to edge during fractional lengthening. The fascial sleeve is remarkably strong; even a microscopic intact band will prevent the muscle from sliding, resulting in a persistent contracture postoperatively. Conversely, over-lengthening is a devastating complication that results from cutting too deeply into the muscle belly during fractional lengthening (severing the continuity of the muscle fibers) or stripping the flexor origin too far distally during a flexor slide. This results in a profound loss of grip strength and the potential development of an iatrogenic extension deformity, which is exceptionally difficult to salvage.
The most common long-term complication is the recurrence of the flexion contracture. This is almost exclusively due to non-compliance with the prolonged postoperative splinting protocol. The newly formed scar tissue within the aponeurotic gap is highly susceptible to the continuous resting tone of the spastic muscle. If not mechanically braced, this immature scar will contract, pulling the muscle back to its original shortened length. Incidence rates of recurrence can approach 20-30% in highly non-compliant patient populations.
Salvage management for failed fractional lengthening or flexor slides is highly complex. For recurrent contractures, revision fractional lengthening is rarely successful due to extensive perimuscular scarring and loss of the distinct aponeurotic anatomy. Salvage options include complete tenotomies (for non-functional, hygiene-only hands), superficialis-to-profundus (STP) tendon transfers, or osseous procedures. Proximal row carpectomy combined with total wrist arthrodesis is the ultimate salvage procedure, providing relative lengthening of the flexor tendons by shortening the skeletal column, thereby restoring the wrist to a neutral, stable position and facilitating hygiene.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Recurrence of Contracture | 15% - 30% | Strict adherence to 6-month night splinting protocol | Serial casting; Salvage tenotomies; Wrist arthrodesis |
| Inadequate Lengthening | 5% - 10% | Complete edge-to-edge transection of the aponeurosis | Revision release; STP transfer |
| Over-Lengthening / Weakness | 2% - 5% | Avoid cutting muscle fibers; controlled passive stretch | Tenodesis; Extensor-to-flexor tendon transfers |
| Palmar Cutaneous Nerve Injury | 1% - 3% | Careful subcutaneous dissection; loupe magnification | Neuroma excision and proximal burying into muscle |
| Ulnar Traction Neuritis | < 2% (if transposed) | Mandatory anterior transposition during flexor slide | Revision neurolysis and submuscular transposition |
Phased Post-Operative Rehabilitation Protocols
The surgical execution of a fractional lengthening or flexor slide represents only the first half of the therapeutic equation; the ultimate success of the procedure is heavily dependent on rigorous, well-managed postoperative care. The newly lengthened muscle-tendon units rely on the formation of organized, resilient scar tissue within the aponeurotic gaps. This tissue is highly vulnerable to rupture if aggressively stretched too early, or to recurrent contracture if not properly splinted during the maturation phase. Rehabilitation is therefore divided into three distinct, highly structured phases.
Phase I: Immobilization (Weeks 0 to 4)
Immediately postoperatively, the limb is placed in a well-padded, rigid palmar (volar) short-arm splint. If a proximal flexor slide was performed, a long-arm splint or cast is mandatory to protect the elbow and the transposed ulnar nerve. The wrist is positioned in a neutral position or slightly extended (10 to 15 degrees of dorsiflexion), and the fingers are placed in functional extension. Crucial Note: The surgeon must avoid extreme hyperextension during this initial casting phase. Forcing the wrist and fingers into maximal extension places excessive tension on the healing aponeurotic gaps, leading to micro-ruptures of the muscle fibers, severe postoperative pain, and excessive hematoma formation. This rigid immobilization is maintained continuously for 3 to 4 weeks to allow the aponeurotic gaps to fill with organized fibrovascular scar tissue.
Phase II: Mobilization and Protection (Weeks 4 to 8)
At the 3- to 4-week mark, the rigid surgical splint or cast is removed. The patient is immediately transitioned into the care of a specialized hand therapist. A custom-molded removable thermoplastic splint is fabricated. This splint is worn at all times for protection, except during designated therapy sessions and hygiene routines. Active and active-assisted mobilization of the wrist and digits is initiated. Therapy focuses on tendon gliding exercises to prevent peritendinous adhesions, maintaining the newly acquired extension, and, critically, re-educating the antagonist extensor muscles. The wrist and finger extensors are often profoundly weak due to prolonged preoperative overstretching and reciprocal inhibition; targeted neuromuscular electrical stimulation (NMES) may be utilized to facilitate extensor activation.
Phase III: Long-Term Maintenance (Months 2 to 6+)
As active motor control and dynamic balance improve, daytime splinting is gradually weaned. However, a volar short-arm night splint must be utilized for an additional 4 to 6 months minimum. Night splinting is absolutely critical and non-negotiable. During sleep, the resting tone of the flexors remains elevated due to the underlying upper motor neuron syndrome. This continuous nocturnal tension can cause the immature, remodeling scar tissue at the lengthening sites to contract, leading to a rapid and devastating recurrence of the deformity. Caregiver education regarding the importance of the night splint is paramount, as compliance is the single greatest determinant of long-term success.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for the spastic upper extremity is deeply rooted in landmark orthopedic literature. The proximal flexor slide was originally popularized by Inglis and Cooper in the mid-20th century. Their seminal work demonstrated that releasing the entire flexor-pronator mass from the medial epicondyle could salvage severely contracted, non-functional hands that were previously deemed untreatable. While the Inglis and Cooper technique remains a powerful tool in the surgeon's armamentarium, its use is now generally reserved for the most severe cases due to the extensive dissection required and the risk of profound postoperative weakness.
The paradigm shift toward fractional lengthening was heavily influenced by the work of Eduardo Zancolli and others, who meticulously detailed the fascial anatomy of the forearm and the biomechanical advantages of preserving muscle continuity. Comparative outcome studies over the past two decades have consistently demonstrated the superiority of fractional lengthening over traditional Z-plasty step-cut lengthening. Literature indicates that fractional lengthening provides a more predictable increase in length, significantly reduces the incidence of iatrogenic over-lengthening, and, most importantly, preserves a greater percentage of preoperative grip strength. This preservation of power is critical for patients who rely on their affected extremity for assistive grasp and transfer activities.
Modern clinical guidelines emphasize a comprehensive, multidisciplinary approach to the spastic upper extremity. Guidelines published by the American Society for Surgery of the Hand (ASSH) and the American Academy of Orthopaedic Surgeons (AAOS) stress that fractional lengthening should rarely be performed in isolation. Concomitant deformities must be addressed simultaneously to achieve a balanced extremity. For example, the thumb-in-palm deformity—driven by spasticity of the adductor pollicis, flexor pollicis brevis, and flexor pollicis longus—must be concurrently released or lengthened to prevent the fingers from trapping the thumb postoperatively. Similarly, severe pronation contractures may require pronator teres tenotomy or rerouting.
Future directions in the management of spastic contractures involve the integration of advanced technologies. High-resolution ultrasound is increasingly being used preoperatively to quantify muscle echogenicity and fascial thickness, helping surgeons predict which muscles will respond best to fractional lengthening versus complete tenotomy. Furthermore, the integration of targeted muscle reinnervation (TMR) concepts and highly selective neurectomies are being investigated as adjuncts to soft tissue lengthening, aiming to permanently downregulate the spastic drive to the flexors while preserving the architectural integrity of the muscle.
