Masterclass: Comprehensive Spring Ligament Reconstruction for Adult Acquired Flatfoot Deformity

Key Takeaway
This masterclass provides an exhaustive, real-time guide to spring ligament reconstruction. Fellows will learn intricate anatomy, meticulous preoperative planning, and precise intraoperative execution, including graft selection, tunnel creation, and fixation techniques. We cover primary repair, superomedial, and inferior reconstructions, emphasizing pearls, pitfalls, and postoperative care for adult acquired flatfoot deformity, ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows and colleagues, to this definitive masterclass on the surgical management of the medial longitudinal arch. Today, we are undertaking a critical and highly nuanced component of adult acquired flatfoot deformity (AAFD), increasingly referred to in contemporary literature as Progressive Collapsing Foot Deformity (PCFD): Spring Ligament Reconstruction. This intervention transcends simple soft-tissue repair; it is a meticulous, biomechanically driven restoration of a complex anatomical structure that serves as the primary static stabilizer of the medial arch. Our overarching objective is to provide a stable, functional, and plantigrade foot by correcting the progressive peritalar subluxation at the talonavicular joint that serves as the hallmark of this debilitating condition.
Let us begin by dissecting the fundamental patho-epidemiology. The spring ligament complex, anatomically defined as the plantar calcaneonavicular ligament, is subjected to immense physiological loads during the stance phase of the gait cycle. Its failure—whether through insidious lengthening, myxoid degeneration, chronic attenuation, or outright traumatic disruption—precipitates a predictable cascade of biomechanical consequences. The most common culprit is the repetitive, cumulative stress associated with a pre-existing pes planovalgus morphology. This chronic strain places disproportionate load on the medial ligamentous constraints, leading to a progressive failure of the collagen matrix. One can conceptualize this process as a high-tension cable fraying progressively under relentless cyclical loading.
This structural degeneration frequently manifests as longitudinal interstitial tears, massive full-thickness defects, or profound plastic deformation. While acute, isolated traumatic ruptures of the spring ligament can occur (often secondary to high-energy athletic injuries involving forced eversion and dorsiflexion), it is exponentially more common to encounter this failure paradigm within the context of a chronically degenerated ligament. This underlying vulnerability is frequently exacerbated by an acute-on-chronic episode, prompting the patient to seek surgical consultation. The epidemiological profile typically features middle-aged to older adults, with a higher prevalence in females, often compounded by systemic comorbidities such as obesity, hypertension, and diabetes mellitus, which further compromise microvascular perfusion to the tendon and ligamentous footprint.
The ultimate consequence of this failure is progressive, multiplanar peritalar deformity. The foot essentially "collapses out" from beneath the talar head. Kinematically, the talar head plantarflexes and medially rotates, migrating dorsally and laterally relative to the navicular articular surface. Conversely, the navicular, calcaneus, and the distal pedal segments abduct and translate plantarly and medially in relation to the talus. This uncoupling of the acetabulum pedis creates the classic clinical presentation: the "too many toes" sign, profound flattening of the medial longitudinal arch, and hindfoot valgus. It is imperative to recognize that spring ligament failure almost universally coexists with posterior tibial tendon insufficiency (PTTI). Regardless of the primary etiology, failure of the spring ligament complex invariably places the patient at extreme risk for exponential talonavicular subluxation; once this subluxation initiates, progression is virtually inevitable without decisive surgical reconstruction.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever passed to the skin, a profound, three-dimensional understanding of the medial pedal anatomy is absolute paramount. The spring ligament is a misnomer if considered singular; it is a robust, multifaceted ligamentous complex comprising distinct anatomical bands with specific biomechanical roles. Recognizing the unique contributions of these components is the foundation of anatomical reconstruction.
The Superomedial and Inferior Ligamentous Bands
The spring ligament complex is primarily divided into two major functional bands. The Superomedial Portion (Medial Calcaneonavicular Ligament) originates from the superomedial aspect of the sustentaculum tali and the anterior facet of the calcaneus. It traverses anteriorly to insert broadly onto the medial aspect of the navicular, intimately adjacent to its articular surface. This band lies immediately deep and medial to the posterior tibial tendon, serving as a critical sling. It also blends inextricably with the superficial anterior deltoid ligament (the tibiospring ligament), forming a continuous capsuloligamentous sheet. Biomechanically, the superomedial band is the primary restraint against medial and plantar migration of the talar head.
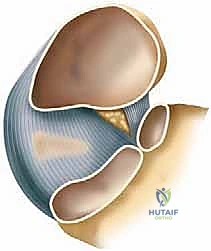
The Inferior Portion (Plantar Calcaneonavicular Ligament) originates from the distinct notch located between the anterior and medial calcaneal articular facets. It courses distally to insert onto the inferior surface of the midnavicular, positioned just lateral to the insertion footprint of the superomedial portion. This inferior band is thicker, more fibrocartilaginous, and functions primarily to resist plantar-directed forces exerted by the talar head during weight-bearing.
Understanding which portion is primarily attenuated or ruptured dictates our reconstructive vector. In advanced PCFD, the talar head migrates both medially and plantarly, signifying the catastrophic failure of both the superomedial and inferior components. A successful reconstruction must therefore recreate the tension and vector of both bands to effectively contain the talar head within the acetabulum pedis.
Neurovascular Topography and Intermuscular Intervals
Navigating the medial approach requires meticulous, atraumatic dissection to preserve vital neurovascular structures. The Posterior Tibial Tendon (PTT) serves as our primary superficial landmark. It courses directly superficial and lateral to the superomedial spring ligament. Retraction of the PTT is required to expose the underlying ligamentous complex, but this must be done delicately to preserve its blood supply, particularly if a primary repair or augmentation of the tendon is planned.
Deep and slightly posterior to the PTT lie the Flexor Digitorum Longus (FDL) and Flexor Hallucis Longus (FHL) tendons. The critical Medial Plantar Neurovascular Bundle, comprising the medial plantar nerve and artery, traverses deep to the fascial layer of the abductor hallucis, running along the plantar aspect of the foot. Extreme caution is mandated during dissection around the inferior aspect of the sustentaculum tali and the plantar navicular to avoid catastrophic iatrogenic injury to this bundle. Furthermore, the Saphenous Nerve and Vein cross the medial malleolus superficially; these must be identified, mobilized, and protected during the initial skin incision to prevent painful postoperative neuromas.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful spring ligament reconstruction. The decision to proceed with operative intervention hinges on a meticulous clinical evaluation, correlating patient symptomatology with objective signs of progressive deformity and functional deficit. Not every flatfoot requires a scalpel; however, a collapsing foot with a compromised static medial restraint demands decisive action.
Clinical Assessment and Decision Making
Patients typically present with insidious, aching medial foot pain, localized along the course of the PTT and the talonavicular joint. In advanced stages, as the deformity progresses, patients frequently develop lateral hindfoot pain secondary to subfibular impingement or calcaneocuboid abutment. A comprehensive physical examination must include a thorough assessment of the medial longitudinal arch in a weight-bearing stance, quantifying the degree of collapse, hindfoot valgus, and forefoot abduction.
The Single-Leg Heel Rise Test is the pathognomonic clinical assay for PTT and spring ligament integrity. An inability to initiate or maintain a single-leg heel rise, or the absence of physiologic hindfoot inversion during the maneuver, indicates profound insufficiency of the medial dynamic and static stabilizers. Range of motion (ROM) of the subtalar and transverse tarsal joints must be critically evaluated. The deformity must be passively correctable (supple). A rigid, fixed deformity represents an absolute contraindication to soft-tissue reconstruction alone and mandates arthrodesis. Finally, the Silfverskiold test is mandatory to assess for concomitant gastrocnemius or Achilles contracture, which, if left unaddressed, will subject any medial reconstruction to catastrophic failure due to unopposed equinus forces.
Indications and Contraindications Matrix
| Parameter | Surgical Indications | Surgical Contraindications |
|---|---|---|
| Deformity Status | Progressive, symptomatic flatfoot deformity failing conservative care (custom orthotics, AFOs). | Rigid, fixed, non-reducible hindfoot or midfoot deformity. |
| Ligament Pathology | MRI or clinically evident high-grade partial tears, complete ruptures, or severe attenuation of the spring ligament. | Isolated, mild PTT tenosynovitis without static ligamentous incompetence or arch collapse. |
| Joint Integrity | Supple peritalar joints (subtalar, talonavicular, calcaneocuboid) with preserved articular cartilage. | Advanced osteoarthritis of the subtalar, talonavicular, or calcaneocuboid joints (mandates arthrodesis). |
| Neuromuscular | Intact neurological function and adequate muscular control of the lower extremity. | Charcot neuroarthropathy, severe peripheral neuropathy, or active spasticity. |
| Patient Factors | Medically optimized patient capable of adhering to strict, prolonged non-weight-bearing rehabilitation protocols. | Uncontrolled diabetes mellitus, severe peripheral vascular disease, active infection, or non-compliance. |
Pre-Operative Planning, Templating, and Patient Positioning
Surgical execution is merely the final manifestation of exhaustive preoperative planning. Our strategy incorporates advanced imaging modalities to quantify the deformity in multiple planes, allowing for the precise selection of concomitant bony procedures (osteotomies) that are universally required to protect the soft-tissue reconstruction.
Radiographic Analysis and Advanced Imaging
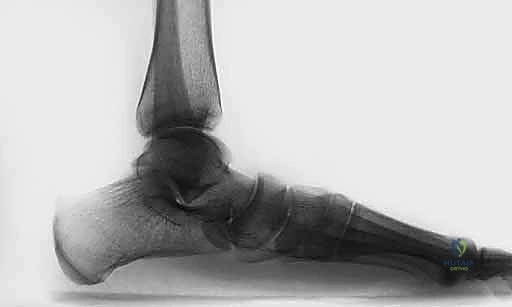
Standard weight-bearing radiographs are the bedrock of our preoperative assessment. These must be obtained with the patient standing, actively bearing weight, and instructed to let the arch sag completely to unmask the true extent of the ligamentous incompetence. Non-weight-bearing films are entirely inadequate and dangerously misleading.
On the AP Foot radiograph, we meticulously calculate the talar head uncoverage angle. This measures the percentage of the talar articular surface that is no longer contained by the navicular, serving as a direct proxy for transverse plane abduction and superomedial spring ligament failure.

The Lateral Foot radiograph is evaluated for plantar migration of the talus. We assess Meary's angle (the talus-first metatarsal angle) and the lateral talocalcaneal angle. A break in the cyma line indicates profound midtarsal subluxation.

Combined AP and Lateral weight-bearing views provide a comprehensive, biplanar understanding of the peritalar subluxation, guiding our decision on whether a lateral column lengthening or a medial displacement calcaneal osteotomy (MDCO) will be required to neutralize the deforming forces.

While radiographs define the bony architecture, Magnetic Resonance Imaging (MRI) is indispensable for interrogating the soft tissues. A high-resolution, non-contrast MRI, ideally evaluated by a musculoskeletal radiologist, allows for direct visualization of the spring ligament complex. We look for increased signal intensity, thickening, discontinuity, or complete absence of the superomedial and inferior bands. MRI also definitively stages the degree of posterior tibial tendon tendinosis or tearing, dictating whether the PTT requires debridement, tubularization, or complete substitution via an FDL transfer.
Operating Room Setup and Patient Positioning
The patient is positioned supine on a standard radiolucent operating table. A significant bump is placed under the ipsilateral hip to internally rotate the lower extremity, bringing the medial aspect of the foot and ankle directly into the surgeon's field of view. This positioning is critical; inadequate internal rotation will force the surgeon to fight gravity and awkward angles throughout the procedure.
A well-padded pneumatic tourniquet is applied to the proximal thigh. The entire lower extremity is prepped and draped in a standard sterile fashion, ensuring exposure from the mid-calf to the toes. Intraoperative fluoroscopy (C-arm) must be positioned on the contralateral side of the table, draped sterilely, and verified to have unimpeded access for AP, lateral, and axial imaging of the foot and ankle. Prophylactic intravenous antibiotics are administered 30 minutes prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical reconstruction of the spring ligament is an exercise in meticulous anatomical dissection and robust biomechanical fixation. It is almost never performed in isolation; it is the soft-tissue capstone to a foundation of bony realignment (e.g., MDCO, Evans osteotomy, or Cotton osteotomy). For the purpose of this masterclass, we will focus specifically on the spring ligament reconstruction phase.
Exposure and Ligament Interrogation
We begin with a medial utility incision, typically 8 to 10 centimeters in length, centered over the course of the posterior tibial tendon, extending from the retromalleolar groove distally to the medial cuneiform.
Careful superficial dissection is performed, identifying and retracting the saphenous vein and nerve dorsally. The flexor retinaculum is incised, and the posterior tibial tendon sheath is opened longitudinally. The PTT is inspected; if it is severely degenerated, it is excised, and the FDL tendon is harvested for transfer. The PTT (or its remnant) is retracted plantarly to expose the underlying spring ligament complex.

At this juncture, the profound pathology of the spring ligament is usually apparent. The superomedial band is often attenuated, thinned out, or completely avulsed from its navicular insertion, exposing the underlying articular cartilage of the talar head.

Preparation of the Anatomical Footprints
Successful ligamentous reconstruction requires robust biological healing, which dictates meticulous preparation of the bony footprints. Using a combination of a surgical scalpel, curettes, and a motorized burr, the native insertion sites on the sustentaculum tali and the medial navicular are decorticated down to bleeding cancellous bone.
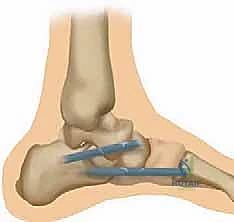
We must identify the exact anatomical origin on the superomedial aspect of the sustentaculum. A guide pin is placed into the sustentaculum, directed laterally and slightly plantarly, ensuring it does not breach the subtalar joint. This is verified with fluoroscopy. A blind-ended tunnel (typically 4.5mm to 5.5mm, depending on graft size) is then reamed over the guide pin.

Similarly, the insertion footprint on the medial navicular is prepared. Depending on the specific technique (e.g., single-bundle vs. double-bundle reconstruction), one or two tunnels are created in the navicular, directed from medial to lateral.

Graft Passage and Biomechanical Tensioning
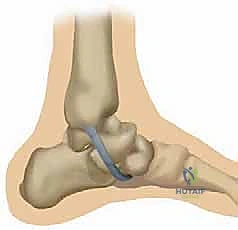
For a comprehensive reconstruction, a robust graft is required. While local tissue augmentation can be attempted for minor attenuation, significant deformity necessitates a free graft—typically a split peroneus longus allograft, an Achilles allograft, or an autologous semitendinosus graft. The graft is prepared on the back table, tubularized, and armed with high-strength non-absorbable sutures at both ends.
The graft is first secured into the sustentaculum tali tunnel. This is most reliably achieved using a bio-tenodesis interference screw, ensuring the graft is seated deeply and firmly at the anatomical origin.

The free end of the graft is then passed distally towards the navicular. This is the critical moment of the procedure: tensioning. The foot must be held in maximal supination, plantarflexion of the first ray, and inversion of the hindfoot—essentially overcorrecting the deformity and fully reducing the talonavicular joint.
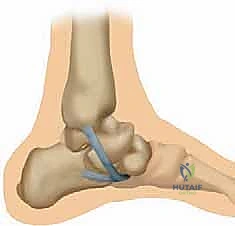
While an assistant holds the foot in this reduced position, the graft is tensioned into the navicular tunnel(s). Fixation is achieved with a second interference screw or, alternatively, with robust suture anchors if a surface-lay technique is preferred.

Once fixed, the tension is tested. The graft should act as a rigid sling, preventing any medial or plantar subluxation of the talar head when a valgus stress is applied to the hindfoot. Any remaining native spring ligament tissue or the anterior deltoid capsule is then imbricated over the graft to provide secondary stabilization and a robust biological envelope.
If an FDL transfer was performed, the FDL tendon is now routed through a separate tunnel in the navicular and tensioned over the newly reconstructed spring ligament complex, providing active, dynamic support to the static reconstruction.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, spring ligament reconstruction, particularly in the context of advanced PCFD, carries a distinct risk profile. Recognizing, mitigating, and managing these complications is the hallmark of an experienced foot and ankle surgeon. Complications can range from transient neuropraxias to catastrophic structural failures requiring salvage arthrodesis.
The most devastating complication is the recurrence of the progressive collapsing foot deformity. This typically occurs not because of isolated graft failure, but due to a failure to adequately address the underlying bony architecture. If the deforming forces (e.g., a short lateral column, a valgus calcaneal axis, or a profound Achilles contracture) are not neutralized with concomitant osteotomies and lengthenings, the reconstructed soft tissues will inevitably stretch and fail over time.
Iatrogenic nerve injury is a significant concern given the medial approach. The saphenous nerve is at risk during the superficial exposure, while the medial plantar nerve is highly vulnerable during dissection near the sustentaculum tali and the plantar aspect of the navicular. Meticulous retraction and a thorough understanding of the anatomical danger zones are required.
Complications and Salvage Matrix
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Deformity / Graft Failure | 5% - 15% | Inadequate bony correction (missed lateral column shortening), failure to lengthen Achilles, severe obesity, non-compliance with NWB. | Revision surgery with triple arthrodesis or talonavicular arthrodesis to provide rigid, permanent stabilization. |
| Medial Plantar Nerve Injury | 1% - 3% | Overzealous deep retraction, errant drill bit/guide pin placement through the plantar sustentaculum. | Initial observation and gabapentinoids. If persistent severe neuropathy, surgical exploration, neurolysis, or neurectomy may be required. |
| Saphenous Neuritis | 3% - 8% | Direct transection or traction injury during the initial medial utility incision. | Desensitization therapy, topical compounded neuropathic creams, targeted corticosteroid injections. Rarely requires surgical excision of the neuroma. |
| Hardware Prominence / Pain | 5% - 10% | Prominent interference screws or suture anchors in the medial navicular, particularly in thin patients. | Conservative management with shoe modifications. If refractory, minor outpatient procedure for hardware removal after biological integration of the graft (typically >9 months). |
| Talonavicular Joint Stiffness | 10% - 20% | Over-tensioning of the graft, prolonged immobilization, aggressive capsular imbrication. | Aggressive physical therapy, dynamic splinting. Mild stiffness is often well-tolerated and preferable to recurrent instability. |
Phased Post-Operative Rehabilitation Protocols
The biological integration of a ligamentous reconstruction, particularly an allograft, requires a prolonged and highly structured rehabilitation protocol. The newly reconstructed spring ligament is mechanically vulnerable for several months; premature loading will inevitably lead to graft attenuation and failure. Patient education and strict adherence to the protocol are non-negotiable.
Phase I: Maximum Protection (Weeks 0 - 2)
Immediately postoperatively, the patient is placed in a well-padded, short-leg plaster or fiberglass splint. The foot is immobilized in slight inversion and equinus to eliminate any tension on the medial structures and the Achilles lengthening. The patient is strictly non-weight-bearing (NWB) and instructed to aggressively elevate the operative extremity above the level of the heart to mitigate edema and promote wound healing. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk stratification.
Phase II: Controlled Immobilization (Weeks 2 - 6)
At the two-week mark, the surgical dressings are removed, and the incisions are inspected for primary healing. Sutures are removed. The patient is transitioned into a rigid fiberglass cast or a locked controlled ankle motion (CAM) boot. The foot is maintained in a neutral to slightly inverted position. The patient remains strictly NWB using crutches, a walker, or a knee scooter. Isometric exercises for the proximal musculature (quadriceps, gluteals) are encouraged to prevent profound deconditioning.
Phase III: Progressive Loading and Early Mobilization (Weeks 6 - 12)
At six weeks, assuming radiographic evidence of osteotomy consolidation (if performed) and clinical stability, the patient begins a meticulously supervised transition to weight-bearing. This starts with partial weight-bearing (PWB) in the CAM boot, progressively advancing to full weight-bearing (FWB) over a 4-week period. Formal physical therapy is initiated. The early focus is on active and active-assisted range of motion of the ankle and subtalar joints, avoiding passive, forceful eversion that would stress the spring ligament graft. Proprioceptive training and gentle intrinsic foot strengthening commence.
Phase IV: Functional Restoration (Weeks 12+)
By the 12-week mark, the patient is typically transitioned out of the CAM boot and into a supportive, stiff-soled athletic shoe fitted with a custom, rigid medial longitudinal arch orthotic. The orthotic is crucial for providing long-term mechanical support to the reconstructed ligament. Physical therapy intensifies, focusing on closed-kinetic-chain exercises, dynamic balance, and progressive strengthening of the posterior tibial tendon and the peroneal complex. Return to high-impact activities or sports is generally restricted until 6 to 9 months postoperatively, contingent upon the restoration of symmetric strength and pain-free dynamic function.
Summary of Landmark Literature and Clinical Guidelines
The evolution of spring ligament reconstruction is a testament to the advancing understanding of foot and ankle biomechanics. Historically, surgical intervention for AAFD focused almost exclusively on the posterior tibial tendon, with procedures like isolated FDL transfers yielding suboptimal long-term results due to the failure to address the profound static instability of the medial arch
