Osteotomy for Femoral Malunion in Children: Comprehensive Surgical Guide
Key Takeaway
Femoral malunion in children presents complex biomechanical challenges requiring precise surgical correction. This guide details the indications, preoperative planning, and step-by-step surgical techniques for corrective osteotomy. Emphasizing both modern internal fixation methods—such as intramedullary nailing and plating—and historical two-stage osteoclasis techniques, it provides orthopedic surgeons with an evidence-based framework to restore anatomic alignment, optimize limb length, and ensure robust osseous union in pediatric patients.
Comprehensive Introduction and Patho-Epidemiology
Femoral shaft fractures represent one of the most frequently encountered major skeletal injuries in the pediatric orthopedic population. The inherent biological advantages of the pediatric skeleton, characterized by a thick, highly vascularized, and osteogenically robust periosteum, facilitate rapid fracture union. However, this very capacity for rapid consolidation can be a double-edged sword; when fractures are inadequately reduced, or when conservative or surgical fixation fails to maintain alignment, rapid malunion is an almost inevitable consequence. The pediatric femur possesses a remarkable, yet strictly conditional, capacity for spontaneous remodeling. This remodeling potential is primarily governed by Wolff’s Law, which dictates that bone adapts to the loads under which it is placed, and the Hueter-Volkmann principle, which describes how mechanical compression inhibits physeal growth while tension stimulates it. Consequently, remodeling is most effective in the plane of adjacent joint motion—specifically, the sagittal plane—where dynamic loading during ambulation naturally realigns the osseous architecture over time.
Despite this biological resilience, the remodeling capacity of the pediatric femur is not infinite and is highly constrained by several critical variables: the child's skeletal age, the distance of the malunion from the nearest active physis, and the specific plane of the deformity. Angular deformities in the coronal plane (varus or valgus) demonstrate significantly less potential for spontaneous correction compared to sagittal plane deformities. Furthermore, rotational deformities (excessive anteversion or retroversion) exhibit virtually zero remodeling potential, regardless of the child's age or the fracture's proximity to the growth plate. When a femoral malunion exceeds these biological thresholds, the altered mechanical axis shifts the weight-bearing loads across the knee and hip joints. Over time, this abnormal biomechanical loading accelerates articular cartilage wear, predisposing the patient to premature, asymmetric joint arthrosis and significant functional impairment.
The epidemiology of pediatric femoral malunions is closely tied to the chosen modality of initial fracture management. Historically, conservative treatments such as spica casting or skeletal traction were the mainstays of therapy, carrying a higher inherent risk of malalignment, particularly in older children or those with high-energy, unstable fracture patterns. While the modern paradigm has shifted toward early surgical stabilization using flexible intramedullary nails, submuscular plating, or rigid lateral entry nails, malunions still occur due to technical errors, premature weight-bearing, or implant failure. A comprehensive understanding of the patho-epidemiology of these deformities is essential for the orthopedic surgeon. It informs not only the decision-making process regarding when to intervene but also the precise geometric requirements of the corrective osteotomy.
The primary objectives of a corrective femoral osteotomy are multifaceted: to meticulously restore the mechanical axis of the lower extremity, to correct any clinically significant rotational malalignment, to equalize limb length discrepancies (LLD), and ultimately, to prevent long-term degenerative joint disease. Achieving these goals requires a profound appreciation of normal lower extremity biomechanics and a meticulous approach to preoperative planning. The surgeon must balance the need for precise anatomical correction with the biological imperative of preserving the local vascular supply to ensure rapid and predictable osseous union following the osteotomy.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of femoral surgical anatomy and lower extremity biomechanics is the foundational prerequisite for executing a successful corrective osteotomy. The femur is the longest and strongest bone in the human body, enveloped by a massive musculature that exerts immense deforming forces following a fracture or osteotomy. The thigh is divided into three distinct fascial compartments: anterior, medial, and posterior. For the vast majority of diaphyseal and subtrochanteric femoral osteotomies, the surgical approach traverses the anterior compartment, specifically utilizing the internervous plane or the substance of the vastus lateralis. The vastus lateralis originates from the greater trochanter and the lateral lip of the linea aspera, receiving its innervation from the femoral nerve. Elevating this muscle anteriorly off the lateral intermuscular septum provides safe, extensile access to the lateral and anterior aspects of the femoral shaft.
The vascular anatomy of the femur is of paramount importance during both the surgical approach and the osteotomy itself. The primary blood supply to the femoral diaphysis is derived from the profunda femoris artery, which gives rise to a series of perforating branches. These perforators pierce the lateral intermuscular septum in close proximity to the linea aspera to supply the vastus lateralis. During the deep dissection, these vessels must be meticulously identified, isolated, and ligated or cauterized to prevent catastrophic postoperative hematoma. Furthermore, the periosteal blood supply, which is particularly robust in children, forms a dense anastomotic network critical for callus formation. Stripping of the periosteum must be strictly limited to the areas required for the osteotomy cuts and implant footprint; excessive circumferential stripping will devascularize the cortical bone, exponentially increasing the risk of delayed union or nonunion.
Biomechanically, the lower extremity is evaluated using both the mechanical and anatomic axes. The mechanical axis of the lower limb is defined by a line drawn from the center of the femoral head to the center of the ankle joint (tibial plafond). In a normally aligned limb, this line should pass precisely through, or slightly medial to, the center of the knee joint. The anatomic axis of the femur is defined by a line bisecting the medullary canal. The angle formed between the mechanical and anatomic axes of the femur is typically 5 to 7 degrees. When planning a corrective osteotomy, the surgeon must calculate joint orientation angles, most notably the mechanical Lateral Distal Femoral Angle (mLDFA), which normally measures 88 degrees, and the mechanical Medial Proximal Femoral Angle (mMPFA), which normally measures 84 degrees. Deviations from these normative values quantify the magnitude of the coronal plane deformity.
Rotational biomechanics are equally critical and often more challenging to assess clinically. Normal femoral anteversion is approximately 40 degrees at birth and gradually remodels to 15 degrees by skeletal maturity. A rotational malunion disrupts this delicate torsional alignment, leading to profound gait abnormalities, such as intoeing or outtoeing, and altering the patellofemoral tracking mechanics. Because rotational deformities do not remodel, they must be quantified precisely using advanced imaging. The Center of Rotation of Angulation (CORA) is the biomechanical cornerstone of deformity correction. The CORA represents the intersection of the proximal and distal mechanical or anatomic axis lines. Paley’s rules of osteotomy dictate that to achieve pure angular correction without inducing secondary translation (displacement), the osteotomy must pass through the CORA. If the osteotomy is performed at a level different from the CORA, the surgeon must intentionally translate the fragments to restore the overall mechanical axis.
Exhaustive Indications and Contraindications
The decision to proceed with a corrective osteotomy for a pediatric femoral malunion is highly nuanced, requiring the surgeon to synthesize the patient's age, remaining growth potential, functional deficit, and the specific geometric characteristics of the deformity. Not all malunions require surgical intervention; many will remodel sufficiently to provide a functional, pain-free limb. Therefore, establishing rigorous indications and contraindications is vital to avoid unnecessary surgical morbidity.
The primary indication for surgical intervention is a deformity that exceeds the child's biological remodeling potential and causes, or is highly likely to cause, functional impairment or premature joint degeneration. As a general heuristic, angular deformities in the sagittal plane (procurvatum or recurvatum) remodel best, particularly if the child is under 10 years of age and the deformity is located near the rapidly growing distal femoral physis. Conversely, coronal plane deformities (varus or valgus) have limited remodeling potential. An osteotomy is generally indicated for coronal deformities exceeding 10 to 15 degrees in a child older than 8 years. Rotational deformities exhibit no remodeling potential; therefore, a clinically significant rotational malunion (typically >15-20 degrees of version difference compared to the contralateral normal side) that causes gait disturbance or patellofemoral instability is an absolute indication for derotational osteotomy.
Limb length discrepancy (LLD) is another critical factor. Pediatric femur fractures frequently stimulate overgrowth due to the hyperemic response of healing, which can add 1 to 2 centimeters of length to the affected limb over the subsequent 18 to 24 months. If a malunion heals with significant shortening (e.g., >3 cm) that cannot be compensated for by anticipated overgrowth, or if it heals with lengthening that exacerbates an existing discrepancy, corrective surgery is warranted. In such cases, the osteotomy may be combined with acute shortening, acute lengthening, or the application of an external fixator for gradual distraction osteogenesis.
Contraindications to corrective osteotomy must be carefully evaluated to prevent catastrophic postoperative complications. Active, untreated local or systemic infection is an absolute contraindication to internal fixation and must be eradicated prior to any structural bone work. Poor soft tissue envelopes, such as those seen in severe burn victims or following massive degloving injuries, may preclude standard open approaches and necessitate the use of percutaneous techniques and external fixation. Severe medical comorbidities that render the child unfit for general anesthesia or major surgery are also clear contraindications.
| Category | Specific Indications | Specific Contraindications |
|---|---|---|
| Age & Growth | Girls >10 yrs, Boys >12 yrs with significant deformity; Deformity far from active physis. | Infants and toddlers (<4 yrs) with massive remodeling potential (relative). |
| Plane of Deformity | Coronal plane (Varus/Valgus) >10-15°; Sagittal plane >20° in older children. | Mild sagittal plane deformities in young children (<8 yrs). |
| Rotational Alignment | Torsional difference >15-20° causing gait dysfunction or patellar maltracking. | Asymptomatic, mild rotational asymmetry (<10°). |
| Limb Length | Projected LLD at maturity >2.5 cm requiring acute correction or lengthening. | Projected LLD at maturity <1.5 cm (manageable with shoe lift). |
| Biological/Systemic | Intractable pain, impending joint arthrosis, failed conservative management. | Active osteomyelitis, severe malnutrition, unacceptable anesthetic risk. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough, meticulous preoperative planning is the absolute cornerstone of a successful corrective osteotomy. The surgeon must transition from a qualitative assessment of the deformity to a precise, quantitative geometric blueprint. This process begins with acquiring high-quality, standardized imaging. Full-length, weight-bearing standing radiographs of both lower extremities, taken from the pelvis to the ankles on a single cassette (or digitally stitched), are mandatory. The patellae must be strictly oriented forward to ensure an accurate assessment of the coronal plane, minimizing the projectional artifacts caused by rotational malalignment.
From these full-length radiographs, the surgeon calculates the Mechanical Axis Deviation (MAD). The mechanical axis line is drawn from the center of the femoral head to the center of the tibial plafond. The distance from this line to the center of the knee joint dictates the MAD. Next, the joint orientation angles (mLDFA and mMPFA) are measured to localize the source of the deformity. The Center of Rotation of Angulation (CORA) is then mapped by drawing the proximal and distal anatomical or mechanical axes of the femur; their intersection defines the CORA. If the deformity is uniapical, a single CORA will be identified. If the deformity is multiapical, multiple CORAs must be analyzed, potentially necessitating a multi-level osteotomy.
For rotational deformities and precise limb length measurements, a CT scanogram is the gold standard. The rotational profile is determined by superimposing axial cuts of the proximal femur (femoral neck axis) and the distal femur (posterior condylar axis). The angle between these two axes defines the femoral version. Comparing the affected side to the contralateral normal side provides the exact degree of rotational correction required. Once all parameters are quantified, digital or analog templating is performed. The surgeon selects the osteotomy level (ideally at the CORA), determines the wedge size and angle for correction, and selects the appropriate fixation implant (e.g., locking plate, intramedullary nail) to ensure adequate purchase in both the proximal and distal fragments.
Proper patient positioning in the operating room is critical for executing the preoperative plan. The patient is placed supine on a radiolucent operating table to allow for unimpeded, orthogonal fluoroscopic imaging of the entire femur, hip, and knee. A bump is often placed under the ipsilateral hemipelvis to internally rotate the lower extremity until the patella is pointing directly toward the ceiling, neutralizing any external rotation contracture. The entire lower extremity, from the iliac crest to the toes, must be prepped and draped free to allow for intraoperative manipulation and clinical assessment of alignment and rotation. The fluoroscopy unit (C-arm) should be positioned on the contralateral side of the table, ensuring the surgeon has unobstructed access to the lateral aspect of the thigh.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a corrective osteotomy demands precision, respect for soft tissues, and strict adherence to the preoperative templating. For the majority of diaphyseal and subtrochanteric malunions, the lateral approach to the femur is the workhorse exposure. It provides safe, extensile access while minimizing the risk to major neurovascular structures. The incision is centered over the apex of the deformity (the planned osteotomy site) along the lateral aspect of the thigh. The fascia lata is incised longitudinally in line with the skin incision.
The deep dissection involves elevating the vastus lateralis. Instead of splitting the muscle fibers, which causes unnecessary bleeding and denervation, the muscle is elevated anteriorly off the lateral intermuscular septum. As the dissection proceeds distally and posteriorly toward the linea aspera, the surgeon will encounter the perforating branches of the profunda femoris artery and vein. These vessels must be meticulously isolated, clamped, and ligated or cauterized to prevent postoperative hematoma. Once the femoral shaft is exposed, the periosteum is incised longitudinally and elevated. It is critical to strip only enough periosteum to accommodate the osteotomy cuts and the footprint of the planned fixation device; preserving a robust periosteal sleeve is vital for maintaining cortical perfusion and ensuring rapid postoperative callus formation.
Direct Corrective Osteotomy Execution
With the bone exposed, the surgeon correlates the gross anatomy with the preoperative radiographs to pinpoint the exact level of the planned osteotomy (the CORA). The osteotomy can be executed using several techniques. A motorized oscillating or reciprocating saw provides a clean, precise cut but generates significant heat, which can lead to thermal necrosis of the bone ends. To mitigate this, continuous saline irrigation must be applied directly to the saw blade during the cut. Alternatively, the drill and osteotome method can be utilized. The surgeon outlines the planned osteotomy plane by drilling multiple contiguous unicortical or bicortical holes. A narrow, sharp osteotome is then used to connect these holes and complete the bone division. This technique generates minimal heat and preserves the osteogenic potential of the bone ends, though it may result in a slightly more irregular surface.
In cases of long-standing malunion, resecting a small segment of bone (0.6 to 1.3 cm) from the apex of the deformity is highly recommended. The bone ends at the malunion site are typically sclerotic and avascular; resecting back to healthy, bleeding cortical bone is essential for reliable union. Furthermore, creating flat, parallel surfaces allows for stable apposition of the fragments. Importantly, in chronic deformities, the surrounding soft tissues (muscles, fascia, neurovascular bundles) have contracted and adapted to the shortened or angulated state. Shortening the bone slightly during the osteotomy reduces this soft tissue tension, making the reduction significantly easier and preventing neurovascular compromise (e.g., sciatic nerve stretch) upon realignment of the limb.
Fixation Strategies
Once the deformity is acutely corrected and the bone ends are optimally apposed, rigid internal or external fixation is applied to maintain the alignment until biological union occurs. The choice of fixation depends on the patient's age, the location of the osteotomy, and the quality of the bone.
- Plate Osteosynthesis: Broad dynamic compression plates (DCP) or locking compression plates (LCP) are excellent for diaphyseal and metaphyseal osteotomies. They provide absolute stability, allowing for early mobilization. The plate should be pre-contoured to match the normal anatomy of the femur. At least three, and ideally four, bicortical screws should be placed in both the proximal and distal fragments to ensure adequate biomechanical stability.
- Intramedullary Nailing: In older children and adolescents (typically those over 10 years of age with closed or closing greater trochanteric physes), a rigid, interlocking intramedullary (IM) nail is the preferred method. IM nails provide superior load-sharing biomechanics, excellent control of both angular and rotational alignment, and allow for early weight-bearing. A lateral entry point (tip of the greater trochanter) is strongly preferred in the pediatric population to avoid the piriformis fossa and eliminate the risk of iatrogenic avascular necrosis (AVN) of the femoral head.
- External Fixation: For severe, multiplanar deformities, or when acute correction would result in excessive soft tissue tension or neurovascular compromise, external fixation is indicated. Circular frames (e.g., Ilizarov or Taylor Spatial Frame) or monolateral fixators allow for gradual, computer-assisted correction of the deformity and simultaneous limb lengthening via distraction osteogenesis.
Historical and Alternative Techniques (Resource-Limited Settings)
In global health scenarios or resource-limited settings where modern fluoroscopy, rigid IM nailing systems, or locking plates are unavailable, orthopedic surgeons must rely on time-tested, biologically driven techniques. These historical methods leverage the immense osteogenic potential of the pediatric periosteum and natural callus formation to stabilize the correction.
The Ferguson, Thompson, and King Two-Stage Osteotomy
Ferguson et al. described an elegant two-stage osteotomy designed to correct angular deformities while virtually eliminating the risk of nonunion or catastrophic loss of fixation.
Stage 1: Defect Creation and Grafting
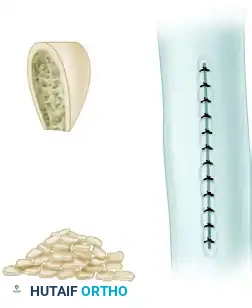
Through a limited approach, a rectangular segment of cortical bone, comprising approximately one-half the width of the diaphysis, is excised from the concave side of the deformity.

This resected cortical block is not discarded; rather, it is meticulously morselized on the back table into small cancellous and cortical chips. These autologous bone chips are then packed tightly back into the created defect. This process acts as a massive biological stimulus, inciting aggressive local osteogenesis and hypervascularity.

Stage 2: Deformity Correction
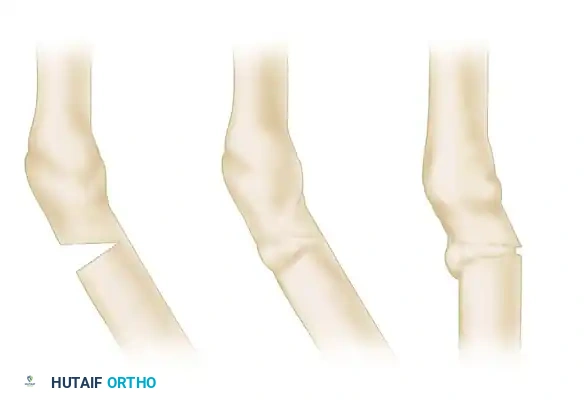
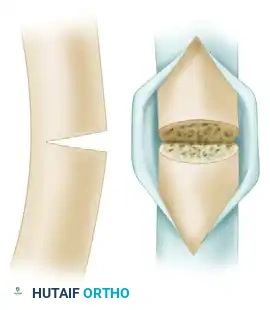
The patient is immobilized, and the second stage is delayed for 3 to 6 weeks. During this interval, a thick, sticky, highly vascular callus forms across the grafted defect. Once this medial callus is deemed clinically and radiographically stable, the patient returns to the operating room. The osteotomy is completed on the convex side of the deformity by resecting a precise wedge of bone exactly opposite the middle of the first defect.

The surgeon then manually manipulates the limb, applying a bending moment to close the lateral wedge and correct the varus or valgus angulation. The previously formed, robust callus on the concave side acts as a living, biological hinge. It provides immense intrinsic stability, preventing translation or over-correction. The limb is then immobilized in a spica cast until definitive solid union is achieved.
The Moore Osteotomy-Osteoclasis Technique
Moore described another ingenious, biologically focused method for correcting malunited fractures that minimizes initial soft tissue stripping and relies on delayed manual osteoclasis.
Surgical Execution:
At the apex of the maximal deformity, the surgeon divides approximately three-fourths of the bone's circumference using a sharp osteotome. A precisely calculated wedge of bone is then resected from the diaphysis, leaving the far cortex on the concave side of the deformity completely intact. The proximal cut is oriented perpendicular to the long axis of the proximal fragment, and the distal cut is perpendicular to the distal fragment.

Similar to the Ferguson technique, the excised wedge of bone is reduced to small chips and returned to the defect to act as an autograft. The periosteum is meticulously repaired and approximated over the bone chips to contain the graft and promote rapid revascularization.

Postoperative Casting and Osteoclasis:
Immediately following the initial surgery, the limb is placed in a rigid, well-molded cast in the uncorrected position. At 3 to 4 weeks postoperatively, early callus has consolidated the grafts, but the newly formed woven bone remains malleable. At this precise biological window, a circular segment of the cast is removed (windowed) at the level of the osteotomy.

With the cast windowed, the surgeon performs a manual osteoclasis—a controlled, forceful manipulation to break the remaining intact cortex and acutely correct the deformity. The intact, newly formed callus acts as a robust, flexible hinge, preventing any unwanted translation of the bone fragments during the correction.
Once the desired anatomical alignment is achieved and verified radiographically, the cast window is repaired with fresh plaster or fiberglass, locking the limb in the newly corrected position until definitive osseous union occurs.
Complications, Incidence Rates, and Salvage Management
Despite meticulous preoperative planning and precise surgical execution, osteotomies for pediatric femoral malunions carry a distinct profile of potential complications. The surgeon must be acutely aware of these risks, employ rigorous preventative strategies, and possess the technical armamentarium to manage them should they arise. Complications can be broadly categorized into biological failures (nonunion, delayed union, infection), mechanical failures (hardware breakage, loss of fixation, recurrence of deformity), and iatrogenic injuries (neurovascular compromise).
Nonunion and delayed union are critical biological complications. While the pediatric skeleton is highly osteogenic, the bone ends at a malunion site are often sclerotic, poorly vascularized, and mechanically inferior. Failure to resect this sclerotic bone back to bleeding margins, or excessive circumferential stripping of the periosteum during the surgical approach, severely compromises the local biological environment. Furthermore, inadequate mechanical stability—due to the selection of an undersized plate, insufficient screw purchase, or a loose intramedullary nail—allows for excessive micromotion, leading to hypertrophic nonunion. Management of nonunion typically requires revision surgery, which may involve exchange nailing, the application of a larger compression plate, and the addition of autologous iliac crest bone graft (ICBG) to stimulate osteogenesis.
Neurovascular injury is a devastating iatrogenic complication. The superficial femoral artery and vein, located in the adductor canal on the medial aspect of the femur, are at significant risk during deep dissection, drilling, and the execution of the osteotomy cuts. The surgeon must maintain strict control of all instruments. When using a motorized saw or osteotomes, the medial soft tissues must be continuously protected with blunt retractors, such as properly positioned Hohmann retractors. Postoperatively, the limb must be closely monitored for signs of compartment syndrome or vascular compromise, particularly if the osteotomy involved acute shortening or significant angular correction that may have kinked or stretched the vessels.
Infection, though less common in elective, closed pediatric osteotomies compared to trauma settings, remains a severe threat. Meticulous soft tissue handling, strict adherence to sterile technique, and the administration of appropriate weight-based prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are mandatory. In cases utilizing external fixation, pin tract infections are the most frequent complication. These must be treated aggressively with local pin site care (chlorhexidine or hydrogen peroxide solutions) and oral antibiotics to prevent progression to deep osteomyelitis or ring sequestrum, which would necessitate premature removal of the fixator.
| Complication | Estimated Incidence | Preventative Strategy | Salvage / Management |
|---|---|---|---|
| Delayed Union / Nonunion | 2% - 5% | Resect sclerotic bone; preserve periosteum; ensure rigid fixation. | Revision fixation (exchange nail/larger plate); Autologous bone grafting (ICBG). |
| Recurrence of Deformity | 5% - 10% | Over-correct slightly if growth remains; use load-sharing IM nails in older kids. | Revision osteotomy; guided growth (hemiepiphysiodesis) if physis is open. |
| Neurovascular Injury | < 1% | Protect medial structures with Hohmann retractors during all cuts/drilling. | Immediate vascular surgery consultation; exploration and repair. |
| Infection (Deep) | 1% - 2% | Strict sterility; prophylactic IV antibiotics; meticulous soft tissue handling. | Surgical debridement (I&D); hardware removal if union achieved; culture-specific IV antibiotics. |
| Pin Tract Infection (Ex-Fix) | 15% - 30% | Meticulous daily pin site care; proper pin insertion technique (low heat). | Oral antibiotics; aggressive local care; pin removal/exchange if loosening occurs. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following a femoral osteotomy is not a monolithic pathway; rather, it is highly customized and strictly dictated by the type of fixation achieved intraoperatively, the quality of the host bone, and the age and compliance of the pediatric patient. A phased approach ensures that the mechanical demands placed on the healing bone do not exceed its biological capacity at any given time.
Phase 1: Acute Protection and Soft Tissue Healing (0-2 Weeks)
Regardless of the fixation method, the primary goals during the first two weeks are pain control, edema management, and the protection of the surgical incision. For patients with rigid internal fixation (locking plates or IM nails), the limb is typically maintained in a non-weight-bearing status. Gentle, active-assisted range of motion (ROM) exercises for the hip and knee are initiated immediately to prevent capsular contracture and muscle atrophy. Physical therapy focuses on teaching safe transfer techniques and the proper use of assistive devices (crutches or a walker). For patients managed with cast immobilization (e.g., following a Moore osteoclasis), strict elevation and monitoring for neurovascular compromise or cast sores are paramount.
Phase 2: Callus Formation and Progressive Loading (2-6 Weeks)
During this phase, the biological focus shifts to early callus formation. For patients with rigid internal fixation, follow-up orthogonal radiographs are obtained at 2 to 3 weeks. If early, hazy callus is visible bridging the osteotomy site, the patient may be advanced to toe-touch or partial weight-bearing (approximately 20-30% of body weight). This controlled axial loading stimulates osteogenesis via micromotion, adhering to Wolff's Law. ROM exercises are advanced to active and
