Sublimis Tendon Transfer for Thumb Opposition (Riordan)
Key Takeaway
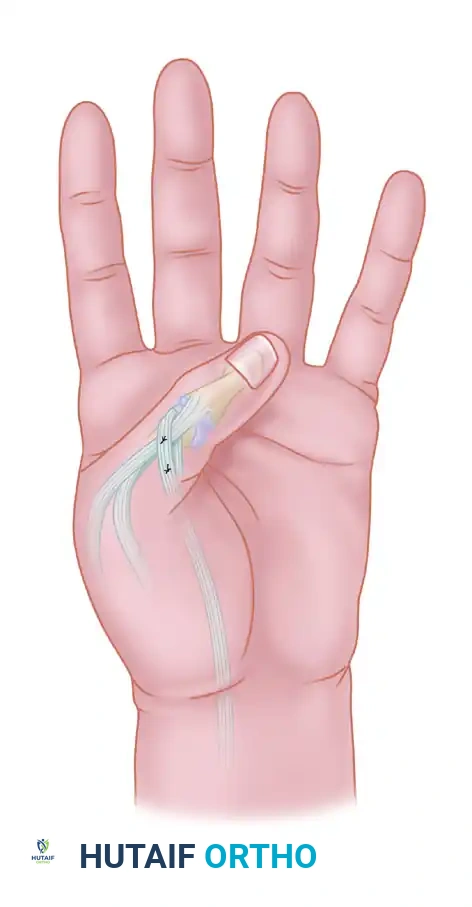
The Riordan technique for sublimis tendon transfer is a highly effective opponensplasty utilized to restore thumb opposition in median nerve palsy. By harvesting the ring finger flexor digitorum superficialis, routing it through a flexor carpi ulnaris pulley, and inserting it into the thumb's extensor mechanism, surgeons can reconstruct the complex biomechanics of palmar abduction, flexion, and pronation essential for functional pinch.
Comprehensive Introduction and Patho-Epidemiology
The restoration of thumb opposition represents one of the most critical and biomechanically demanding reconstructive procedures in the armamentarium of upper extremity surgery. Opposition is not a simple, uniplanar motion; rather, it is a highly complex, multi-planar kinematic sequence requiring the simultaneous palmar abduction, flexion, and pronation of the first metacarpal. This precise positioning must be coupled with stable extension of the interphalangeal (IP) joint and metacarpophalangeal (MCP) joint to facilitate a robust, functional tip-to-tip or pulp-to-pulp pinch against the index and long fingers. The evolutionary advantage of the human hand is inextricably linked to this opposable function, and its loss renders the hand severely impaired, reducing it to a primitive assistive appendage capable only of rudimentary hook grasp or lateral key pinch.
In the clinical setting, the loss of opposition most frequently arises from pathology affecting the median nerve, which provides the critical motor innervation to the intrinsic thenar musculature. Specifically, the abductor pollicis brevis (APB), the opponens pollicis (OP), and the superficial head of the flexor pollicis brevis (FPB) are rendered paralytic in cases of isolated low median nerve palsy. This denervation can result from traumatic lacerations at the wrist, severe and neglected carpal tunnel syndrome leading to irreversible thenar atrophy, or infectious and neurologic etiologies such as poliomyelitis and Charcot-Marie-Tooth disease. As the thenar muscles atrophy, the unopposed pull of the adductor pollicis (ulnar nerve innervated) and the extensor pollicis longus (radial nerve innervated) drives the thumb into a supinated, adducted posture, progressively leading to secondary soft-tissue contractures of the first web space.
To address this profound functional deficit, the transfer of the sublimis tendon—specifically utilizing the flexor digitorum superficialis (FDS) of the ring finger—has endured as a gold-standard opponensplasty. Pioneered by Sterling Bunnell and subsequently refined by Paul Brand and Daniel Riordan, this procedure elegantly leverages the synergistic action of the ring finger FDS. The physiological action of the donor muscle (finger flexion during power grasp) is highly synergistic with thumb opposition, significantly reducing the cognitive burden of postoperative motor re-education compared to non-synergistic transfers like the extensor indicis proprius (EIP).
The epidemiology of median nerve injuries dictates a steady demand for this reconstructive technique. While early microsurgical repair of the median nerve yields favorable outcomes in young patients, delayed presentations, crush injuries, or advanced age often result in incomplete motor recovery despite technically sound nerve reconstruction. Furthermore, the global prevalence of advanced, neglected compressive neuropathies ensures that irreversible thenar atrophy remains a common clinical entity. In these scenarios, the Riordan modification of the sublimis transfer is particularly distinguished by its sophisticated dual-insertion method into the thumb's extensor mechanism, which not only restores the complex vector of opposition but actively prevents the hyperflexion of the IP joint (a Froment’s sign equivalent) during forceful pinch, a common failure point in earlier, simpler opponensplasties.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and the underlying biomechanical principles is paramount for the successful execution of the Riordan opponensplasty. The normal mechanics of thumb opposition rely heavily on the abductor pollicis brevis (APB), which acts as the primary driver of palmar abduction and pronation. The APB originates from the flexor retinaculum and the tubercles of the scaphoid and trapezium, inserting into the radial base of the proximal phalanx and the extensor expansion. To successfully reconstruct opposition, the transferred tendon must meticulously replicate the vector of the paralyzed APB. The ideal vector for opposition originates from the region of the pisiform and directs toward the metacarpophalangeal (MCP) joint of the thumb.
The donor muscle, the flexor digitorum superficialis (FDS) of the ring finger, is anatomically uniquely suited for this transfer. The FDS muscle belly is robust, providing adequate excursion (approximately 3 to 4 cm) and tension-generating capacity to mobilize the thumb against resistance. Distally, the FDS tendon bifurcates at the level of the proximal phalanx to form Camper's chiasm, allowing the flexor digitorum profundus (FDP) to pass through to its distal insertion. Meticulous anatomical dissection and division of these slips at the proximal interphalangeal (PIP) joint are critical; failure to completely free the FDS from the FDP will result in tethering, altering the excursion mechanics and potentially inducing a "lumbrical plus" deformity or severe PIP joint stiffness in the donor digit.
The biomechanical genius of the Riordan technique lies in its dual-insertion strategy, which addresses the dynamic instability of the thumb during pinch. In a normal thumb, intrinsic muscles stabilize the MCP joint and assist the extensor pollicis longus (EPL) in extending the IP joint. When these intrinsics are paralyzed, the extrinsic flexor pollicis longus (FPL) overpowers the weakened extensor mechanism during pinch, leading to hyperflexion of the IP joint and hyperextension of the MCP joint (akin to Froment's sign seen in ulnar nerve palsy, but occurring here due to lack of intrinsic stabilization). By splitting the transferred sublimis tendon and inserting one slip into the APB tendon (to drive abduction and pronation) and the other directly into the EPL aponeurosis, the transfer simultaneously stabilizes the MCP joint and extends the IP joint. This creates a rigid, biomechanically sound post for the index and middle fingers to pinch against.
Furthermore, the creation of the pulley at the flexor carpi ulnaris (FCU) is a critical biomechanical step. By utilizing the FCU near its insertion on the pisiform, the surgeon establishes a fixed fulcrum that perfectly redirects the sublimis tendon to pull the thumb into palmar abduction and pronation. If the pulley is positioned too proximally, the vector becomes too parallel to the radius, resulting in radial abduction rather than true palmar opposition. If the tendon is routed deep to the palmar fascia rather than strictly subcutaneously, the moment arm for palmar abduction is drastically reduced, rendering the transfer mechanically inefficient and clinically unsuccessful.
Exhaustive Indications and Contraindications
The decision to proceed with a sublimis tendon transfer for thumb opposition requires a rigorous evaluation of the patient's neurological status, anatomical prerequisites, and functional demands. The primary indication is the irreversible loss of thenar intrinsic muscle function, most commonly secondary to a low median nerve palsy. This includes patients with severe, late-stage carpal tunnel syndrome where electromyography (EMG) confirms absent motor unit potentials in the APB and OP, and clinical examination reveals profound thenar wasting. Additionally, traumatic nerve lacerations that have failed to reinnervate after primary repair or nerve grafting, as well as neurologic conditions like poliomyelitis or specific variants of Charcot-Marie-Tooth disease, represent classic indications for this reconstructive procedure.
However, the presence of a paralyzed thenar eminence does not automatically qualify a patient for an opponensplasty. Several absolute prerequisites must be met to ensure surgical success. Foremost among these is a completely supple first web space. A tendon transfer is designed to provide dynamic motion; it cannot, under any circumstances, overcome a fixed skeletal or soft-tissue contracture. If a severe adduction contracture exists, it must be aggressively addressed via conservative serial casting or surgical release (e.g., Z-plasty of the web space, release of the adductor pollicis fascia, or even trapezial wedge osteotomy) prior to or concomitantly with the tendon transfer. Furthermore, the donor ring finger FDS must demonstrate normal Medical Research Council (MRC) Grade 5 strength, and the thumb carpometacarpal (CMC), MCP, and IP joints must possess a functional, pain-free passive range of motion.
Contraindications must be carefully respected to avoid devastating functional downgrades. High median nerve palsies represent a relative contraindication to using the FDS as a donor, as the FDS itself is innervated by the median nerve and will be paralyzed. In such cases, alternative donors such as the extensor indicis proprius (EIP) or the abductor digiti minimi (Huber transfer) must be considered. Additionally, patients with severe spasticity, profound cognitive impairment precluding participation in postoperative rehabilitation, or those lacking adequate soft-tissue coverage over the volar wrist and thenar eminence are poor candidates. The surgeon must also carefully evaluate the functional status of the donor digit; pre-existing PIP joint stiffness or a tendency toward swan-neck deformity in the ring finger should prompt the consideration of an alternative donor to prevent exacerbating donor site morbidity.
| Parameter | Indications / Favorable Factors | Contraindications / Unfavorable Factors |
|---|---|---|
| Neurological Deficit | Isolated low median nerve palsy, late-stage CTS, Poliomyelitis | High median nerve palsy (FDS paralyzed), severe generalized spasticity |
| Donor Muscle Status | Ring finger FDS strength MRC Grade 5, independent FDS function | FDS strength < Grade 4, tethered FDS, absence of independent FDS |
| First Web Space | Supple, passive palmar abduction > 45 degrees, no adductor contracture | Fixed adduction contracture, severe cutaneous scarring limiting expansion |
| Thumb Joint Mobility | Full, pain-free passive ROM at CMC, MCP, and IP joints | Arthritic CMC joint, fixed MCP hyperextension, ankylosed IP joint |
| Patient Factors | High motivation, capable of complex postoperative motor re-education | Severe cognitive impairment, non-compliance, active local infection |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful Riordan opponensplasty. The clinical examination must be exhaustive, beginning with a precise assessment of the motor deficit. The surgeon must isolate and test the APB, observing not just for movement but for the quality of the muscle belly and any palpable contraction. The donor FDS of the ring finger is tested by holding the index, middle, and small fingers in full extension to neutralize the FDP, and asking the patient to flex the ring finger PIP joint. This confirms the independent function and strength of the donor muscle. The passive mobility of the first web space is then quantified; the surgeon should be able to passively place the thumb in full opposition without encountering rigid resistance. If resistance is met, the surgical plan must be modified to include a preliminary or concurrent web space release.
Templating for this procedure involves a mental and physical rehearsal of the tendon routing and vector alignment. The surgeon must map out the anticipated path of the sublimis tendon from the ring finger, through the volar forearm, around the FCU pulley at the pisiform, and across the thenar eminence to the dual insertion points on the thumb. Skin incisions should be planned to avoid crossing flexion creases at right angles, thereby preventing postoperative scar contractures. The selection of suture materials is also determined preoperatively; nonabsorbable, braided synthetic sutures (such as 3-0 or 4-0 polyester) are typically selected for the tendon weaves and pulley construction due to their high tensile strength and minimal tissue reactivity.
Patient positioning and operating room setup must be optimized for meticulous hand surgery. The patient is placed in the supine position with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The use of an upper extremity tourniquet is mandatory to ensure a bloodless surgical field, which is critical for the precise identification of tendon slips, the superficial radial nerve branches, and the delicate extensor aponeurosis. The arm is prepped and draped in a standard sterile fashion, allowing access from the mid-arm down to the fingertips.
Surgical loupe magnification (typically 2.5x to 3.5x) is highly recommended for the duration of the procedure, particularly during the management of Camper's chiasm and the dual insertion into the thumb's extensor mechanism. Standard hand surgery instrumentation is required, including delicate tenotomy scissors, fine-toothed forceps, and specialized tendon passers or carriers (such as a Brand tendon passer) for the subcutaneous routing. The surgeon should also ensure the availability of small hemostats for the intraoperative tenodesis test, which is the most critical step in determining the appropriate tension of the transfer.
Step-by-Step Surgical Approach and Fixation Technique
Phase 1: Harvesting the Ring Finger Sublimis Tendon
The procedure commences with the meticulous harvest of the donor tendon. The ring finger sublimis tendon is exposed through an ulnar midlateral incision centered over the proximal interphalangeal (PIP) joint. The ulnar approach is specifically preferred to avoid placing a scar on the radial pinch surface of the digit, which is critical for tactile interaction with the thumb, and to protect the more dominant radial neurovascular bundle. The incision is carried down through the subcutaneous tissue, and the flexor tendon sheath is carefully incised.
Identification and division of the FDS tendon require precision. The FDS is identified and divided at the level of the PIP joint or just proximal to it. Managing Camper's chiasm is a critical, highly technical step. The surgeon must meticulously divide the chiasm, separating the two slips of the sublimis tendon at the level of the joint. They must be completely freed from their passage around the flexor digitorum profundus (FDP). The surgeon must visually confirm that no residual slips of FDS are tethering the FDP. Failure to adequately separate these slips will result in tethering of the profundus tendon, leading to restricted finger flexion or a paradoxical "lumbrical plus" deformity during attempted grip. Once completely freed, the tendon is left in the sheath temporarily to be withdrawn from the wrist later.
Phase 2: Creation of the Flexor Carpi Ulnaris Pulley
Attention is then directed to the volar wrist to create the critical biomechanical fulcrum. The FCU tendon is exposed through an L-shaped incision. The longitudinal limb of the incision should extend proximally along the FCU tendon, and the transverse limb should turn distally and radialward, running parallel to the major flexor creases of the wrist. This incision design prevents the formation of a restrictive, linear scar contracture across the radiocarpal joint. The antebrachial fascia is incised, and the FCU tendon is clearly delineated down to its insertion on the pisiform.
To construct a robust pulley that provides the correct biomechanical vector for opposition, the surgeon cuts halfway through the FCU tendon at a point approximately 6.0 cm proximal to the pisiform. The radial half of the FCU tendon is then stripped distally, stopping almost at the pisiform to maintain its distal vascularity and structural integrity. A loop is created that must be large enough for the sublimis tendon to pass through smoothly without friction, yet snug enough to prevent bowstringing. The radial segment of the FCU is carried through a split made in the remaining intact ulnar half of the tendon, looped back upon itself, and sutured securely with multiple interrupted nonabsorbable braided sutures (e.g., 3-0 Ethibond).
Phase 3: Thumb Exposure and Preparation
The preparation of the thumb requires wide exposure to access the multiple insertion sites dictated by the Riordan technique. A wide C-shaped incision is made on the thumb. The incision begins on the dorsum of the thumb just proximal to the IP joint, proceeds proximally and volarward around to the radial aspect of the thumb, and at a point just proximal to the MCP joint, curves dorsalward, keeping in line with the major skin creases of the thenar eminence. Flaps are elevated with careful preservation of the subdermal vascular plexus.
During this dissection, meticulous care must be taken to identify and protect the fine sensory branches of the superficial radial nerve (SRN) on the dorsoradial aspect of the thumb. Injury to these branches results in debilitating, painful neuromas that can completely negate the functional benefits of the opponensplasty. Once the nerve branches are protected, the surgeon clearly defines the insertion sites: the extensor pollicis longus (EPL) tendon over the proximal phalanx, the extensor aponeurosis over the MCP joint, and the paralyzed abductor pollicis brevis (APB) tendon near its insertion.
Phase 4: Tendon Routing and Subcutaneous Tunneling
With the donor tendon prepared and the insertion sites exposed, the tendon routing phase begins. At the wrist, the previously released ring finger sublimis tendon is identified and gently withdrawn into the proximal forearm incision. The tendon should glide out smoothly; any resistance indicates incomplete release at Camper's chiasm, necessitating a return to the digital incision to complete the release. The sublimis tendon is then passed through the newly fashioned FCU loop. The surgeon must ensure there is no twisting of the tendon within the loop, which could impede excursion.
Using a small hemostat or a specialized tendon carrier, the sublimis tendon is passed subcutaneously across the thenar eminence from the pisiform to the MCP joint of the thumb. The trajectory must be in direct line with the native fibers of the paralyzed APB. The tunnel across the thenar eminence must be strictly subcutaneous. If the tendon is inadvertently passed deep to the palmar fascia, its vector will be fundamentally altered, and it will fail to provide adequate palmar abduction, acting instead as a simple thumb flexor. Conversely, if the tunnel is too superficial and the FCU pulley is inadequate, cosmetically unappealing and mechanically inefficient bowstringing will occur.
Phase 5: The Riordan Dual-Insertion and Tensioning
This final phase dictates the functional success of the entire construct. The distal end of the sublimis tendon is split longitudinally for approximately 2.5 cm (or more if required by the patient's specific anatomy). A small tunnel is created for the first insertion by burrowing between two small parallel incisions in the paralyzed APB tendon. One half of the split sublimis is passed through this tunnel. Next, the extensor aponeurosis is separated from the periosteum of the thumb's proximal phalanx. A small incision is made in the aponeurosis approximately 6 mm distal to the first APB tunnel, and the same strip of sublimis is passed through it. Finally, this slip is brought out from beneath the aponeurosis through a small longitudinal slit made in the EPL tendon, located about 3 mm proximal to the IP joint.
Determining the proper tension is the most demanding and unforgiving aspect of the procedure. The surgeon grasps the two slips of the sublimis with small hemostats and crosses them. The thumb is placed in full opposition and the wrist is held in a straight line (neutral). The overlapping slips are placed under moderate tension. The surgeon then performs the Tenodesis Test: The thumb is released, and the wrist is passively flexed. This maneuver should completely relax the transfer, allowing the thumb to be brought into full extension and abduction passively. Next, the wrist is passively extended to 45 degrees. The tenodesis effect should place enough tension on the transfer to automatically bring the thumb into complete opposition and the tip of the thumb into complete IP extension. If the tension is insufficient, it is adjusted and the test repeated.
Once the correct tension is confirmed, the slips of the sublimis are sutured together and to the surrounding tendinous structures using nonabsorbable sutures, ensuring the cut ends are buried to minimize adhesions. A crucial final step is the Capsular Anchoring: The transfer and the tendon of the APB are anchored to the MCP joint capsule with a single nylon or wire suture. This anchor must be positioned so that the transfer passes directly over the middle of the metacarpal head. This specific anchoring prevents the transferred tendon from displacing toward the palmar aspect of the joint during active opposition, which would alter the moment arm and drastically reduce the mechanical advantage of the transfer.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following a sublimis tendon transfer for thumb opposition can occur, ranging from minor functional deficits to complete failure of the reconstruction. The most frequent complication is under-tensioning of the transfer. Because tendons inherently stretch and relax during the initial healing phase, a transfer that appears perfectly tensioned intraoperatively may become lax postoperatively. This results in a weak pinch, incomplete palmar abduction, and a failure to achieve true tip-to-tip opposition. The intraoperative tenodesis test is the primary defense against this, but if symptomatic under-tensioning persists after a full course of therapy, salvage may require surgical re-exploration, shortening, and re-tensioning of the tendon slip.
Conversely, over-tensioning of the transfer is a less common but arguably more debilitating complication. An over-tensioned opponensplasty results in a fixed flexion and opposition contracture of the thumb. The patient will present with an inability to open the first web space sufficiently to grasp large objects, severely limiting the hand's functional utility. This complication is entirely iatrogenic, stemming from setting the tension with the wrist in excessive extension or failing to perform the relaxation phase of the tenodesis test. Management of a severe over-tension contracture often requires surgical lengthening of the transferred tendon, which is technically challenging and yields unpredictable results.
Donor site morbidity represents another significant category of complications. Harvesting the FDS can lead to proximal interphalangeal (PIP) joint stiffness, a swan-neck deformity (due to loss of the volar stabilizing force of the FDS), or a "lumbrical plus" deformity in the ring finger. The lumbrical plus deformity occurs when the FDS is inadequately separated from the FDP at Camper's chiasm, causing the FDP to pull the lumbrical proximally during attempted finger flexion, paradoxically extending the PIP and DIP joints. Prevention relies on meticulous anatomical dissection at the donor site. Salvage of a lumbrical plus deformity requires a secondary procedure to section the lumbrical tendon of the affected digit.
Bowstringing of the transferred tendon is a cosmetic and functional complication that occurs if the FCU pulley fails or if the subcutaneous tunnel across the thenar eminence is made too superficial. When bowstringing occurs, the moment arm of the transfer is altered, and mechanical efficiency is lost. Prevention requires robust construction of the FCU loop using heavy nonabsorbable sutures and ensuring the tendon is passed deep to the subcutaneous fat but superficial to the palmar fascia. If the pulley ruptures postoperatively, surgical reconstruction of the pulley using a tendon graft or retinacular flap is mandated to restore the correct vector of pull.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Under-tensioning | 10% - 15% | Rigorous intraoperative tenodesis testing, slightly over-tensioning initially | Surgical re-exploration and shortening of the transfer |
| Over-tensioning | 2% - 5% | Ensure full passive thumb extension with wrist flexion intraoperatively | Surgical tendon lengthening or Z-plasty of the transfer |
| Lumbrical Plus Deformity | 1% - 3% | Complete, meticulous release of FDS from FDP at Camper's chiasm | Surgical sectioning of the ring finger lumbrical tendon |
| Pulley Failure / Bowstringing | < 2% | Robust suturing of FCU loop, strict subcutaneous routing | Reconstruction of the pulley using tendon graft or retinaculum |
| Swan-Neck Deformity (Donor) | 5% - 8% | Avoid harvesting FDS in patients with pre-existing PIP hyperextensibility | FDS tenodesis, volar plate advancement, or silver ring splinting |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of a sublimis tendon transfer relies as much on meticulous, phased postoperative rehabilitation as it does on flawless surgical execution. The rehabilitation protocol must balance the competing needs of protecting the fragile tendon repair while preventing restrictive peritendinous adhesions. The protocol is broadly divided into an immobilization phase, a mobilization and motor re-education phase, and a long-term protection phase tailored to the patient's specific functional demands.
Immobilization Phase (Weeks 0-3)
Immediately following wound closure with nonabsorbable sutures, the hand is immobilized in a bulky, compressive dressing reinforced with a rigid dorsal plaster or fiberglass splint. The positioning of the splint is highly specific and critical for protecting the repair. The wrist is placed in approximately 30 degrees of flexion to relieve tension on the transferred sublimis tendon and the FCU pulley. The fingers are placed in a functional position (MCP joints flexed to 70 degrees, IP joints fully extended) to prevent collateral ligament contracture. Crucially, the thumb is immobilized in a position of full opposition with the distal phalanx (IP joint) fully extended, mimicking the desired final functional posture. A few layers of sterile gauze must be placed between the individual fingers to prevent skin maceration during this three-week period of absolute immobilization.
Mobilization and Motor Re-education Phase (Weeks 3-9)
At exactly three weeks postoperative, the initial dressing, splint, and skin sutures are removed. The patient is transitioned to a custom-fabricated thermoplastic opponens splint. This splint must be worn continuously between exercise sessions and at night for an additional six weeks to prevent inadvertent stretching of the healing tendon transfer. Active, therapist-supervised range of motion exercises are initiated.
The cornerstone of this phase is motor re-education. Because the ring finger sublimis was utilized, training the patient to use the transfer is highly intuitive due to the synergistic nature of the donor muscle. The therapist instructs the patient to perform the "Ring Finger Trick": The patient is asked to attempt to place the tip of their thumb against their ring finger. This maneuver naturally produces flexion of the ring finger, which automatically fires the transferred sublimis muscle belly. This synergistic firing results in smooth, coordinated thumb opposition. Many patients achieve active opposition almost immediately upon splint removal using this cognitive shortcut, highlighting the profound advantage of selecting a synergistic donor muscle.
Long-Term Protection and Strengthening (Weeks 9+)
By the ninth postoperative week, the tendon repair has typically achieved sufficient tensile strength to allow for the gradual discontinuation of the daytime opponens splint and the initiation of progressive pinch and grip strengthening exercises. However, the surgeon must identify high-demand patients who require extended protection. In patients with weak quadriceps muscles who habitually rise from a sitting position by pushing up with flattened, extended hands, or in patients who rely heavily on crutches or walkers for ambulation, the transfer is at a high risk of catastrophic stretching. In these specific populations, the transfer must be protected with a rigid, custom-molded splint during all weight-bearing activities for three months or longer. Failure to recognize these unique biomechanical demands and protect the transfer accordingly will inevitably result in an overstretched, non-functional opponensplasty, regardless of the initial surgical success.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the sublimis tendon transfer for thumb opposition is a testament to the iterative refinement of biomechanical principles in hand surgery. The foundational concepts were established by Sterling Bunnell in the early 20th
