Transverse Deficiencies: Arrest of Development & Surgical Management

Key Takeaway
Transverse deficiencies represent a failure of formation in the upper extremity, characterized by the complete absence of parts distal to a specific level. Affecting 6.8 per 10,000 live births, these congenital amputations are predominantly unilateral. Management relies heavily on age-appropriate prosthetic fitting, though surgical interventions, such as the excision of nonfunctional digital nubbins or the Krukenberg reconstruction, are indicated to optimize bimanual function, cosmesis, and tactile sensibility.
Comprehensive Introduction and Patho-Epidemiology
Embryological Foundations and Pathogenesis
Transverse deficiencies of the upper extremity represent a profound failure of formation, specifically categorized as an arrest of development. To comprehend the complexity of these anomalies, the orthopedic surgeon must possess a granular understanding of embryonic limb morphogenesis. The upper limb bud emerges from the lateral plate mesoderm approximately on day 26 of gestation. This highly orchestrated process is governed by a complex, multi-dimensional signaling network that dictates growth along three distinct axes: the proximal-distal, anterior-posterior (radioulnar), and dorsal-ventral axes. The entire framework of the limb is established within a remarkably narrow window, typically concluding by the eighth week of embryonic development.
The primary driver of proximal-distal outgrowth is the Apical Ectodermal Ridge (AER), a specialized multilayered epithelium situated at the distal margin of the limb bud. The AER exerts its influence through the secretion of Fibroblast Growth Factors (specifically FGF-4 and FGF-8), which maintain the underlying mesenchymal cells in a highly proliferative, undifferentiated state known as the Progress Zone. A transverse deficiency is the direct phenotypic result of an early, abrupt cessation of AER function. When the AER signaling is prematurely extinguished—whether due to a localized vascular insult, a teratogenic exposure, or a spontaneous genetic mutation—the underlying mesoderm loses its proliferative drive, resulting in a sudden truncation of the limb at that specific embryological time point.
Concurrently, the Zone of Polarizing Activity (ZPA), located in the posterior margin of the limb bud, regulates the radioulnar axis via Sonic Hedgehog (SHH) expression, while the dorsal ectoderm dictates the dorsal-ventral axis through Wnt-7a signaling. In pure transverse deficiencies, the structural integrity of the limb proximal to the level of amputation is generally well-preserved, indicating that the ZPA and dorsal ectoderm functioned normally until the catastrophic failure of the AER. This sudden arrest distinguishes transverse deficiencies from longitudinal deficiencies (such as radial clubhand), where a specific axis is selectively impaired while proximal-distal growth continues.
Epidemiological Profile and Genetic Considerations
From an epidemiological standpoint, transverse deficiencies are relatively rare but represent a significant proportion of congenital upper limb anomalies. Landmark epidemiological studies, including the seminal work by Wynne-Davies and Lamb, have established the incidence of transverse deficiencies at approximately 6.8 per 10,000 live births. Unlike many other congenital skeletal dysplasias, these anomalies exhibit no distinct sex predilection, affecting males and females with equal frequency. Furthermore, the overwhelming majority of these presentations—approximately 98%—are strictly unilateral, a clinical feature that heavily influences both prosthetic management and surgical decision-making.
The anatomical level of the deficiency is highly variable, but statistical distributions reveal a clear predilection for the proximal third of the forearm. This specific level, often termed a proximal transradial deficiency, accounts for the lion's share of clinical presentations. Deficiencies at the transhumeral, elbow disarticulation, or midcarpal levels are encountered with significantly less frequency. The precise timing of the AER disruption directly correlates with the anatomical level of the truncation; an earlier disruption yields a more proximal amputation, whereas a later disruption results in a more distal deficiency, such as aphalangia or adactylia.
Genetically, transverse deficiencies are overwhelmingly sporadic. Extensive pedigree analyses have consistently failed to demonstrate predictable Mendelian inheritance patterns for the vast majority of these cases. The prevailing pathogenetic theory implicates a spontaneous, localized vascular disruption—analogous to a microvascular chorionic villus hemorrhage—occurring during the critical window of embryogenesis. Teratogenic factors, including misoprostol exposure or early chorionic villus sampling (prior to 10 weeks gestation), have been definitively linked to an increased risk of transverse limb reduction defects, reinforcing the vascular disruption hypothesis over a purely hereditary genetic mutation.
Clinical Presentation and Natural History
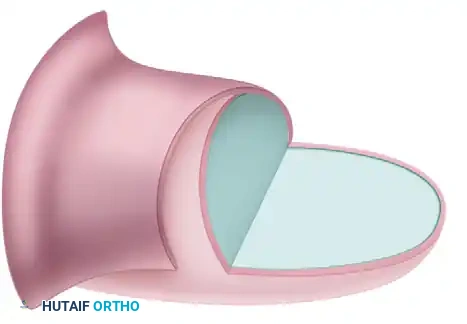
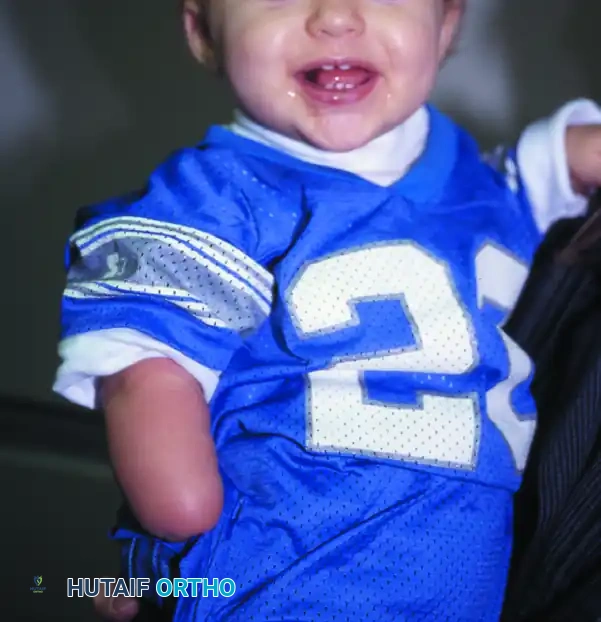
The hallmark clinical presentation of a transverse deficiency is a well-padded, amputation-like stump that terminates abruptly at a specific anatomical level. Unlike traumatic amputations, the congenital stump is typically characterized by redundant, highly mobile soft tissue that provides excellent cushioning over the terminal bone. This robust soft-tissue envelope is highly advantageous for subsequent prosthetic fitting, as it minimizes the risk of terminal bony overgrowth—a complication notoriously common in pediatric traumatic amputations but exceedingly rare in true congenital transverse deficiencies.
A frequent and notable finding at the distal terminus of the stump is the presence of "digital nubbins." These rudimentary soft-tissue appendages are remnants of failed digital ray formation. Clinically, they present as small, flail outpouchings of skin and subcutaneous tissue, occasionally bearing rudimentary fingernails or dimples. While they often lack functional skeletal elements, tendinous insertions, or voluntary motor control, their presence is a critical diagnostic indicator distinguishing a true failure of formation from amniotic band sequence, where the amputation is typically characterized by scarring, syndactyly, or constrictive rings without organized nubbin formation.
The natural history of a child born with a unilateral transverse deficiency is one of remarkable neurodevelopmental adaptation. In the absence of surgical or prosthetic intervention, these children rapidly incorporate the anomalous limb into their body schema, utilizing the stump as a highly effective non-dominant assisting limb. They develop compensatory prehensile strategies, often trapping objects between the stump and the torso or utilizing the stump to stabilize items while the contralateral, fully formed hand performs fine motor manipulation. Understanding this profound natural adaptability is paramount, as any surgical or prosthetic intervention must demonstrably improve upon the child's innate functional baseline.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Relationships
The osteology of a transverse deficiency is defined by the absolute absence of skeletal elements distal to the level of the arrest. In the most common presentation—the proximal transradial deficiency—the humerus, elbow joint, and proximal portions of the radius and ulna are structurally intact and radiographically normal. The proximal radioulnar joint (PRUJ) is typically well-formed, allowing for preserved, albeit sometimes limited, pronation and supination. The preservation of the PRUJ is a critical biomechanical asset, as it permits the active positioning of the terminal stump in space, a function that is heavily leveraged in both prosthetic design and advanced reconstructive procedures like the Krukenberg operation.
In midcarpal or transcarpal deficiencies, the distal radius and ulna, as well as the proximal carpal row, may be present. It is imperative for the orthopedic surgeon to recognize that the carpal bones remain entirely cartilaginous and radiolucent until approximately 6 to 8 months of age. Consequently, early radiographs may falsely suggest a more proximal level of deficiency. The presence of these cartilaginous anlagen is highly prognostic, as they ensure continued longitudinal growth of the distal radius and ulna via their respective physes, preventing the severe forearm shortening seen in more proximal arrests.
Biomechanically, the terminal bone in a congenital deficiency behaves differently than a surgically amputated bone. The medullary canal is typically closed and rounded off with a smooth cortical cap, covered by a thick periosteal sleeve. This anatomical configuration prevents the phenomenon of terminal bony overgrowth (appositional bone growth piercing the skin), which plagues pediatric traumatic amputees. Therefore, prophylactic surgical capping of the bone ends (such as with epiphyseal transplants or synthetic caps) is rarely, if ever, indicated in the virgin congenital transverse deficiency.
Myology and Muscular Rebalancing
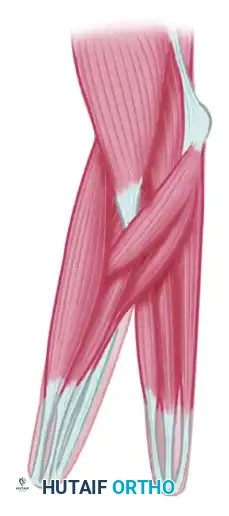
The muscular anatomy proximal to the level of the deficiency is subject to significant variation, dictated entirely by the level of the embryological arrest. Muscles that normally originate proximal to the amputation but insert distal to it (e.g., the long flexors and extensors of the digits in a transradial deficiency) are present but lack their normal distal tendinous insertions. Instead, these muscle bellies typically converge and insert directly into the deep fascia of the terminal stump, creating a robust, unified myofascial envelope.
This anomalous insertion pattern is of profound clinical significance, particularly when contemplating myoelectric prosthetic fitting or surgical reconstruction. Because the flexor and extensor muscle masses remain distinct and are firmly anchored to the terminal fascia, they retain their ability to contract isometrically. This isometric contraction generates robust electromyographic (EMG) signals that can be reliably harvested by surface electrodes in a myoelectric prosthesis. The surgeon must respect this myofascial continuity; injudicious excision of terminal soft tissue during nubbin removal can inadvertently detach these muscle insertions, severely degrading the patient's myoelectric potential.
In the context of the Krukenberg procedure, understanding the precise myology of the forearm is the absolute crux of the operation. The procedure demands the longitudinal division of the forearm into a radial and an ulnar ray. The pronator teres is the biomechanical linchpin of this reconstruction; it must remain meticulously attached to the radius to serve as the primary motor for active pincer closure. The remaining flexor and extensor wads are carefully segregated to provide balanced antagonistic forces, ensuring that the newly created rays can actively open and close without succumb to progressive flexion or extension contractures.
Neurovascular Topography in the Anomalous Limb
The neurovascular anatomy of a transverse deficiency generally mirrors the skeletal truncation. The major arterial trunks (brachial, radial, and ulnar arteries) and peripheral nerves (median, ulnar, and radial nerves) follow their normal anatomical courses until they reach the terminal stump. At the distal terminus, the vessels typically arborize into a rich, plexiform subcutaneous network that supplies the redundant soft-tissue envelope. This robust vascularity guarantees excellent healing potential for any surgical incisions made at the stump level.
The peripheral nerves terminate in organized, microscopic neuromas embedded within the deep fascia and subcutaneous tissue. Unlike traumatic neuromas, which are often tethered to scar tissue and exquisitely painful, these congenital terminal neuromas are typically asymptomatic and well-cushioned. They provide the stump with excellent protective and tactile sensibility. Preservation of this terminal sensibility is a paramount surgical principle; any intervention that compromises the sensory feedback of the stump fundamentally degrades the limb's utility, even if it achieves a perceived cosmetic improvement.
When rudimentary digital nubbins are present, they frequently contain distinct, albeit microscopic, neurovascular bundles branching from the terminal median or ulnar nerves. This is a critical anatomical trap for the unwary surgeon. If a nubbin is simply amputated at its base without formal identification and proximal retraction of these tiny nerves, a painful, symptomatic neuroma can develop directly beneath the surgical scar. Such an iatrogenic complication will render the stump intolerant to the socket of a prosthesis, transforming a functional, painless anomaly into a profound source of morbidity.
Exhaustive Indications and Contraindications
Surgical Thresholds and Non-Operative Paradigms
The overarching philosophy in the management of transverse deficiencies is heavily weighted toward non-operative, prosthetic, and adaptive interventions. The indications for surgical intervention are exceptionally narrow and must be justified by a clear, predictable enhancement of the child's functional independence or the facilitation of prosthetic wear. The orthopedic surgeon must resist the temptation to operate solely for the purpose of normalizing the limb's appearance, as aesthetic procedures that compromise sensation, mobility, or soft-tissue padding are universally detrimental to the patient's long-term outcomes.
For the vast majority of unilateral transverse deficiencies, the definitive treatment is the timely prescription of an age-appropriate prosthesis, coordinated with intensive occupational therapy. The "sit to fit" protocol dictates that a passive prosthesis should be introduced when the infant achieves independent sitting balance (typically between 3 to 6 months of age). This early introduction fosters cortical integration of the device and promotes symmetrical bimanual motor development. Surgery is strictly contraindicated in this cohort unless specific anatomical impediments to prosthetic fitting exist.
Conversely, the indications for advanced surgical reconstruction, specifically the Krukenberg procedure, are reserved for a highly specific and profoundly affected patient population. The classic, absolute indication for a Krukenberg reconstruction is a patient with bilateral below-elbow amputations who is concurrently blind or severely visually impaired. In this scenario, conventional prostheses are entirely inadequate because they deprive the patient of tactile feedback—the only remaining sensory modality available for environmental interaction. By converting the forearm into a sensate pincer, the Krukenberg procedure restores prehension while preserving critical tactile sensibility, representing a life-altering functional salvage.

Matrix of Indications and Contraindications
| Procedure / Intervention | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Passive Prosthetic Fitting | Unilateral/bilateral deficiency; infant achieving sitting balance (3-6 months). | Severe skin breakdown or active infection at the stump interface. | Unsupportive family environment lacking commitment to OT protocols. |
| Myoelectric Prosthesis | Preschool age (2-4 years); adequate isometric muscle contraction (EMG signal). | Lack of distinct flexor/extensor EMG signals; severe cognitive delay. | Heavy manual labor environments where device durability is a concern. |
| Excision of Digital Nubbins | Flail, non-functional nubbins causing psychological distress or interfering with prosthetic socket fit. | Nubbins possessing underlying skeletal continuity and voluntary motor control. | Patient/family prioritizing minor tactile input over cosmetic appearance. |
| Krukenberg Procedure | Bilateral below-elbow amputations; concomitant blindness/visual impairment; lack of prosthetic access. | Unilateral deficiency (functionally inferior to a standard prosthesis); absent pronator teres. | Severe elbow contracture; inadequate cognitive capacity for sensory re-education. |
| Bone Capping / Revision | True terminal bony overgrowth causing skin tenting or ulceration (rare in congenital). | Asymptomatic stump; routine prophylaxis in a virgin congenital limb. | Active stump infection; inadequate soft tissue for tension-free closure. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Radiographic Assessment
Meticulous pre-operative planning begins with a comprehensive clinical and radiographic evaluation of the anomalous limb. The surgeon must meticulously document the active and passive range of motion of all proximal joints, particularly the elbow and shoulder, as well as the presence of any residual radioulnar pronation and supination. The soft-tissue envelope of the stump must be assessed for mobility, redundancy, and the presence of terminal sensory feedback. Any digital nubbins must be carefully palpated to detect underlying cartilaginous or bony structures.
Radiographic evaluation is mandatory, even when the clinical level of amputation appears obvious. Standard orthogonal views (anteroposterior and lateral) of the affected limb, including the joint proximal to the deficiency, must be obtained. In infants and young children, the surgeon must account for the delayed ossification of the carpal and epiphyseal elements. High-resolution ultrasonography or magnetic resonance imaging (MRI) can be invaluable adjuncts in characterizing the cartilaginous anlagen within the stump or assessing the continuity of flexor and extensor muscle masses when planning for myoelectric prosthetic fitting or a Krukenberg reconstruction.
When evaluating digital nubbins for potential excision, the radiographic confirmation of an entirely flail, soft-tissue composition is a prerequisite for surgery. If radiographs or ultrasound reveal skeletal continuity with the proximal stump, or if the child demonstrates voluntary motor control over the nubbin, excision is strictly contraindicated. Such functional appendages, regardless of their aesthetic appearance, must be preserved and leveraged to maximize the child's tactile and prehensile capabilities.
Prosthetic Interface Considerations
Surgical planning cannot occur in a vacuum; it must be intimately coordinated with a certified prosthetist and an occupational therapist. The ultimate goal of any soft-tissue contouring or nubbin excision is to optimize the limb for a prosthetic socket. The surgeon and prosthetist must collaboratively determine the ideal stump morphology. Redundant soft tissue, while beneficial for padding, can occasionally create a "bulbous" terminus that makes donning and doffing a rigid prosthetic socket difficult.
In such cases, the surgical plan may involve a conservative defatting or contouring of the stump concurrently with the nubbin excision. However, the surgeon must exercise extreme caution to avoid over-resection, which can leave the terminal bone inadequately padded and vulnerable to breakdown under the sheer forces of a prosthetic socket. The placement of surgical incisions is also critical; scars should be designed to fall outside the primary weight-bearing or contact zones of the anticipated prosthetic interface to prevent painful friction blisters or ulcerations.
Anesthesia, Positioning, and Tourniquet Application
Surgical interventions for transverse deficiencies are performed under general anesthesia, tailored to the pediatric patient by a specialized pediatric anesthesiologist. Regional anesthesia (such as a supraclavicular or axillary brachial plexus block) is highly recommended as an adjunct for postoperative pain management, reducing the reliance on systemic opioids and facilitating a smoother emergence from anesthesia.
The patient is positioned supine on the operating table. For unilateral procedures, the affected limb is extended onto a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm (or the proximal humerus in the case of a transradial deficiency) over a layer of cast padding. Exsanguination is achieved via elevation or the application of an Esmarch bandage, followed by tourniquet inflation to an age- and size-appropriate pressure (typically 100 mmHg above systolic blood pressure, not exceeding 250 mmHg in pediatric patients).
For the Krukenberg procedure, meticulous positioning and lighting are paramount. The use of surgical loupe magnification (typically 3.5x to 4.5x) is mandatory to facilitate the precise identification and protection of the microvascular and neural structures during the longitudinal splitting of the forearm. A sterile marking pen is utilized to meticulously design the complex skin flaps prior to the initial incision, ensuring adequate soft-tissue coverage for the newly created radial and ulnar rays.
Step-by-Step Surgical Approach and Fixation Technique
Excision of Digital Nubbins and Soft Tissue Contouring
The excision of nonfunctional digital nubbins, while conceptually simple, demands rigorous adherence to plastic surgery principles to prevent catastrophic prosthetic interface complications. The procedure begins with the design of an elliptical incision at the base of the nubbin. The long axis of the ellipse should ideally be oriented transversely or obliquely to align with the natural skin tension lines of the stump, ensuring a cosmetically acceptable and biomechanically sound scar.
Upon incising the skin, the surgeon must proceed with meticulous, magnified dissection. The subcutaneous tissue is carefully spread to identify the rudimentary neurovascular bundles that invariably supply the nubbin. These structures, though microscopic, are of paramount clinical importance. Once identified, the tiny nerves must be isolated, placed under gentle distal traction, sharply transected, and allowed to retract deeply into the well-padded soft tissue of the proximal stump. This proximal retraction is the critical step in preventing the formation of a symptomatic terminal neuroma.
Following the management of the neurovascular elements, the base of the nubbin is excised. If a prominent fascial defect remains, it is repaired with fine, absorbable suture to prevent soft-tissue herniation. The skin is then meticulously reapproximated using deep dermal interrupted sutures and a running subcuticular closure with an absorbable monofilament (e.g., 5-0 Monocryl). The use of absorbable sutures is highly preferred in the pediatric population to eliminate the psychological trauma and logistical difficulty of suture removal in the clinic.
The Krukenberg Reconstruction Incision and Exposure
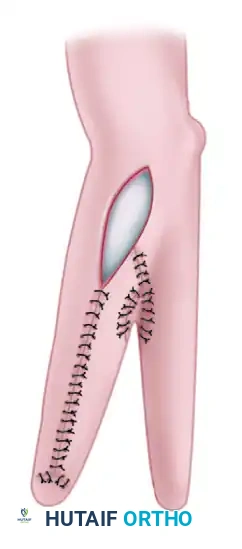
The Krukenberg procedure is a formidable, limb-salvaging operation that requires an intimate knowledge of forearm anatomy. The objective is to longitudinally bisect the forearm, creating an independent radial ray and an ulnar ray that function as a sensate pincer. The procedure commences with the precise marking of the skin incisions.

A longitudinal incision is designed on the flexor (volar) aspect of the forearm, positioned slightly ulnar to the true midline. A corresponding longitudinal incision is marked on the dorsal surface. The placement of these incisions is critical; they must yield skin flaps of sufficient width to circumferentially wrap the opposing (inner) surfaces of the newly created rays. Preserving normal, sensate skin on these opposing surfaces is the absolute prerequisite for the functional success of the pincer grasp.
The incisions are carried down through the dermis and subcutaneous tissue to the level of the deep antebrachial fascia. Broad, full-thickness fasciocutaneous flaps are elevated radially and ulnarly. The surgeon must maintain a meticulous hemostatic field, utilizing bipolar electrocautery to control perforating vessels while preserving the primary axial blood supply to the skin flaps.
Myofascial Separation and Neurovascular Protection
Once the deep fascia is exposed, it is incised longitudinally, revealing the underlying flexor and extensor muscle masses. The most technically demanding phase of the operation—the segregation of the musculature into a radial and an ulnar motor group—now begins.

The flexor mass is addressed first. The flexor carpi radialis (FCR) and the radial half of the flexor digitorum sublimis (FDS) are mobilized radially. The flexor carpi ulnaris (FCU) and the ulnar half of the FDS are mobilized ulnarly. During the longitudinal splitting of the FDS, the surgeon must exercise extreme vigilance to identify and protect the median nerve, which lies immediately deep to this muscle belly. Iatrogenic injury to the median nerve at this juncture will result in catastrophic denervation and loss of tactile sensibility to the radial ray, entirely defeating the purpose of the operation.
The dissection proceeds deeply to expose the interosseous membrane. The pronator teres, the absolute critical motor for pincer closure, is identified and meticulously preserved on its radial insertion. The interosseous membrane is then sharply divided longitudinally from its distal margin to the proximal radioulnar joint. The anterior and posterior interosseous vessels are carefully ligated and divided to allow for the wide separation of the radius and ulna.
The extensor mass is subsequently divided. The brachioradialis, extensor carpi radialis longus and brevis (ECRL/ECRB), and the radial half of the extensor digitorum communis (EDC) are grouped with the radius. The extensor carpi ulnaris (ECU) and the ulnar half of the EDC are grouped with the ulna. This precise allocation of musculature ensures that both the radial and ulnar rays possess balanced flexor and extensor forces, preventing late postural contractures of the pincer.
Skin Closure and Grafting Strategies
With the radius and ulna fully mobilized and capable of wide abduction, the tourniquet is deflated, and meticulous hemostasis is achieved. The previously elevated fasciocutaneous flaps are now wrapped around the opposing (inner)
Clinical & Radiographic Imaging Archive