Opening Wedge Osteotomy and Surgical Management of the Delta Phalanx

Key Takeaway
The opening wedge osteotomy of the terminal phalanx is a highly effective surgical intervention for correcting progressive angular deformities, such as clinodactyly and delta phalanx. This procedure restores digital alignment by utilizing a dorsal periosteal hinge and precise diaphyseal cuts. When combined with physiolysis or fat interposition in pediatric patients, it prevents progressive deformity, optimizes biomechanics, and ensures excellent long-term functional and aesthetic outcomes in the hand.
Comprehensive Introduction and Patho-Epidemiology
Angular deformities of the digits in the frontal plane, clinically referred to as clinodactyly, present a uniquely complex reconstructive challenge in both pediatric and adult hand surgery. While mild angulation is frequently observed in the general population and is often entirely asymptomatic, severe progressive deformity can lead to profound functional impairment, restricted range of motion, and unacceptable aesthetic outcomes. The clinical manifestation of clinodactyly involves a deviation of the digit away from its normal longitudinal axis, most commonly occurring at the distal interphalangeal (DIP) joint. When this deviation exceeds 10 to 15 degrees, the mechanical axis of the digit is altered, leading to overlapping digits during functional grip and subsequent impairment of fine motor dexterity.
The most common pathoanatomic etiology for severe, progressive clinodactyly is the presence of a delta phalanx, a condition more accurately and descriptively termed a longitudinally bracketed epiphysis (LBE). This congenital anomaly represents a failure of normal physeal development, wherein the growth plate does not remain confined to the proximal transverse base of the phalanx but instead extends longitudinally along the diaphysis, eventually bridging the proximal and distal epiphyses. This anomaly most frequently manifests in the middle phalanx of the small finger and the proximal phalanx of the thumb, the latter often presenting in association with a triphalangeal thumb. The next most frequent location is the proximal phalanx of the ring finger. In border digits, the presence of a delta phalanx invariably causes the finger to deviate toward the midline of the hand, producing classic radial deviation of the small finger or ulnar deviation of the thumb.
Epidemiologically, the delta phalanx can occur as an isolated, sporadic anomaly or as a component of a broader genetic syndrome. It exhibits an autosomal dominant inheritance pattern with variable penetrance and expressivity when presenting as an isolated familial trait. Syndromic associations are well-documented and include Rubinstein-Taybi syndrome, Apert syndrome, Carpenter syndrome, Holt-Oram syndrome, and trisomy 21 (Down syndrome). In syndromic cases, the delta phalanx is often bilateral and may involve multiple digits, complicating the reconstructive algorithm. The true incidence of the delta phalanx in the general population remains difficult to ascertain definitively, as mild, asymptomatic cases frequently go undiagnosed; however, it is recognized as a leading cause of pediatric hand consultations for digital deformity.
Because progressive angulation is an inevitable biomechanical consequence in the presence of a true delta phalanx, nonoperative management, such as splinting or physical therapy, is universally ineffective and contraindicated as a primary treatment modality. The tethering effect of the bracketed epiphysis dictates that the deformity will worsen with skeletal growth. Therefore, operative intervention is mandated for moderate to severe cases. The primary surgical goals are to narrow the abnormally widened digit, straighten the mechanical axis of the phalanx, ablate the abnormal tethering portion of the epiphysis to prevent recurrence, and restore a functional, aesthetically acceptable digit. This comprehensive chapter details the opening wedge osteotomy of the terminal phalanx as described by Carstam and Eiken, alongside the contemporary, age-based management of the delta phalanx utilizing physiolysis and osteotomy techniques pioneered by Vickers, and further refined by Strauss and Goldfarb.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the aberrant surgical anatomy and the resulting biomechanical tethering caused by the delta phalanx is absolutely critical for successful surgical correction. The normal tubular bones of the hand, including the phalanges, possess a single, transverse proximal physis responsible for longitudinal growth. The distal end of the phalanx is characterized by a non-growing articular surface or, in the case of the distal phalanx, the ungual tuberosity. Normal longitudinal growth proceeds symmetrically, maintaining the rectilinear alignment of the diaphysis.
In stark contrast, a delta phalanx is characterized by a continuous, C-shaped or bracketed physis that runs longitudinally along one side of the diaphysis, effectively connecting the proximal and distal epiphyses. This abnormal physeal bracket restricts longitudinal growth on the affected, tethered side while allowing continued, relatively normal growth on the contralateral, unbracketed side. The biomechanical result of this asymmetric growth is a progressive, trapezoidal or triangular (delta) shaping of the bone. The diaphysis becomes wedge-shaped, and the adjacent joint surfaces become non-parallel, leading to severe angular deviation of the entire digit distal to the anomaly.
The longitudinally bracketed epiphysis acts as an unyielding biomechanical tether. As the normal side of the physis continues to proliferate and expand longitudinally, the bracketed side acts as a fixed hinge. This forces the digit into progressive clinodactyly, with the apex of the deformity pointing away from the tethered side. The soft tissue envelope, including the neurovascular bundles, collateral ligaments, and extensor and flexor tendons, adapts to this skeletal deformity over time. The collateral ligament on the concave side of the deformity becomes contracted, while the ligament on the convex side becomes attenuated. The extensor mechanism may subluxate, further exacerbating the deformity and complicating surgical correction. Surgical intervention must directly address this tethering effect; it must either destroy the tether entirely through physiolysis to allow for spontaneous remodeling, or correct the established, rigid bony deformity through an osteotomy.
Vascular anatomy is of paramount importance when planning surgical interventions on the delta phalanx. The digital arteries course volarly and laterally along the digit, sending critical transverse branches to supply the phalangeal diaphysis and the physeal plates. The surgical approach must meticulously preserve these neurovascular structures. Furthermore, the periosteal blood supply is vital for the survival and consolidation of any subsequent osteotomy or bone graft. The dorsal periosteum, in particular, plays a crucial role in the opening wedge osteotomy technique, where it is intentionally preserved to act as a vascularized hinge and a biomechanical tension band. Disruption of this delicate vascular network can lead to devastating complications, including avascular necrosis of the phalangeal fragments, nonunion, or complete digital loss.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for a delta phalanx must be based on a meticulous evaluation of the patient's functional impairment, the magnitude of the angular deformity, the remaining skeletal growth potential, and the presence of any associated syndromic anomalies. Not all delta phalanges require surgical correction; mild, non-progressive deformities that do not interfere with hand function may be observed. However, a structured approach is essential to identify those patients who will benefit from early intervention to prevent severe, irreversible deformity.
The primary indication for surgical intervention is progressive angular deformity (clinodactyly) that exceeds 20 to 25 degrees in the frontal plane. Deformities of this magnitude frequently cause the affected digit to cross over or under adjacent digits during active flexion, significantly impairing grip strength, fine motor dexterity, and overall hand function. Furthermore, severe aesthetic concerns, particularly in border digits, represent a valid indication for surgery, as the psychosocial impact of a visibly deformed hand can be profound for both the child and the parents. The timing of the intervention is dictated by the patient's age and the specific procedure planned, with physiolysis indicated for younger children with substantial remaining growth potential, and osteotomy reserved for older children and adults with established bony deformity.
Contraindications to surgical intervention must be carefully considered to avoid unnecessary morbidity. Absolute contraindications include the presence of active local or systemic infection, severe vascular compromise of the affected digit, or medical comorbidities that preclude safe administration of anesthesia. Relative contraindications include mild, asymptomatic deformities (less than 15-20 degrees) that do not impair function, or severe syndromic anomalies where the overall functional capacity of the hand is so profoundly limited that correction of a single digit will not yield a meaningful improvement in quality of life. In cases of central polydactyly associated with a delta phalanx, simple osteotomy is contraindicated; the abnormal phalanx should be excised entirely along with the extra digit, followed by a syndactyly-type reconstruction.
Indications and Contraindications Summary Table
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Absolute Indications | Progressive angulation > 25 degrees | Prevents irreversible joint contracture and severe functional crossover during grip. |
| Absolute Indications | Functional impairment (digit crossover) | Restores normal digital cascade and prehension mechanics. |
| Relative Indications | Angulation between 15-25 degrees | Considered if aesthetic concerns are profound or if rapid progression is documented. |
| Relative Indications | Triphalangeal thumb with delta phalanx | Requires excision of the delta phalanx and meticulous ligamentous reconstruction to restore thumb stability. |
| Absolute Contraindications | Active local or systemic infection | High risk of osteomyelitis, graft failure, and catastrophic digital loss. |
| Absolute Contraindications | Severe vascular compromise | Surgical dissection and osteotomy may precipitate digital ischemia and necrosis. |
| Relative Contraindications | Mild, non-progressive deformity (< 15 degrees) | Functional impairment is minimal; surgical risks outweigh potential benefits. |
| Relative Contraindications | Severe syndromic hand anomalies | Correction of a single digit may not improve overall global hand function. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful surgical correction of the delta phalanx. The initial step involves a comprehensive radiographic assessment. Standard posteroanterior (PA), true lateral, and oblique radiographs of the affected digit are mandatory. It is critical that the PA radiograph is a "true" PA of the individual digit, rather than a standard PA of the entire hand, as the rotational position of the affected digit can distort the apparent magnitude of the angular deformity. The PA radiograph will clearly demonstrate the pathognomonic trapezoidal or triangular shape of the phalanx and the continuous, C-shaped radiolucent line representing the bracketed epiphysis.
Once high-quality radiographs are obtained, precise templating must be performed. The surgeon must calculate the exact angle of the deformity by drawing lines parallel to the proximal and distal articular surfaces of the affected phalanx; the intersection of these lines yields the angle of correction required. For an opening wedge osteotomy, this angle dictates the size of the wedge that must be created to restore rectilinear alignment. The surgeon must also anticipate the need for bone grafting. If a large opening wedge is planned, particularly in older children or adults, structural autograft (typically harvested from the distal radius or iliac crest) or allograft must be available to fill the defect, provide structural stability, and promote osseous consolidation.
The age-based treatment algorithm, as refined by Strauss and Goldfarb, is a critical component of preoperative planning. The timing of surgical intervention dictates the choice of procedure. For children under 5 years of age, a Vickers-type procedure (physiolysis with fat interposition) is the recommended primary approach. Resecting the abnormal physeal bracket early in life removes the biomechanical tether, allowing the substantial remaining growth potential of the phalanx to facilitate spontaneous angular correction and normalized longitudinal growth. For children over 5 years of age and adults, the remaining growth potential is insufficient for spontaneous correction following physiolysis alone. In these patients, an opening wedge osteotomy (with or without concurrent physiolysis and bone grafting) is strictly required to correct the established osseous deformity.
Patient positioning and operating room setup must be optimized for precision and safety. The patient is placed supine on the operating table with the affected upper extremity extended on a radiolucent hand table. General anesthesia is typically preferred for pediatric patients to ensure complete immobility, while regional anesthesia (such as a supraclavicular or axillary block) may be utilized for older, compliant adolescents or adults. A well-padded pediatric or digital tourniquet is applied to ensure an absolutely bloodless surgical field, which is essential for identifying the delicate physeal anatomy and protecting the neurovascular bundles. Loupe magnification (minimum 2.5x to 3.5x) is highly recommended, and a mini-C-arm fluoroscopy unit must be positioned appropriately for intraoperative imaging to confirm osteotomy placement, wedge opening, and hardware trajectory.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of the delta phalanx requires a nuanced, highly technical approach that varies based on the patient's age and the specific procedure indicated. The following sections detail the comprehensive sequence, incorporating the principles of the Vickers physiolysis for younger children and the opening wedge osteotomy for older patients, as well as the combined approach described by Strauss and Goldfarb.
Phase 1: Identification of the Deformity and Surgical Exposure
Under strict tourniquet control, the surgical approach begins with a precise incision. A radial or ulnar midlateral incision is typically preferred over the affected phalanx, chosen based on the side of the bracketed epiphysis (usually the concave side of the deformity). This midlateral approach avoids the creation of volar or dorsal scars that could lead to flexion or extension contractures.
Careful dissection is carried through the subcutaneous tissues. The surgeon must meticulously identify and protect the terminal branches of the digital nerve and artery, mobilizing them and retracting them volarly. The extensor mechanism is identified and retracted dorsally. The periosteum is then incised longitudinally, and the phalanx is exposed via meticulous subperiosteal dissection. The initial exposure reveals the classic delta phalanx morphology. The longitudinally bracketed epiphysis is clearly visible as a cartilaginous band tethering the diaphysis, preventing normal longitudinal growth on the affected side.
This biomechanical tethering results in the characteristic angular deformity (clinodactyly) in the frontal plane, which is now fully appreciated under direct visualization. The apex of the deformity points away from the tethered side, and the shortened, concave aspect of the phalanx is dominated by the abnormal physeal tissue.
Phase 2: Physiolysis (The Vickers Procedure)
For children under 5 years of age, resection of the abnormal physeal bracket (physiolysis) is the definitive treatment of choice. The objective is to completely ablate the tethering mechanism, allowing the phalanx to remodel spontaneously over subsequent years of growth.

Using a sharp scalpel (such as a #15 blade) or a fine micro-osteotome, the surgeon begins the precise resection of the isthmus of the continuous epiphysis. The goal is to completely ablate the abnormal physeal tissue that bridges the proximal and distal ends of the bone. Magnification is crucial here to differentiate the pearly white physeal cartilage from the adjacent metaphyseal bone.

The resection must be carried deeply into the medullary canal of the bone to ensure that absolutely no residual physeal cells remain. Incomplete resection is the primary cause of procedure failure; any retained physeal tissue will inevitably lead to the reformation of a physeal bar and rapid recurrence of the angular deformity. The surgeon must visually confirm that normal cancellous bone is exposed at the base of the resection trough.

Once the bracket is fully and aggressively excised, a distinct, deep gap is created in the lateral aspect of the phalanx. The biomechanical tethering effect is now completely released. The bone now possesses the potential to remodel and grow symmetrically, driven by the remaining normal proximal physis.
Phase 3: Fat Interposition
Following complete physiolysis, a critical step is required to prevent the bone from healing across the freshly created resection gap. If left empty, hematoma will organize, and osteogenic cells will rapidly reform a bony or physeal bridge, recreating the tether.

To prevent this, an interpositional material must be placed. A free fat graft is harvested—typically from a separate small incision over the hypothenar eminence or the proximal volar forearm. The fat graft is meticulously sized and densely packed into the resection defect. This fat interposition acts as a permanent biologic spacer, inhibiting osteogenesis and permanently preventing the reformation of the bony/physeal bridge. The periosteum is loosely closed over the fat graft, if possible, to hold it in place.
Phase 4: Opening Wedge Osteotomy and Fixation (For Older Children and Adults)
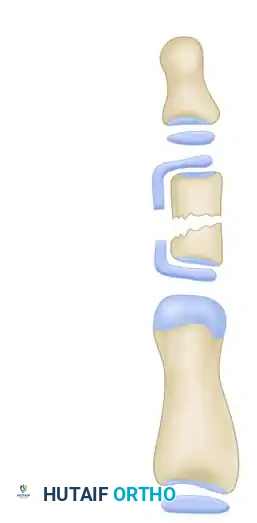
If the patient is older than 5 years, physiolysis alone is fundamentally insufficient because the remaining growth potential cannot spontaneously correct the established, rigid angular deformity. In these cases, an opening wedge osteotomy must be performed to acutely correct the mechanical axis.
To execute the osteotomy, two transverse cuts are made through the volar three-fourths of the diaphysis using a fine oscillating saw or a sharp micro-osteotome. CRITICAL STEP: The surgeon must leave the dorsal periosteum and the dorsal one-fourth of the bony cortex entirely intact. This creates a vital periosteal hinge. This hinge acts as a tension band during the opening of the wedge, prevents catastrophic displacement of the distal fragment, and provides absolute control over the rotation of the fragments.
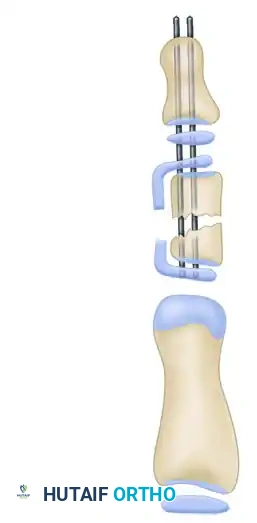
A gentle opening force is applied to correct the angular deformity, utilizing the intact dorsal hinge to guide the correction. Complete correction may occasionally be blocked by a severe, curved nail deformity; in such cases, the nail matrix may require partial elevation from the underlying periosteum. Once anatomic, rectilinear alignment is achieved, the correction is rigidly stabilized. A longitudinal Kirschner wire (K-wire) (typically 0.028 or 0.035 inch) is driven retrograde through the tip of the distal phalanx, across the osteotomy site, and across the distal interphalangeal (DIP) joint. For extremely small phalanges where an intramedullary wire might shatter the bone, a K-wire can be inserted extraperiosteally along the volar aspect to act as an internal splint. If a large opening wedge is created, structural bone graft (autograft or allograft) is meticulously shaped and inserted into the void to promote rapid osseous union.
Complications, Incidence Rates, and Salvage Management
While the surgical management of the delta phalanx is generally highly successful when executed with precision, orthopedic surgeons must be acutely aware of potential complications and be prepared to manage them effectively. Complications can arise from technical errors during the procedure, failure of biological healing, or the inherent complexity of the congenital deformity itself.
The most frequent complication is the recurrence of the angular deformity. This is particularly common following a Vickers physiolysis procedure if the abnormal physeal bracket is incompletely resected, or if the fat interposition fails or extrudes, leading to the rapid reformation of a tethering physeal bar. Recurrence rates in the literature vary but can approach 10-15% if meticulous technique is not strictly adhered to. When recurrence occurs, it typically necessitates a revision procedure, often requiring a definitive opening or closing wedge osteotomy once the patient approaches skeletal maturity.
Nonunion or delayed union of the osteotomy site is a rare complication in the highly osteogenic pediatric population, but it can occur, particularly in older adolescents or adults. The risk of nonunion is significantly increased if the critical dorsal periosteal hinge is completely violated during the saw cuts, leading to instability, or if the K-wire fixation is inadequate. Management of an established nonunion requires a secondary surgical intervention involving debridement of the nonunion site, rigid internal fixation (often upgrading from K-wires to micro-plates if size permits), and the application of autologous cancellous bone graft.
Nail bed deformities represent a frustrating aesthetic and functional complication. Aggressive dissection dorsally, failure to respect the sterile matrix, or failure to address a pre-existing curved nail deformity during the osteotomy correction can lead to permanent ridging, splitting, or complete loss of the nail plate. Furthermore, prolonged transarticular K-wire fixation across the DIP joint can lead to temporary or permanent joint stiffness. To mitigate this, pins should be removed promptly at 4 to 6 weeks once clinical union is achieved, followed by aggressive range of motion therapy.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Deformity Recurrence | 10 - 15% | Incomplete physiolysis; failure of fat interposition; early pin removal. | Revision osteotomy at skeletal maturity; repeat physiolysis rarely effective. |
| Nonunion / Delayed Union | < 5% | Violation of dorsal periosteal hinge; unstable fixation; inadequate bone grafting. | Revision open reduction, rigid fixation (micro-plate if possible), autologous bone grafting. |
| Nail Bed Deformity | 5 - 10% | Iatrogenic injury to germinal matrix; failure to release tethered nail matrix. | Nail bed reconstruction; matrix grafting; often difficult to fully salvage aesthetically. |
| Joint Stiffness (DIPJ) | 15 - 20% | Prolonged transarticular K-wire fixation (> 6 weeks); lack of postoperative therapy. | Aggressive hand therapy; dynamic splinting; rarely requires surgical capsulotomy. |
| Pin Tract Infection | 5 - 8% | Poor local hygiene; prolonged K-wire retention. | Oral antibiotics; local pin care; early pin removal if infection tracks deeply to bone. |
Phased Post-Operative Rehabilitation Protocols
Meticulous, phased postoperative care is absolutely essential to ensure successful bony union, prevent hardware complications, and avoid devastating stiffness in the adjacent interphalangeal joints. The rehabilitation protocol must be tailored to the patient's age, compliance level, and the specific surgical technique utilized.
Phase 1: Immediate Postoperative Immobilization (Weeks 0 to 4)
Immediately following the surgical procedure, the affected digit is immobilized in a protective, rigid splint. For pediatric patients, who are inherently non-compliant with activity restrictions, a well-padded long-arm cast extending to include the affected digit is often preferred. This prevents accidental removal of the splint, protects the protruding K-wires from trauma, and ensures absolute immobilization of the osteotomy site. The primary goals during this phase are pain control, edema management through strict elevation, and the prevention of pin tract infections. Pin sites must be kept clean and dry; if left exposed, daily cleansing with chlorhexidine or dilute hydrogen peroxide is mandated.
Phase 2: Clinical Union and Hardware Removal (Weeks 4 to 6)
At approximately 4 to 6 weeks postoperatively, the patient returns for critical clinical and radiographic evaluation. Serial radiographs are obtained to assess the maintenance of angular alignment and to evaluate the progression of bony healing at the osteotomy site. The surgeon looks for signs of bridging callus formation or the obliteration of the osteotomy line. Once clinical stability and radiographic signs of early union are evident, the K-wires are removed in the outpatient clinic setting. Prolonging transarticular fixation beyond 6 weeks significantly increases the risk of permanent DIP joint stiffness and should be avoided unless absolutely necessary for delayed unions.
Phase 3: Mobilization and Functional Restoration (Weeks 6 to 12)
Following pin removal, the rigid immobilization is discontinued. Usually, no specific, intensive postoperative hand therapy is necessary for isolated terminal phalanx osteotomies in young children, as they naturally resume use of the hand. However, for older children and adults, a formal hand therapy program is highly recommended. Active and passive range of motion exercises for the DIP and proximal interphalangeal (PIP) joints are initiated immediately. Dynamic flexion or extension splinting may be employed if residual stiffness is noted. Full, unrestricted activities, including contact sports and heavy manual labor, are permitted only gradually, guided by the final radiographic consolidation of the osteotomy, typically achieved by 10 to 12 weeks postoperatively. Long-term follow-up is required annually until skeletal maturity to monitor for late recurrence or growth arrest.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for the delta phalanx is deeply rooted in several landmark publications that have fundamentally shaped contemporary orthopedic practice. Understanding this literature provides the necessary context for the current standard of care.
The conceptual foundation for addressing the physeal tether was established by Vickers in 1987. His seminal paper described the physiolysis technique, demonstrating that early excision of the abnormal continuous epiphysis, coupled with the interposition of a free fat graft, could reliably halt the progression of clinodactyly and allow for spontaneous remodeling in young children. This paradigm shift moved the field away from purely corrective osteotomies in toddlers, emphasizing biological correction and preservation of growth potential.
For established deformities requiring structural correction, the work of Carstam and Eiken (1970) remains the gold standard. They popularized the opening wedge osteotomy, specifically highlighting the biomechanical necessity of the intact dorsal periosteal hinge. Their research demonstrated that reverse wedge osteotomies effectively eliminated clinodactyly with a significantly lower recurrence rate compared to the historically utilized simple closing wedge osteotomies, which often resulted in unacceptable digital shortening.
The modern clinical synthesis of these techniques is best articulated by the age-based treatment algorithm proposed by Strauss and Goldfarb. Their comprehensive reviews and clinical guidelines emphasize that the choice of procedure must be strictly dictated by skeletal maturity. They established the critical threshold of 5 years of age: utilizing the Vickers physiolysis for those under 5 to harness remaining growth, and mandating structural opening wedge osteotomies for those over 5 where growth potential is insufficient for spontaneous correction. Adherence to these established guidelines ensures that orthopedic surgeons can achieve excellent, long-lasting functional and cosmetic outcomes while minimizing the risk of recurrence and iatrogenic complications.
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
