Clubfoot Release: A Masterclass in Posteromedial and Posterolateral Surgical Correction

Key Takeaway
This masterclass guides fellows through posteromedial and posterolateral clubfoot release. We cover comprehensive surgical anatomy, meticulous preoperative planning, and granular intraoperative execution using preferred incisions. Learn to identify and release contracted structures, manage neurovascular risks, and ensure optimal correction. Critical pearls, pitfalls, and postoperative protocols are emphasized to achieve tension-free anatomical alignment and prevent recurrence in resistant cases.
Welcome, colleagues, to the operating theater. Today, we embark on a comprehensive masterclass detailing the surgical management of a resistant, recalcitrant clubfoot, clinically known as talipes equinovarus. This pathology represents far more than a simple cosmetic pedal deformity; it is a profound, three-dimensional structural and kinematic anomaly. If left uncorrected or inadequately addressed, it severely compromises a patient's ambulation, leading to a lifetime of chronic pain, abnormal weight-bearing callosities, debilitating ulcerations, and recurrent deep-space infections.
Our primary objective in the surgical theater is to meticulously release the contracted soft-tissue envelope to achieve a functional, plantigrade, and braceable foot without placing the neurovascular structures or skin under undue tension. The modern orthopedic surgeon must recognize that the true art of clubfoot surgery lies in the philosophy of the "à la carte" release—doing just enough to restore normal osseous alignment, but absolutely no more, thereby preventing the catastrophic sequelae of overcorrection and iatrogenic stiffness.
Comprehensive Introduction and Patho-Epidemiology
Before a scalpel ever touches skin, the orthopedic surgeon must possess a profound, almost intuitive understanding of the underlying pathology. Clubfoot is classically defined by the mnemonic CAVE, representing a rigid positioning of the foot in Cavus (plantarflexion of the forefoot on the hindfoot), Adductus (medial deviation of the forefoot), Varus (inward inversion of the hindfoot), and Equinus (plantarflexion of the ankle and hindfoot). This is not a simple uniplanar bend; it is a complex, multi-planar interplay of severe soft tissue contractures acting upon dysplastic bony malalignments.
Etiology and Embryological Considerations
The exact pathophysiological genesis of idiopathic clubfoot remains a subject of intense academic debate, though it is universally accepted to be multifactorial. A strong genetic predisposition is evident, with a documented familial concordance in a significant percentage of cases. Prevailing theories range from a temporary developmental arrest during the 9th to 10th weeks of fetal embryogenesis to primary germ plasm defects affecting the talar anlage. Other hypotheses implicate in-utero mechanical restriction (oligohydramnios) or subtle vascular anomalies, such as early diminution of the anterior tibial artery, which may precipitate regional neuromuscular imbalance and subsequent fibrosis.

It is of paramount importance to differentiate between an isolated, idiopathic birth defect and a teratologic or syndromic clubfoot. The latter is frequently associated with complex neuromuscular conditions, including myelomeningocele (spina bifida), cerebral palsy, muscular dystrophy, or arthrogryposis multiplex congenita. Identifying these associated syndromic anomalies preoperatively is critical, as they dictate the rigidity of the soft tissues, alter the expected natural history, and significantly reduce the likelihood of success with conservative casting alone. The global incidence of clubfoot hovers around 1 to 2 per 1,000 live births, demonstrating a distinct male predominance (ratio of 2:1) and presenting bilaterally in approximately 50% of all affected infants.
The Natural History of the Untreated Foot
The natural history of an untreated or neglected clubfoot is universally poor, leading to severe functional impairment. As the child grows and begins to bear weight, the mechanical forces of ambulation exacerbate the deformity. The patient is forced to walk on the dorsolateral aspect of the foot, specifically over the cuboid and the base of the fifth metatarsal. This abnormal weight-bearing axis leads to the development of massive, painful adventitial bursae and hyperkeratotic calluses.

Over time, the adaptive bony changes become fixed. The talus deforms into a flattened, wedge shape (the "flat-top talus"), the navicular articulates with the medial malleolus, and the calcaneus becomes rigidly locked in varus and equinus. The surrounding soft tissues undergo severe fibrotic contracture, rendering late surgical intervention exceptionally difficult and significantly increasing the risk of avascular necrosis (AVN) of the talus during extensive capsular releases. Therefore, early recognition and appropriate intervention—whether conservative or surgical—are mandatory to alter this devastating trajectory.
Detailed Surgical Anatomy and Biomechanics
The clubfoot deformity is driven by a complex, synergistic imbalance and contracture of the soft-tissue envelope surrounding the talus, calcaneus, and navicular, fundamentally altering the kinematics of the subtalar and Chopart joints. To perform a successful release, the surgeon must visualize the three-dimensional distortion of these structures prior to dissection.
Osteology and Articular Malalignment
The bony anatomy of a clubfoot is characterized by specific, predictable dysplasias. The talus is the primary culprit; its neck is typically shortened, plantarflexed, and severely medially deviated. This morphological alteration is the keystone of the deformity. The calcaneus is held in rigid varus and equinus, pulled superiorly and medially beneath the talus by the contracted Achilles tendon and posterior capsule, effectively locking the subtalar joint.

The navicular is perhaps the most displaced osseous structure, found medially subluxated or even completely dislocated onto the medial aspect of the talar head. In severe cases, the navicular articulates directly with the medial malleolus. The cuboid follows the navicular, subluxating medially on the anterior process of the calcaneus, contributing to the severe forefoot adduction and supination. Understanding this "medial spin" of the midfoot around the talar head is essential for executing a proper reduction.
Ligamentous and Capsular Contractures
The soft-tissue contractures in a clubfoot are profound and can be topographically divided into medial, posterior, and lateral tethers. Medially, we encounter severe fibrosis and shortening of the talonavicular capsule, the calcaneonavicular (spring) ligament, and the robust deltoid ligament (particularly its deep tibiotalar components). The superficial deltoid and the tibionavicular ligaments tether the navicular to the medial malleolus.
Posteriorly, the pathology is driven by the contracted posterior ankle capsule (tibiotalar capsule) and the posterior subtalar capsule (talocalcaneal capsule). The posterior talofibular ligament and the calcaneofibular ligament are also frequently shortened, locking the calcaneus in equinus. The interosseous talocalcaneal ligament, located deep within the sinus tarsi, is often thickened and acts as a major impediment to the lateral rotation and valgus reduction of the calcaneus.
Musculotendinous and Neurovascular Considerations
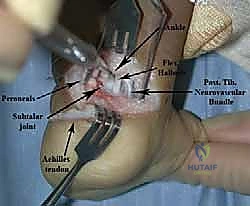
The musculotendinous units crossing the ankle and subtalar joints are severely imbalanced. The Achilles tendon (tendo calcaneus) is universally thick, tight, and contracted, representing the primary deforming force for hindfoot equinus. Other critically contracted tendons include the tibialis posterior (the primary invertor of the midfoot), the flexor digitorum longus (FDL), and the flexor hallucis longus (FHL). The calf musculature, particularly the triceps surae, exhibits congenital hypoplasia and atrophy, a finding that persists even after successful correction.

Neurovascular anatomy is the most critical safety consideration during this procedure. As we dissect medially, we must be exquisitely aware of the posteromedial neurovascular bundle (posterior tibial artery, posterior tibial veins, and the tibial nerve), which courses together with the FHL and FDL in the tarsal tunnel, just posterior and inferior to the medial malleolus. The sural nerve and lesser saphenous vein are highly vulnerable laterally, particularly during the lateral limb of the Cincinnati incision. Meticulous hemostasis, blunt dissection techniques, and loupe magnification are mandatory to protect these vital structures from iatrogenic transection or traction injury.
Exhaustive Indications and Contraindications
It is a fundamental tenet of modern pediatric orthopedics that extensive, comprehensive surgical releases are required in fewer than 5% of all idiopathic clubfoot cases today. The Ponseti method of serial manipulation and casting remains the undisputed gold standard for initial treatment, successfully achieving correction in upwards of 90-95% of compliant patients. Surgery is reserved for specific, recalcitrant scenarios.
Defining Surgical Candidacy
The primary indication for a comprehensive posteromedial and posterolateral release is a rigid, resistant clubfoot that has failed an adequate, meticulously applied trial of Ponseti casting. This is often seen in "atypical" or "complex" clubfeet, which present with a short, stubby foot, a deep transverse plantar crease, and severe equinus. Furthermore, teratologic clubfeet—those associated with underlying neuromuscular disorders such as arthrogryposis or myelomeningocele—are notoriously resistant to conservative measures and frequently require early, extensive surgical intervention.

Timing is a critical variable. Soft tissue releases are typically most effective when performed between the ages of 6 months and 2 years. In this window, the cartilaginous anlagen of the tarsal bones are still malleable enough to remodel congruently once the deforming soft-tissue forces are released. Operating too early (under 3-4 months) increases the risk of anesthetic complications and technical difficulty due to the diminutive size of the structures. Operating too late (beyond 4-5 years) often yields suboptimal results, as the bony deformities become fixed, necessitating complex osseous procedures (e.g., lateral column shortening, medial column lengthening, or corrective osteotomies) in addition to soft tissue release.
Clinical Decision-Making Matrix
| Indication Category | Specific Clinical Scenarios | Surgical Approach/Recommendation |
|---|---|---|
| Primary Idiopathic (Failed Conservative) | Failure to achieve plantigrade foot after 6-8 Ponseti casts; persistent rigid equinovarus. | Comprehensive Posteromedial/Posterolateral Release (Cincinnati or Turco). |
| Teratologic/Syndromic | Arthrogryposis, Spina Bifida, Diastrophic Dysplasia presenting with rigid, unyielding deformity. | Early, extensive soft tissue release; high likelihood of requiring concurrent tendon transfers or talectomy in severe cases. |
| Recurrent Deformity (Toddler) | Relapse of supination/varus due to bracing non-compliance after initial Ponseti success. | Limited release (e.g., Tibialis Anterior Tendon Transfer - TATT) combined with Achilles lengthening. Avoid full posteromedial release if possible. |
| Contraindications | Active local infection; medically unstable infant; previously overcorrected foot (valgus/pronated). | Absolute contraindication. Delay surgery until medically optimized or infection resolves. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for a comprehensive clubfoot release is a meticulous, multi-faceted process that synthesizes a rigorous clinical examination with targeted radiographic evaluation. The goal is to map out the exact sequence of releases required, adhering to the "à la carte" philosophy.
Advanced Clinical Assessment
Our examination begins with a standardized assessment of the deformity, often utilizing validated scoring systems such as the Pirani or Dimeglio scores. We systematically evaluate the severity of the hindfoot equinus, hindfoot varus, midfoot supination, and forefoot adductus.

Palpation is critical. The surgeon must palpate the dorsolateral aspect of the midfoot to locate the prominent talar head, which remains uncovered due to the medial subluxation of the navicular. When assessing range of motion, particularly equinus, a common clinical pitfall must be avoided: the surgeon must palpate the os calcis directly. The thick infantile heel pad may superficially appear to dorsiflex, creating a "rocker-bottom" illusion, while the calcaneus itself remains rigidly locked in equinus.

We must also assess the reducibility of the forefoot onto the talar head. The more rigid the talonavicular articulation, the more extensive the medial release required. Furthermore, the resting alignment of the heel relative to the tibia in the sagittal and coronal planes must be documented. The ultimate intraoperative goal is to achieve 5 to 10 degrees of valgus; failure to achieve this indicates an incomplete release of the subtalar tethers.
Radiographic and Imaging Protocols
While plain radiography offers limited utility in the newborn due to the lack of ossification centers (the navicular, for instance, does not ossify until 3-4 years of age), it becomes an indispensable tool in older infants and toddlers. We routinely obtain weight-bearing (or simulated weight-bearing using a radiolucent block) anteroposterior (AP) and lateral radiographs of the foot and ankle.
On the AP view, we assess the Kite's angle (the talocalcaneal angle). In a normal foot, this angle ranges from 20 to 40 degrees. In a clubfoot, the axes of the talus and calcaneus are nearly parallel, resulting in an angle approaching zero. We also evaluate the talar-1st metatarsal angle to quantify forefoot adductus. On the lateral view, the lateral talocalcaneal angle is measured; again, parallelism indicates persistent hindfoot varus and equinus. These baseline metrics are crucial for intraoperative comparison.
Patient Positioning and Surgical Setup
Optimal patient positioning is the foundation of a smooth surgical procedure. For a comprehensive posteromedial and posterolateral release utilizing the Cincinnati approach, the patient is placed in the prone position.

Adequate padding is placed beneath the chest and iliac crests to ensure unrestricted ventilation and prevent pressure necrosis. The bilateral lower extremities are prepped and draped free, allowing the knee to be fully extended or flexed to 90 degrees as needed. Flexing the knee to 90 degrees during the procedure relaxes the gastrocnemius complex, dramatically facilitating the visualization and subsequent Z-lengthening of the Achilles tendon. A well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, which is absolutely critical for the safe identification of the delicate neurovascular structures. Finally, the fluoroscopic C-arm is positioned to allow for seamless, orthogonal intraoperative imaging without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be methodical, precise, and respectful of the soft tissues. We will utilize the Cincinnati incision, a transverse, circumferential approach that provides unparalleled, panoramic access to the medial, posterior, and lateral compartments of the clubfoot.
The Cincinnati Incision and Superficial Dissection
The incision begins medially at the level of the first metatarso-cuneiform joint. It extends proximally and posteriorly, running parallel to the sole of the foot, crossing the posterior aspect of the ankle at the level of the tibiotalar joint crease, and terminating laterally at the calcaneocuboid joint.

The initial dissection is carried down through the subcutaneous tissue. Extreme caution must be exercised on the lateral aspect of the incision to identify and protect the sural nerve and the lesser saphenous vein, which are mobilized and retracted superiorly. Medially, the skin flaps are elevated to expose the deep fascia. The key to preventing postoperative skin slough is to maintain thick, full-thickness fasciocutaneous flaps; avoiding aggressive subcutaneous undermining is paramount.
The Medial Release: Unlocking the Midfoot
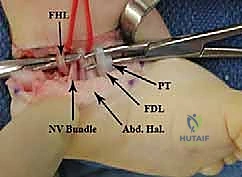
The medial dissection begins with the identification of the posteromedial neurovascular bundle. The deep fascia (flexor retinaculum) is incised, and the tibial nerve and posterior tibial artery are carefully isolated with a vessel loop and gently retracted.

Next, we identify the tendons of the medial compartment. The tibialis posterior tendon is traced distally to its broad insertion on the navicular and medial cuneiform. In severe cases, a Z-lengthening of the tibialis posterior is performed. We then identify the Master Knot of Henry, where the FDL crosses over the FHL. Releasing the fascial sling at this junction allows the FHL and FDL to glide freely, reducing the medial tethering.

The crux of the medial release is the complete capsulotomy of the talonavicular joint. The capsule is incised dorsally, medially, and plantarly, taking care not to score the articular cartilage of the talar head. The spring ligament (calcaneonavicular ligament) is divided. Once this release is complete, the navicular should glide laterally, reducing concentrically onto the talar head.

The Posterior Release: Correcting the Equinus
Attention is then directed posteriorly. The Achilles tendon is identified and isolated. A formal Z-lengthening is performed in the sagittal plane. The distal cut is typically made medially to remove the inversion vector of the tendon, while the proximal cut is made laterally. The tendon ends are tagged and reflected.

With the Achilles out of the way, the posterior capsule of the ankle (tibiotalar joint) and the posterior capsule of the subtalar joint (talocalcaneal joint) are exposed. A meticulous posterior capsulotomy is performed across both joints. The posterior talofibular ligament and the calcaneofibular ligament are divided. This extensive posterior release is the definitive step required to allow the calcaneus to dorsiflex out of equinus and rotate laterally out of varus.
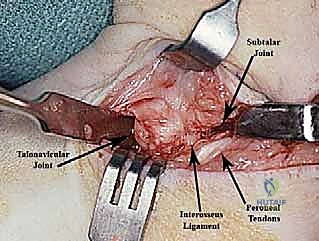
The Lateral Release and Osseous Fixation
If the calcaneus remains locked in varus despite the posterior release, the dissection proceeds laterally. The lateral subtalar capsule is incised. In extremely rigid cases, the interosseous talocalcaneal ligament within the sinus tarsi may need to be carefully sectioned, though this should be done sparingly to avoid destabilizing the subtalar joint.
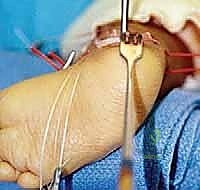
Once all soft tissue tethers have been released, the foot is gently manipulated into a corrected, plantigrade position. The navicular is reduced onto the talar head, and the calcaneus is positioned in slight valgus and dorsiflexion. To maintain this reduction during the healing phase, Kirschner wires (K-wires) are utilized. A smooth K-wire (typically 0.045 or 0.062 inches) is driven retrogradely from the dorsum of the first metatarsal, through the medial cuneiform and navicular, and into the center of the talar head.
A second K-wire may be placed across the calcaneocuboid joint or up through the heel across the subtalar joint to maintain the hindfoot correction. Intraoperative fluoroscopy is mandatory at this stage to confirm absolute concentric reduction of the talonavicular joint and restoration of the talocalcaneal angles.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, comprehensive clubfoot releases carry a significant risk profile. The orthopedic surgeon must be intimately familiar with potential complications, their incidence, and the appropriate salvage strategies. The overarching principle is that it is far better to accept a mild, asymptomatic undercorrection than to create a stiff, painful, overcorrected foot.
Early Postoperative Complications
The most dreaded early complication is wound dehiscence and skin necrosis, particularly at the apex of the Cincinnati incision or the posterior aspect of a Turco incision. This occurs due to excessive tension on the skin edges when the foot is dorsiflexed and abducted into the corrected position. If blanching is observed during closure, the foot must be casted in slight equinus to relieve tension, with gradual correction achieved through serial cast changes in the outpatient clinic.

Neurovascular injury is rare but catastrophic. Transection of the posterior tibial artery can lead to partial foot ischemia, although the robust collateral circulation from the dorsalis pedis usually prevents frank gangrene. Injury to the tibial nerve results in devastating plantar anesthesia and intrinsic muscle paralysis. Immediate microsurgical repair is mandated if transection is identified intraoperatively.
Late Complications and Deformities
Late complications are frequently related to the biomechanical consequences of the surgical release. Avascular necrosis (AVN) of the talus is a severe complication resulting from aggressive dissection stripping the fragile blood supply surrounding the talar neck and sinus tarsi. AVN leads to talar collapse, chronic pain, and rigid osteoarthritis, often necessitating salvage arthrodesis later in life.

Overcorrection is a hallmark of overly aggressive surgery. Excessive lateral release can lead to a severe, painful calcaneovalgus deformity or a planovalgus foot. Over-lengthening of the Achilles tendon, combined with a strong, unopposed tibialis anterior, frequently results in a "dorsal bunion"—a fixed dorsiflexion deformity of the first metatarsal with compensatory plantarflexion of the great toe.
| Complication | Estimated Incidence | Etiology / Risk Factor | Salvage / Management Strategy |
| :
