Intertrochanteric Varus Osteotomy: A Masterclass in Femoral Reorientation

Key Takeaway
This masterclass provides an exhaustive, real-time guide to intertrochanteric varus osteotomy. Fellows will learn intricate surgical anatomy, meticulous preoperative planning, and granular intraoperative execution from incision to hardware placement. We cover essential pearls, potential pitfalls, and comprehensive postoperative management, ensuring a deep understanding of femoral reorientation to improve hip joint congruency and prevent progressive destruction.
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues and fellows, to the operating theater and to this definitive exploration of proximal femoral reconstruction. Today, we are undertaking an intricate, highly demanding, and profoundly rewarding procedure: the intertrochanteric adduction (varus) osteotomy of the proximal femur. This intervention transcends the simplistic definition of a mere bone cut; it is a masterclass in spatial reorientation designed to fundamentally alter the biomechanical environment of the hip joint. By meticulously calculating and executing a change in the proximal femoral geometry, we aim to improve femoral head coverage, restore articular congruency, and optimize the transmission of forces across the hip joint. Our ultimate, overarching goal is the alleviation of debilitating pain, the preservation of the native hip joint, and the significant delay—if not outright prevention—of the need for total hip arthroplasty (THA) in a carefully selected patient demographic.
The historical context of this procedure is deeply rooted in the pioneering biomechanical principles elucidated by Friedrich Pauwels and later refined by figures such as Bombelli and Müller. They recognized that hip joint incongruence invariably leads to an increased mechanical load concentrated on a dramatically reduced weight-bearing surface area. According to Wolff’s Law, this focal stress concentration initiates a predictable, deleterious cascade of subchondral sclerosis, cyst formation, cartilage degradation, and ultimately, end-stage arthrotic changes. By performing a varus osteotomy, we effectively medialize the mechanical axis of the lower extremity relative to the hip joint center, lateralize the greater trochanter to enhance the abductor lever arm, and rotate the femoral head to bring a healthier, more congruent segment of articular cartilage into the primary weight-bearing dome of the acetabulum.
The patho-epidemiology of conditions amenable to this intervention centers on structural deformities that compromise the normal ball-and-socket kinematics. We are primarily evaluating young, active patients whose native joints possess sufficient viable cartilage to warrant preservation. The quintessential candidate presents with a structural mismatch that, if left untreated, guarantees premature joint failure. The absolute prerequisite for a successful clinical outcome is the radiographic and clinical confirmation that the joint incongruence can be significantly ameliorated by spatial reorientation. If the joint is perfectly spherical but completely denuded of cartilage, an osteotomy will fail. The joint must demonstrate "hinge" abduction or focal incongruity that improves dynamically when the femur is placed in a varus, and often slightly extended or internally rotated, position.
While the modern era of orthopedics frequently defaults to total hip arthroplasty due to its excellent, predictable results even in younger cohorts, the paradigm of joint preservation remains crucial. Arthroplasty in a twenty-year-old guarantees multiple future revision surgeries, each carrying escalating risks of bone loss, infection, and mechanical failure. Therefore, the intertrochanteric osteotomy remains an indispensable tool in the armamentarium of the comprehensive hip surgeon. Furthermore, the operative techniques discussed herein, with appropriate preoperative mathematical modifications, can be seamlessly adapted for corrections in abduction (valgus), flexion, extension, and axial rotation, or any complex multiplanar combination thereof, highlighting the profound versatility of this surgical approach.

Detailed Surgical Anatomy and Biomechanics
To execute an intertrochanteric osteotomy with precision and safety, an exhaustive understanding of the tridimensional anatomy and local biomechanics of the hip joint is non-negotiable. The hip is a robust, multiaxial ball-and-socket synovial joint, engineered by evolution to transmit dynamic, multi-vectorial loads from the axial skeleton to the lower extremities while maintaining a broad arc of motion.
Osteology and Articular Surfaces
The proximal femoral architecture is a marvel of biological engineering, characterized by intersecting trabecular patterns that reflect the principal compressive and tensile stresses acting upon the bone. The femoral head is predominantly covered with smooth, hyaline articular cartilage, with the notable exception of the fovea capitis. The fovea serves as the attachment footprint for the ligamentum teres and its accompanying artery. In pathologic states, such as a severe valgus deformity (coxa valga), the fovea—a non-articular, mechanically inferior structure—can be rotated directly into the critical superior weight-bearing zone, leading to abnormal contact pressures and rapid focal degeneration.
The acetabulum is a hemispherical cavity whose depth and stability are significantly augmented by the fibrocartilaginous labrum. Physiologically, more than half of the femoral head is captured within this socket. The articular surface of the acetabulum is restricted to the lunate surface, while the central and inferior portion, the acetabular fossa, contains the pulvinar fat pad and is non-weight-bearing. Our primary geometric objective with a varus osteotomy is to rotate the femoral head to maximize the contact area between the healthy hyaline cartilage of the head and the lunate surface of the acetabulum, particularly improving lateral coverage. This effectively increases the weight-bearing surface area, thereby decreasing peak contact pressures according to the fundamental equation of Pressure = Force / Area.
Our surgical theater is specifically the intertrochanteric region, the transitional zone between the femoral neck and the diaphysis, bounded by the greater and lesser trochanters. The greater trochanter is our primary palpable anatomical landmark for the surgical incision and serves as the critical insertion point for the abductor complex (gluteus medius and minimus). The lesser trochanter, situated posteromedially, serves as the insertion for the powerful iliopsoas tendon. Intraoperatively, the cranial border of the lesser trochanter is an indispensable internal reference point for determining the distal extent of our osteotomy cut, ensuring we remain in highly vascular, rapidly healing cancellous bone rather than the dense cortical bone of the subtrochanteric diaphysis.

Neurovascular Relationships
The proximal femur is enveloped in a rich, complex neurovascular network. Meticulous dissection, precise retractor placement, and an acute awareness of these structures are paramount to prevent catastrophic iatrogenic complications.
The paramount concern is the blood supply to the femoral head. The dominant arterial supply is derived from the medial circumflex femoral artery (MCFA), a major branch of the deep femoral artery (profunda femoris). The MCFA courses posteriorly around the base of the femoral neck, giving rise to the critical posterosuperior and posteroinferior retinacular vessels. These vessels ascend along the femoral neck beneath the synovial reflection to perfuse the capital epiphysis. Any inadvertent damage to these vessels—whether through errant osteotome placement, excessive posterior soft tissue stripping, or aggressive retractor placement—can precipitate devastating avascular necrosis (AVN) of the femoral head, entirely defeating the purpose of a joint-preserving operation.
The lateral circumflex femoral artery (LCFA) courses anteriorly. While its ascending branch contributes to the extracapsular arterial ring, the MCFA remains the dominant intraosseous supplier. During our lateral approach, as we reflect the vastus lateralis, we will invariably encounter the first perforating arteries. These vessels, often branches of the LCFA or directly from the deep femoral artery, typically cross the operative field 8 to 10 centimeters distal to the innominate tubercle. They must be meticulously identified, isolated, and ligated or cauterized; failure to do so will result in profound, vision-obscuring hemorrhage that complicates the osteotomy execution.
Regarding neurology, the lateral approach necessitates strict vigilance concerning the superior gluteal nerve. This nerve exits the greater sciatic foramen above the piriformis and courses between the gluteus medius and minimus, innervating both, before terminating in the tensor fasciae latae (TFL). When splitting the gluteus medius or retracting the TFL anteriorly, the surgeon must diligently protect the terminal branches supplying the TFL. The "safe zone" is typically cited as being no more than 3 to 5 centimeters cranial to the tip of the greater trochanter. Iatrogenic denervation here leads to profound abductor weakness, a persistent Trendelenburg limp, and significant gait pathology.
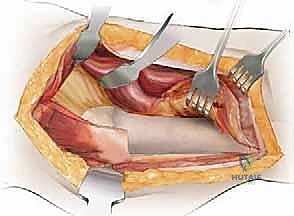
Muscular Intervals and Biomechanics of Reorientation
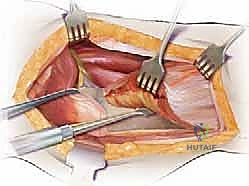
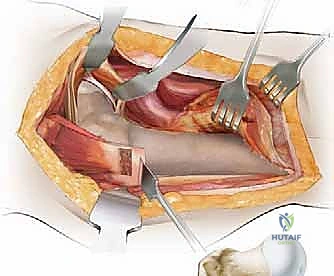
Our standard lateral approach (a modification of the Hardinge or Watson-Jones intervals) navigates the precise fascial planes between major muscle groups. We typically perform an L-shaped or straight distal detachment of the vastus lateralis from its origin on the vastus ridge of the greater trochanter and the proximal linea aspera. This reflection creates a safe, avascular interval medial to the abductor musculature, allowing wide exposure of the lateral femoral cortex for hardware application.
The tensor fasciae latae lies anterior to the gluteus medius. Incision placement is critical: a trajectory that is too anterior risks severing the TFL muscle belly, while a trajectory that is excessively posterior risks erroneous division of the cranial fibers of the gluteus maximus, leading to unnecessary bleeding and dead space.
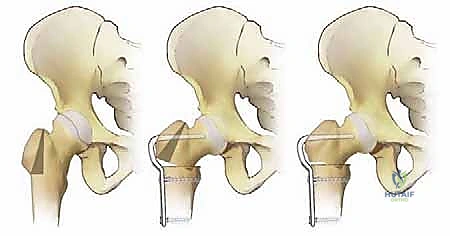
Biomechanically, the varus osteotomy directly manipulates Pauwels' classification of hip forces. By resecting a medial-based wedge and closing the osteotomy, we decrease the neck-shaft angle (varization). This medializes the femoral shaft relative to the center of rotation of the femoral head. Concurrently, it lateralizes the greater trochanter. This lateralization significantly increases the moment arm of the abductor musculature. Consequently, the abductors require less force to maintain pelvic horizontality during the single-leg stance phase of gait. This reduction in required abductor force directly translates to a profound decrease in the resultant joint reaction force (R) across the articular surface, fulfilling the primary biomechanical objective of the procedure.
Exhaustive Indications and Contraindications
The success of an intertrochanteric varus osteotomy is entirely predicated on rigorous, uncompromising patient selection. The procedure is technically demanding and requires a compliant patient capable of adhering to strict postoperative rehabilitation protocols. The ideal candidate is a physiologically young, non-obese patient with a symptomatic, mechanically incongruent hip joint that demonstrates preserved cartilage space on functional radiographs.
We are specifically targeting pathologies where hip joint incongruence leads to an increased load on a reduced weight-bearing area. Mild epiphyseal dysplasia of the femoral head is a classic indication, particularly when the lateral aspect of the head remains intact, viable, and spherical enough to be rotated into the weight-bearing dome. Similarly, patients with developmental dysplasia of the hip (DDH) frequently benefit from this procedure. In the context of DDH, a varus-derotation osteotomy (VDRO) is often performed concomitantly with a periacetabular osteotomy (PAO) to achieve optimal, tridimensional joint congruency and stability.
Other indications include circumscribed anteromedial avascular necrosis (AVN) or osteochondritis dissecans of the femoral head. In these scenarios, the osteotomy is utilized to mechanically offload the necrotic or fragmented segment, rotating it away from the peak stress zones and bringing healthy posterior or lateral cartilage into the zenith of the acetabulum. This offloading can halt the progression of collapse and promote creeping substitution and healing. Furthermore, a valgus femoral head (often seen in neuromuscular conditions or as a sequela of childhood hip disease) responds exceptionally well to varization, restoring normal abductor mechanics and centralizing the femoral head. Posttraumatic joint incongruence, such as malunions of femoral neck fractures or slipped capital femoral epiphysis (SCFE) sequelae, can also be addressed, provided the articular cartilage remains viable.
Conversely, the contraindications must be strictly respected. Advanced osteoarthritis (Tönnis Grade 3 or 4), characterized by complete loss of joint space, large subchondral cysts, and severe osteophytosis, is an absolute contraindication. In such cases, there is no viable cartilage to preserve, and an osteotomy will only subject the patient to unnecessary surgical morbidity before an inevitable THA. Inflammatory arthropathies (e.g., Rheumatoid Arthritis, Ankylosing Spondylitis) are generally contraindicated due to the systemic, progressive nature of the cartilage destruction. Finally, severe preoperative joint stiffness is a harbinger of poor outcomes; an osteotomy requires a functional preoperative arc of motion to allow the reoriented head to articulate smoothly within the acetabulum.
| Category | Specific Conditions | Rationale / Clinical Notes |
|---|---|---|
| Primary Indications | Mild Epiphyseal Dysplasia | Preserves viable lateral cartilage by rotating it into the weight-bearing zone. |
| Developmental Dysplasia of the Hip (DDH) | Often combined with pelvic osteotomy to optimize global joint congruency. | |
| Focal Avascular Necrosis (Kerboul angle < 200°) | Offloads the necrotic segment to prevent subchondral collapse. | |
| Coxa Valga / Subluxation | Restores the neck-shaft angle, improves abductor lever arm, centralizes head. | |
| Sequelae of Perthes or SCFE | Corrects complex multiplanar deformities (varus/flexion/derotation). | |
| Absolute Contraindications | Advanced Osteoarthritis (Tönnis Grade 3/4) | Lack of viable hyaline cartilage makes preservation futile; THA is indicated. |
| Inflammatory Arthropathy (RA, AS) | Progressive systemic cartilage destruction will outpace any biomechanical benefit. | |
| Severe Joint Stiffness (< 60° flexion arc) | Reoriented head requires mobility to function; stiffness leads to rapid failure. | |
| Active Joint Infection | Absolute contraindication for internal fixation and major reconstructive surgery. | |
| Relative Contraindications | Advanced Age (> 50-55 years) | Lower regenerative capacity; THA offers faster, more reliable return to function. |
| Severe Obesity (BMI > 35) | Exponentially increases risk of hardware failure, nonunion, and complications. |



Pre-Operative Planning, Templating, and Patient Positioning
Gentlemen, it is an axiom of orthopedic surgery that the battle is won or lost before the first incision is ever made. In the context of an intertrochanteric osteotomy, preoperative planning is not merely a suggestion; it is a mandatory, exhaustive process. The precise calculation of angles, wedge sizes, and hardware placement dictates the entire biomechanical outcome of the procedure.
Imaging and Diagnostic Studies
A comprehensive, high-quality radiographic workup is the foundation of our planning. We begin with a standard anteroposterior (AP) radiograph of the entire pelvis. Crucially, the patient's lower extremities must be positioned in 15 degrees of internal rotation. This maneuver compensates for normal femoral antetorsion, bringing the femoral neck parallel to the imaging cassette and providing a true AP projection of the neck-shaft angle and lateral head coverage.
Functional radiographs are indispensable. An AP radiograph of the pelvis with the affected hip in maximal abduction is critical. This dynamic view simulates the postoperative position of the femoral head following a varus osteotomy. It allows the surgeon to visually confirm whether varization actually improves joint congruency and helps estimate the optimal degree of angular correction required. If maximal abduction results in hinge-like opening of the medial joint space rather than concentric seating, a pure varus osteotomy may be contraindicated, or a concomitant pelvic procedure may be required.
We also mandate a false-profile view (the Lequesne view), which provides a true lateral projection of the anterior femoral head and anterior acetabular coverage, essential for evaluating anterior dysplasia. An axial view (cross-table lateral or Dunn view) is required to assess the sphericity of the head and the extent of any cam-type morphology or anterior/posterior necrosis. Advanced imaging, specifically a high-resolution MRI or a CT arthrogram, is highly recommended. These modalities offer unparalleled visualization of the articular cartilage integrity, labral pathology, and the precise tridimensional volume of any avascular necrosis, confirming that sufficient viable cartilage exists to justify the preservation attempt.

Detailed Preoperative Drawing and Digital Templating
The templating process is where surgical art meets geometric science. Whether utilizing traditional acetate overlays on physical radiographs or advanced digital templating software within a PACS environment, the steps remain rigorous.
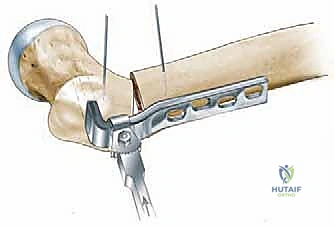
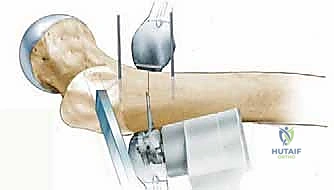
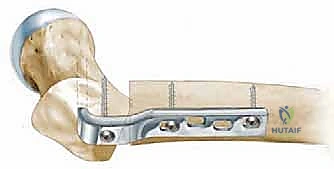
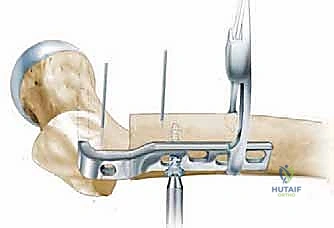
First, the precise outlines of the proximal femur and the acetabulum are traced. We then identify our critical reference points. The innominate tubercle (IT) on the greater trochanter is our primary lateral, intraoperatively palpable landmark. We must also identify the dense primary compressive bone trabeculae within the femoral neck and head; this is the optimal trajectory for our seating chisel and subsequent blade plate, ensuring maximum mechanical purchase in the cancellous bone.
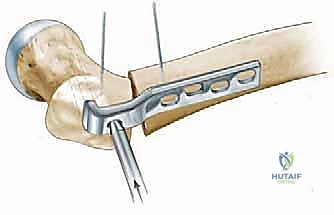
The planned osteotomy line is drawn perpendicular to the mechanical axis of the femoral shaft, typically aiming for the cranial extension of the lesser trochanter to ensure we remain in the highly vascular intertrochanteric cancellous bed. Based on the functional abduction radiographs, we determine the desired correction angle (e.g., 20 degrees of varus). We then template the blade position relative to the planned osteotomy line to achieve this exact correction. The intersection of this templated blade trajectory with the lateral femoral cortex dictates the precise entry point for the seating chisel.
Crucially, we must measure the distance from this calculated entry point to the innominate tubercle. This measurement is the key to reproducing the templated plan intraoperatively. Furthermore, if the planned varus correction angle exceeds 25 degrees, a concomitant greater trochanteric osteotomy is strongly recommended. Massive varization without trochanteric advancement leads to severe relative overgrowth of the greater trochanter, resulting in extra-articular impingement against the ilium and profound abductor weakness due to a shortened resting length. If templated, the trochanteric fragment must be at least 10 mm thick to allow for robust reattachment. Finally, all linear measurements must be corrected for radiographic magnification, typically reducing measured distances by 10-15% depending on the specific calibration marker used during the imaging process.

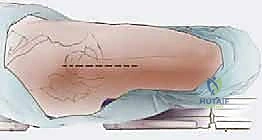
Patient Positioning and Operating Room Setup
Proper patient positioning is critical to facilitate both surgical exposure and unimpeded fluoroscopic imaging. The patient is typically placed sup
Clinical & Radiographic Imaging Archive