Comprehensive Management of Severe Intrinsic Contractures and Dupuytren Disease

Key Takeaway
Severe intrinsic contractures of the hand, often secondary to compartment syndrome, Volkmann ischemic contracture, or progressive Dupuytren disease, present profound reconstructive challenges. Successful management requires a meticulous understanding of hand biomechanics, precise surgical release of fibrotic muscle tissue, and advanced soft-tissue coverage techniques, such as cross-arm flaps for web space deepening. This guide details the indications, operative steps, and postoperative protocols for restoring optimal hand function.
Comprehensive Introduction and Patho-Epidemiology
Severe intrinsic contractures of the hand and Dupuytren disease represent two of the most formidable reconstructive challenges encountered by the orthopedic hand surgeon. While their precipitating etiologies diverge significantly—one rooted in acute ischemic trauma and the other in a progressive, genetically driven fibroproliferative disorder—both culminate in a shared pathological endpoint: the devastating replacement of compliant, functional myofascial architecture with rigid, inelastic fibrous tissue. This profound structural derangement dismantles the intricate biomechanical cascade of the hand, resulting in fixed flexion deformities, obliteration of functional web spaces, and severe global disability.
Pathogenesis of Ischemic Muscle Fibrosis
Volkmann ischemic contracture is the catastrophic end-stage sequela of an untreated, delayed, or inadequately decompressed acute compartment syndrome. The pathophysiological cascade is initiated by a critical elevation in interstitial tissue pressure within the unyielding osseofascial compartments of the forearm and hand. This pressure surpasses the capillary perfusion pressure, leading to an abrupt cessation of microvascular blood flow. The ensuing hypoxia triggers a shift to anaerobic metabolism, rapidly depleting intracellular adenosine triphosphate (ATP) stores. The failure of ATP-dependent sodium-potassium pumps results in massive intracellular edema, further exacerbating the intracompartmental pressure in a devastating positive feedback loop.
If surgical decompression via fasciotomy is not performed within the critical ischemic window (typically 4 to 6 hours), irreversible myonecrosis ensues. The necrotic muscle fibers elicit a profound macrophage-mediated inflammatory response. The body’s attempt at repair leads to the hyperproliferation of fibroblasts, which synthesize dense, disorganized Type I and Type III collagen. Over months, this immature scar tissue undergoes cross-linking and maturation, contracting relentlessly. The resulting fibrotic cord tethers the deep flexors (flexor digitorum profundus and flexor pollicis longus) and the intrinsic musculature, drawing the wrist and digits into the pathognomonic Volkmann posture.
The Dupuytren Diathesis and Fibroproliferative Cascade
In stark contrast to the ischemic etiology of Volkmann contracture, Dupuytren disease is an insidious, progressive fibroplasia of the palmar aponeurosis. The fundamental pathological unit is the myofibroblast—a specialized cell exhibiting characteristics of both fibroblasts and smooth muscle cells. Driven by complex genetic predispositions and aberrant cellular signaling pathways (notably the Wnt/β-catenin and Transforming Growth Factor-beta [TGF-β] pathways), normal fascial bands undergo pathological hypertrophy.
The disease is not merely a localized phenomenon but rather a systemic manifestation of a fibroproliferative disorder. Patients exhibiting ectopic deposits of Dupuytren-like fibroplasia are classified as having a "Dupuytren diathesis." This diathesis indicates a highly aggressive, genetically penetrant form of the disease, characterized by early onset, rapid progression, and an exceptionally high rate of postoperative recurrence. Clinical manifestations of the diathesis include Ledderhose disease (plantar fibromatosis), Peyronie disease (penile fibromatosis), and Garrod nodules (dorsal knuckle pads).
Epidemiological Considerations
The epidemiological profile of Dupuytren disease is striking. It is predominantly a disease of middle-aged to elderly adults, with the highest incidence observed in individuals of Northern European, Scandinavian, and Celtic descent, earning it the historical moniker "Viking disease." The disease exhibits a profound sex predilection, occurring up to ten times more frequently in men than in women. Furthermore, the onset in men is typically a decade earlier and follows a more aggressive clinical course.
Systemic comorbidities heavily influence the incidence and severity of Dupuytren disease. There is a well-documented correlation with diabetes mellitus; however, diabetic patients often present with a milder, more diffuse form of the disease that frequently spares the metacarpophalangeal (MCP) joints and primarily affects the middle and ring fingers. Epilepsy, particularly in patients managed with long-term barbiturate therapy, is also associated with a significantly increased prevalence. While the relationship between manual labor, repetitive microtrauma, and the onset of Dupuytren disease remains a subject of intense academic debate, histological evidence of hemosiderin deposits within the nodules suggests that micro-hemorrhages from fascial micro-tears may act as a precipitating catalyst in genetically susceptible individuals.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the complex, three-dimensional surgical anatomy of the hand is the bedrock of successful reconstructive intervention. The surgeon must navigate an intricate labyrinth of neurovascular bundles, tendinous insertions, and fascial septa, all of which are grossly distorted by the underlying fibrotic pathology.
The Intrinsic Musculature and the Ischemic Cascade
The intrinsic muscles of the hand—comprising the interossei, lumbricals, thenar, and hypothenar eminences—are uniquely vulnerable to ischemic insult due to their tight fascial envelopes. When acute compartment syndrome affects the hand, the interossei and the adductor pollicis are most frequently devastated. The normal biomechanical role of the intrinsic muscles is to flex the MCP joints and extend the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints.
When these muscles undergo ischemic necrosis and subsequent fibrotic contracture, they produce an exaggerated "intrinsic-plus" posture: severe MCP flexion coupled with PIP and DIP extension. Conversely, if the deep volar compartment of the forearm (containing the extrinsic flexors) is the primary site of infarction, the overriding extrinsic fibrotic pull results in an "intrinsic-minus" or claw hand deformity, characterized by MCP hyperextension and IP flexion. In the most severe manifestations of Volkmann contracture, combined intrinsic and extrinsic fibrosis creates a rigid, functionless appendage requiring massive reconstructive efforts.
Normal Palmar Fascia versus Pathological Cords
In Dupuytren disease, the surgeon must intimately understand the distinction between normal anatomical bands and pathological cords. The normal palmar fascia consists of pretendinous bands, the superficial transverse palmar ligament, natatory ligaments, and complex vertical septa (the ligaments of Legueu and Juvara). As the disease progresses, these compliant bands hypertrophy and contract to form predictable, unyielding cords.
The pretendinous cord arises from the pretendinous band and is the primary driver of MCP joint flexion contractures. As the disease extends distally into the digit, the central cord develops, causing progressive PIP joint flexion. The natatory cord, arising from the natatory ligaments, obliterates the web spaces, restricting digital abduction.
Biomechanics of the Spiral Cord and Neurovascular Displacement
The most treacherous anatomical distortion in Dupuytren surgery is the formation of the spiral cord. This pathological structure originates from four distinct normal anatomical entities: the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament. As the spiral cord contracts, it creates a biomechanical bowstring effect that profoundly alters the trajectory of the digital neurovascular bundle.
Normally, the neurovascular bundle lies deep and protected. However, the contracting spiral cord displaces the bundle in three distinct vectors: centrally (toward the midline of the digit), superficially (immediately deep to the dermis), and proximally. This displacement places the digital nerve and artery at immense risk of iatrogenic transection during surgical dissection. The fundamental tenet of Dupuytren surgery is to identify the neurovascular bundle in virgin, unscarred tissue proximally in the palm, and meticulously trace it distally, releasing the constricting spiral cord under direct, magnified vision.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention requires a nuanced risk-benefit analysis, balancing the severity of the functional deficit against the inherent risks of complex reconstructive surgery, prolonged rehabilitation, and the potential for disease recurrence or postoperative flare reactions.
Clinical Thresholds for Intervention
For Volkmann ischemic contracture, surgical intervention is indicated when conservative measures (such as serial casting and dynamic splinting) have failed to halt progression, or when the patient presents with an established, rigid deformity that precludes functional grasp and pinch. The obliteration of the first web space due to adductor pollicis fibrosis is an absolute indication for radical release and flap reconstruction, as a functional thumb is paramount to global hand utility.
In Dupuytren disease, the classic indication for surgery is a positive Hueston tabletop test (the inability to place the palm flat on a hard surface). Specifically, an MCP joint contracture exceeding 30 degrees warrants intervention. Because the MCP joint capsule is highly compliant, MCP contractures can typically be fully corrected even in advanced disease. Conversely, the PIP joint is notoriously unforgiving. Any degree of PIP joint contracture that impairs the patient's activities of daily living (typically >15 to 20 degrees) is an indication for surgery. Delaying intervention for PIP contractures often results in irreversible secondary changes to the joint capsule and collateral ligaments, precluding full anatomical correction.
Indications and Contraindications Summary
| Parameter | Indications for Surgical Intervention | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Volkmann Contracture | Established intrinsic-plus/minus deformity; Obliterated first web space; Failed conservative management; Functional deficit in grasp/pinch. | Active, untreated acute compartment syndrome (requires emergent fasciotomy, not reconstruction); Medically unstable patient. | Severe, irreversible joint ankylosis (may require arthrodesis instead); Lack of patient compliance for post-op therapy. |
| Dupuytren Disease | MCP joint contracture > 30 degrees; PIP joint contracture > 15-20 degrees; Positive Hueston tabletop test; Painful nodules (rare). | Active, severe complex regional pain syndrome (CRPS); Active local skin infection. | Mild, non-progressive disease; Severe systemic comorbidities precluding anesthesia; Extreme advanced age with low functional demands. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of avoiding intraoperative catastrophes and ensuring a durable functional outcome. The reconstructive surgeon must employ advanced diagnostic adjuncts and precise surgical templating.
Advanced Diagnostic Modalities
In the setting of chronic ischemic contractures, Magnetic Resonance Imaging (MRI) is an indispensable tool. High-resolution MRI allows the surgeon to precisely map the extent of myonecrosis and differentiate between viable, contractile muscle tissue and dense fibrous scar. This mapping dictates the surgical strategy: if sufficient viable muscle remains, a muscle slide procedure (such as the Page-Scaglietti-Gosset flexor origin release) may be viable. If the muscle is entirely replaced by fibrosis, the surgeon must plan for free functional muscle transfers, such as a microvascular free gracilis transfer innervated by the anterior interosseous nerve.
For Dupuytren disease, advanced imaging is rarely required. The diagnosis and surgical planning are entirely clinical. The surgeon must meticulously assess the quality of the overlying palmar skin. Severe dermal tethering, skin pitting, or a history of multiple recurrences may necessitate a dermofasciectomy (excision of the diseased fascia and the involved overlying skin) followed by full-thickness skin grafting, rather than a standard regional fasciectomy.
Surgical Templating and Patient Positioning
Preoperative templating involves designing the surgical incisions to maximize exposure while preventing secondary scar contractures. In Dupuytren surgery, the Brunner zig-zag incision is the gold standard. The apices of the triangular flaps must be placed precisely at the flexion creases to prevent longitudinal scar contracture. Alternatively, longitudinal incisions incorporating multiple Z-plasties can be utilized.
The patient is positioned supine on the operating table with a radiolucent hand board. A pneumatic tourniquet is applied to the proximal arm. Crucially, in severe Dupuytren disease, the limb should be exsanguinated by gravity elevation rather than an Esmarch bandage. Compressing the limb with an Esmarch can empty the digital arteries, rendering the neurovascular bundles pale and nearly indistinguishable from the surrounding white fibrotic cords. Gravity exsanguination leaves a small amount of venous blood within the vessels, aiding in their visual identification during meticulous microscopic dissection.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of severe intrinsic contracture release and Dupuytren fasciectomy requires extreme patience, loop magnification, and a systematic, tissue-sparing approach.
Radical Release of Intrinsic Contractures and the Adducted Thumb
The adduction contracture of the thumb is one of the most debilitating sequelae of severe hand trauma or ischemia. The fibrosis of the adductor pollicis and the first dorsal interosseous obliterates the first web space. Simple fascial release is universally inadequate; the fibrotic muscle must be radically recessed or excised.
Step 1: Release and Defect Creation
The procedure begins with a generous incision along the contracted first web space. The surgeon systematically releases the fibrotic fascia, the insertion of the adductor pollicis, and the first dorsal interosseous. The dissection must remain strictly extra-capsular to avoid destabilizing the carpometacarpal (CMC) joint. In extreme, long-standing cases where the bony architecture has adapted to the contracture, a trapezoidal osteotomy or excision of the index metacarpal may be required to artificially widen the web space and provide local filleted skin for coverage. Following the radical release, the thumb is forcefully abducted and extended. This maneuver reveals a massive, raw, diamond-shaped soft-tissue defect on the palmar and dorsal aspects of the web space, which cannot be closed primarily without recreating the contracture.

Figure 1: Web space deepening after skin division and muscle recession, demonstrating the raw, diamond-shaped palmar and dorsal defect.
Web Space Deepening with Cross-Arm Flap Reconstruction
To provide durable, vascularized coverage of this massive defect, a staged cross-arm flap is a highly reliable technique, particularly when local tissue is heavily scarred or unavailable.
Step 2: First-Stage Flap Coverage
A cross-arm flap is meticulously designed on the medial or lateral aspect of the contralateral arm, depending on patient comfort and vascular anatomy. The flap is templated using a sterile glove wrapper to match the exact dimensions of the diamond-shaped defect. The flap is typically designed with two distinct triangular components: a distal triangular flap (b) and a proximal triangular flap (a).
The distal triangular flap (b) is elevated, ensuring the inclusion of the deep fascia to protect the subdermal plexus. It is then transferred and sutured directly into the dorsal aspect of the thumb web defect of the affected hand. The donor site on the arm is partially closed or grafted. The patient's affected arm is then immobilized in a secure, highly customized splint, resting comfortably against the contralateral arm to absolutely prevent any tension, shearing, or torsion on the fragile flap pedicle.
Figure 2: Position of the hand with the triangular distal flap (b) sutured into the dorsal thumb web defect. The outline of the proximal triangular flap (a), which will be used for palmar web coverage during the second stage, is visible.
Step 3: Second-Stage Division and Inset
The patient returns to the operating room approximately 3 to 4 weeks later. By this time, robust neovascularization from the recipient bed into the flap has occurred. The flap pedicle is carefully divided. The proximal triangular flap (a) is then elevated from the donor arm, transferred, and meticulously inset into the palmar aspect of the web space defect. The resulting reconstruction provides a deep, wide, and highly supple first web space, permanently correcting the adduction contracture.
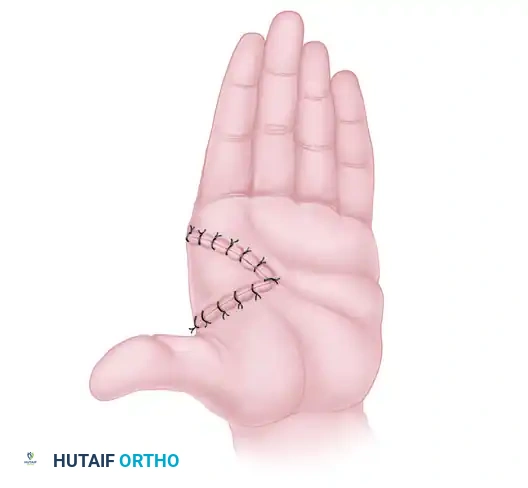
Figure 3: Final web space reconstruction after the transfer and inset of the palmar flap at the second-stage operation, 3 weeks later.
Regional Fasciectomy for Dupuytren Disease
For Dupuytren disease, regional fasciectomy remains the gold standard. The skin is incised using a Brunner zig-zag approach. Full-thickness skin flaps are elevated, meticulously separating the dermis from the underlying pathological cords. The subdermal vascular plexus must be preserved to prevent skin flap necrosis.
The dissection begins proximally in the palm, where the anatomy is relatively undisturbed. The digital neurovascular bundles are identified and protected with vessel loops. The surgeon then traces the bundles distally. When encountering the spiral cord, extreme caution is exercised. The cord is sharply divided and excised, allowing the neurovascular bundle to drop back into its normal, protected anatomical bed. The pretendinous and central cords are then excised en bloc.
Following excision, the joints are gently manipulated into extension. If a PIP joint contracture persists after complete cord excision, a stepwise joint release is performed: first, dividing the accessory collateral ligaments, followed by release of the volar plate if necessary. The tourniquet is deflated prior to closure to ensure meticulous hemostasis, thereby preventing postoperative hematoma.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of severe intrinsic contractures and Dupuytren disease carries a significant risk profile. The surgeon must be prepared to manage both intraoperative catastrophes and frustrating postoperative sequelae.
Intraoperative and Postoperative Sequelae
The most feared intraoperative complication is the iatrogenic transection of a digital nerve or artery, which occurs in approximately 1% to 3% of primary Dupuytren fasciectomies, and up to 10% in revision surgeries. If a nerve is transected, it must be repaired immediately under operative microscopy using 8-0 or 9-0 epineurial sutures. Arterial injury is often well-tolerated due to the dual blood supply of the digit, but if both digital arteries are compromised, immediate microvascular vein grafting is mandatory to prevent digital necrosis.
Postoperatively, hematoma formation is the most common complication. A hematoma acts as a nidus for infection and profound fibrosis, severely compromising the final functional outcome. Meticulous hemostasis and the selective use of closed suction drains are critical preventive measures.
A unique and devastating complication is the postoperative "flare reaction" (a localized form of Complex Regional Pain Syndrome). This presents 2 to 4 weeks postoperatively with severe pain, diffuse edema, joint stiffness, and vasomotor instability. Management requires immediate, aggressive intervention, including high-dose oral corticosteroids, intensive hand therapy, and sympathetic nerve blocks.
Complications and Salvage Strategies Summary
| Complication | Estimated Incidence | Pathophysiology / Etiology | Salvage Management & Prevention |
|---|---|---|---|
| Digital Nerve Transection | 1% - 3% (Primary) 5% - 10% (Revision) |
Displacement by the spiral cord; Dissection in scarred beds. | Immediate microsurgical epineurial repair. Prevention: Proximal to distal dissection under loop magnification. |
| Postoperative Hematoma | 2% - 5% | Inadequate hemostasis; Rebound vasodilation post-tourniquet. | Immediate evacuation in the OR to prevent skin flap necrosis and severe scarring. Prevention: Tourniquet deflation prior to closure. |
| Flare Reaction / CRPS | 5% - 10% | Exaggerated neuroinflammatory response to surgical trauma. | High-dose oral corticosteroids taper (e.g., Prednisone); Aggressive edema control; Stellate ganglion blocks. |
| Disease Recurrence | 20% - 50% (at 5 years) | Genetic diathesis; Incomplete excision of diseased fascia. | Revision fasciectomy; Dermofasciectomy with full-thickness skin grafting (FTSG) to halt local recurrence. |
| Skin Flap Necrosis | 2% - 4% | Damage to the subdermal plexus during flap elevation; Excessive tension on closure. | Debridement and healing by secondary intention or skin grafting. Prevention: Thick flaps; McCash open palm technique. |
Phased Post-Operative Rehabilitation Protocols
The surgical release of severe contractures is merely the first phase of treatment. Without rigorous, supervised, and prolonged postoperative rehabilitation, the biological forces of scar contracture will inevitably pull the hand back into its deformed posture.
Immediate Postoperative Phase (Days 1 to 7)
Immediately following surgery, the hand is immobilized in a bulky, non-compressive, soft dressing reinforced with a volar plaster or thermoplastic orthosis. The positioning of this orthosis is dictated by the specific pathology treated.
* For Dupuytren Releases: The hand is splinted with the wrist in neutral, the MCP joints in 0 to 10 degrees of flexion (to prevent collateral ligament shortening), and the PIP joints in maximum safe extension.
* For Intrinsic Contracture Releases: The hand must be splinted in an "intrinsic-minus" position (MCP joints extended, IP joints flexed). This specific posture places maximum tension on the healing intrinsic muscles, preventing them from scarring down in a shortened, contracted state.
Strict elevation above heart level is mandatory to combat acute postoperative edema. The patient is instructed to perform active range of motion (ROM) exercises of the shoulder, elbow, and uninvolved digits to maintain global upper extremity function and promote lymphatic drainage.
Subacute Phase and Orthotic Management (Weeks 1 to 6)
At the first postoperative visit (typically 5 to 7 days), the bulky dressing is removed. A custom, lightweight thermoplastic extension orthosis is fabricated by a certified hand therapist.
Supervised occupational therapy is initiated. The focus is on active and active-assisted ROM exercises to promote differential tendon gliding and prevent the formation of dense peritendinous adhesions. Passive ROM is introduced cautiously, ensuring that excessive force is not applied to the healing skin flaps or the newly reconstructed web spaces (such as the cross-arm flap inset).
Night splinting is strictly enforced. The biological remodeling of scar tissue takes months, and the myofibroblasts within the surgical bed will continuously attempt to contract. Night splinting in maximum extension mechanically counteracts this cellular force. This regimen must be maintained religiously for a minimum of 3 to 6 months.
Advanced Strengthening and Functional Restoration (Weeks 6 to 12+)
Once the incisions have fully epithelialized and the cross-arm flap has completely stabilized, aggressive scar management begins. This includes deep friction massage, the application of silicone gel sheeting, and the use of elastomer putty to soften the surgical scar and reduce dermal tethering.
Progressive strengthening exercises are introduced at 6 to 8 weeks. Therapy focuses on restoring functional grip strength, lateral pinch, and tripod pinch. Work-hardening programs and simulated activities of daily living are incorporated to ensure the patient can return to their preoperative occupational and recreational activities. Maximum medical improvement is typically not reached until 6 to 12 months postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The modern management of intrinsic contractures and Dupuytren disease is built upon decades of meticulous anatomical research and rigorous clinical trials. The orthopedic surgeon must be intimately familiar with this foundational literature.
Historical Milestones and Foundational Studies
The anatomical basis of Dupuytren surgery was revolutionized by the landmark studies of McFarlane in the 1970s. McFarlane meticulously mapped the normal palmar fascia and definitively described how these normal bands transform into the pathological cords that dictate the clinical deformity. His description of the spiral cord and its displacement of the neurovascular bundle remains the most critical piece of anatomical knowledge for any surgeon performing a fasciectomy.
Tubiana later expanded on this work, developing the widely utilized Tubiana staging system, which quantifies the total deformation of the ray and guides surgical decision-making. In the realm of ischemic contractures, Seddon's classification of Volkmann contracture (Mild, Moderate, Severe) established the algorithmic approach to reconstruction, dictating when muscle slides are appropriate versus when free functional muscle transfers are mandatory.
Contemporary Evidence and Best Practices
In recent years, the management of Dupuytren disease has seen a surge in minimally invasive techniques. Percutaneous Needle Aponeurotomy (PNA) and collagenase clostridium histolyticum (CCH) injections emerged as popular alternatives to open surgery.
However, long-term, multi-center randomized controlled trials have provided crucial perspective. While PNA and CCH offer rapid recovery and minimal immediate morbidity, their 5-year recurrence rates are alarmingly high (often exceeding 60-70%), particularly for PIP joint contractures. Consequently, major orthopedic and hand surgery societies (such as the ASSH and AAOS) maintain that open regional fasciectomy remains the gold standard for achieving durable, long-term correction, particularly in younger patients, those with severe PIP joint involvement, or those exhibiting the aggressive Dupuytren diathesis. The integration of radical surgical release, sophisticated flap coverage (such as the cross-arm flap for web space deepening), and evidence-based rehabilitation protocols remains the definitive paradigm for restoring the severely contracted hand.
