Barsky Technique for Cleft Hand Closure: A Comprehensive Surgical Guide

Key Takeaway
The Barsky technique for cleft hand closure is a foundational orthopedic procedure designed to restore both function and aesthetics in central ray deficiencies. By utilizing a distally based, diamond-shaped flap and precise metacarpal approximation, surgeons can reconstruct the commissure while minimizing contracture risk. This guide details the step-by-step surgical approach, biomechanical considerations, and postoperative protocols essential for optimal outcomes in pediatric hand reconstruction.
Comprehensive Introduction and Patho-Epidemiology
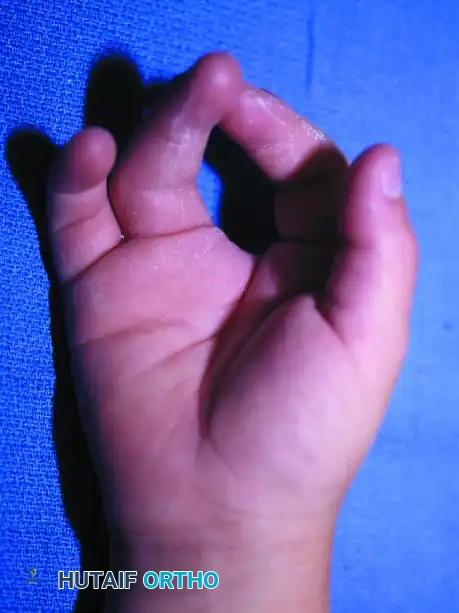
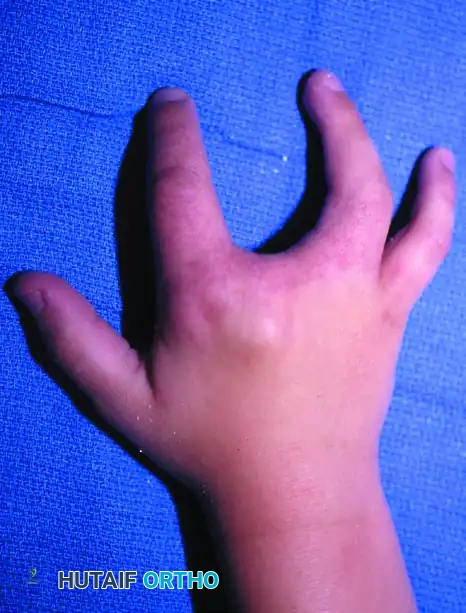
Central ray deficiency, most frequently designated in the surgical literature as "cleft hand" or historically as "split hand malformation," represents a profoundly complex congenital anomaly characterized by the failure of formation of the central digits and their corresponding metacarpals. This dysmorphogenesis results in a pathognomonic V-shaped or U-shaped central cleft that bifurcates the hand into distinct radial and ulnar functional units. The structural absence fundamentally disrupts the normal transverse metacarpal arch and eliminates the deep transverse metacarpal ligament, thereby initiating a cascade of biomechanical imbalances that lead to the progressive divergence of the adjacent border metacarpals.
From an embryological perspective, typical cleft hand is widely understood to result from a central wedge defect in the apical ectodermal ridge (AER) during the early stages of upper limb bud development, specifically between the fourth and seventh weeks of gestation. The AER is the critical signaling center responsible for proximodistal limb outgrowth and the orchestration of underlying mesenchymal condensation. A localized failure or premature apoptosis within the central portion of the AER leads to the cessation of central ray development. Genetic mapping has strongly associated these typical cleft hand presentations with mutations in the DLX5 and DLX6 genes, as well as aberrations in the WNT and Sonic Hedgehog (SHH) signaling pathways, which govern the radioulnar patterning of the limb bud.
Epidemiologically, typical cleft hand is a rare anomaly, with an estimated incidence ranging from 1 in 90,000 to 1 in 120,000 live births. It frequently presents in an autosomal dominant inheritance pattern with highly variable penetrance and expressivity, meaning that familial presentations can range from mild central syndactyly to severe oligodactyly. Furthermore, the condition is frequently bilateral and is often associated with analogous central deficiencies of the feet (split-hand/split-foot malformation or SHFM). The surgeon must maintain a high index of suspicion for syndromic associations, most notably EEC syndrome (Ectrodactyly, Ectodermal dysplasia, and Cleft lip/palate), which necessitates a multidisciplinary approach encompassing genetic counseling, craniofacial surgery, and pediatric dentistry alongside orthopedic intervention.
The primary objectives of surgical intervention in central ray deficiency are multifaceted: to restore functional pinch and grasp mechanics, to close the profound central soft tissue defect, to reconstruct a robust and stable commissure that resists proximal migration, and to optimize the overall aesthetic appearance of the hand to mitigate psychosocial distress as the child matures. The Barsky Technique, originally described in the mid-20th century, remains an absolute cornerstone in the operative armamentarium for managing typical cleft hands. It utilizes a meticulously designed, distally based diamond flap to recreate the web space while physically approximating the divergent metacarpals, thereby restoring the foundational architecture of the hand.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the aberrant surgical anatomy is mandatory before undertaking a cleft hand reconstruction, as the neurovascular and musculotendinous structures rarely adhere to textbook descriptions. Osteologically, the typical cleft hand lacks the entire third ray (middle finger phalanges and the third metacarpal). However, the presentation is highly variable; remnants of the central ray frequently persist as transversely oriented, hypoplastic bony ossicles—often termed "cross-bones." These anomalous transverse elements are typically tethered between the index and ring metacarpals by dense fibrous bands, acting as a rigid mechanical block that prevents the manual approximation of the border rays.

The ligamentous architecture is similarly disrupted, most notably through the complete absence of the deep transverse metacarpal ligament (DTML) across the central cleft. In the normal hand, the DTML serves as the primary static stabilizer of the transverse metacarpal arch, tethering the volar plates of the metacarpophalangeal (MCP) joints together and preventing splaying of the metacarpal heads during forceful grasp. In the cleft hand, the absence of this ligamentous tether leaves the index and ring metacarpals mechanically uncoupled. Consequently, the intrinsic muscles—specifically the dorsal and volar interossei—exert un-opposed deforming forces. Every time the child attempts to pinch or grasp, the flexor and extensor tendons, which may also exhibit anomalous bifurcations or central tethering, exacerbate the splaying of the border digits.
Neurovascular arborization within the cleft hand is notoriously unpredictable and poses the greatest risk during deep dissection. The superficial palmar arch is frequently incomplete or entirely absent, with the digital arteries to the index and ring fingers arising from disparate, independent branches of the radial and ulnar arteries. The common digital artery that would normally supply the adjacent sides of the index and middle fingers may be absent, or it may bifurcate unusually proximal or distal to the expected web space level. Similarly, the common digital nerves often exhibit proximal bifurcations or transverse communicating branches that span directly across the cleft. These structures are highly susceptible to iatrogenic transection or traction injury during the reduction of the metacarpals if not meticulously identified and mobilized.
Biomechanically, the cleft hand functions as two independent, uncoordinated units (a radial pinch unit and an ulnar grasp unit) rather than a cohesive, synergistically functioning hand. The divergence of the metacarpals increases the mechanical advantage of the abductor forces while diminishing the efficiency of the adductor and flexor mechanisms. The Barsky procedure is biomechanically designed to convert these two disparate units back into a single functional entity. By physically tethering the metacarpal necks with heavy, non-absorbable sutures or tendon grafts, the surgeon artificially recreates the DTML. This restores the transverse metacarpal arch, normalizes the vector forces of the intrinsic and extrinsic musculature, and allows for coordinated, powerful grasp and precision pinch.
Exhaustive Indications and Contraindications
Surgical decision-making in the reconstruction of the cleft hand is heavily dictated by the functional status of the first web space (the thumb-index web). A narrowed, contracted, or completely absent thumb web space severely limits thumb opposition and functional grasp, unequivocally taking surgical precedence over the closure of the central cleft itself. The internationally accepted standard for categorizing these central deficiencies and guiding operative strategy is the Manske and Halikis Classification, which categorizes the anomaly based exclusively on the functional morphology of the thumb web space.
Manske and Halikis Surgical Classification
The Manske and Halikis system is indispensable for the operating surgeon, as it directly dictates the hierarchy of surgical interventions. Type I anomalies are characterized by a normal thumb web space with no narrowing or contracture. In these cases, the primary pathology is isolated to the central cleft, and the patient is an ideal candidate for an isolated Barsky cleft closure combined with local tissue reduction and metacarpal approximation. Type IIA anomalies present with a mildly narrowed thumb web space. Surgical management for Type IIA involves local pedicle flaps, such as single or multiple Z-plasties, to widen the first web space simultaneously with the standard cleft closure techniques.
Type IIB anomalies exhibit a moderately narrowed thumb web space that requires more extensive soft tissue mobilization than simple Z-plasties can provide. These cases necessitate the use of dorsal or volar pedicle flaps mobilized directly from the redundant skin of the cleft to reconstruct the thumb web, often supplemented with full-thickness skin grafts, alongside the cleft closure. Type III anomalies are defined by a severely narrowed thumb web space, essentially presenting as a severe syndactyly or rigid contracture of the first web. Surgical recommendations here mandate aggressive syndactyly release utilizing skin grafts and large pedicle flaps from the cleft. In severe Type III cases, the excision of the index ray bony elements (index ray transposition or amputation) may be strictly required to create a functional first web space, prioritizing thumb function over a five-digit appearance.
Type IV anomalies represent a merged web and cleft, where the normal thumb web space is entirely obliterated, and the central cleft itself functions as the primary web space for the thumb. In these complex presentations, formal cleft closure is absolutely contraindicated, as closing the cleft would eliminate the only functional web space the child possesses. Interventions are limited to soft tissue reduction and stabilization of the metacarpophalangeal joints. Finally, Type V anomalies involve the complete absence of the thumb web space, often accompanied by severe hypoplasia or aplasia of the thumb itself. Cleft closure is strictly contraindicated; surgical focus shifts entirely to restoring fundamental grasp mechanics through complex procedures such as toe-to-hand transfers, pollicization, or metacarpal lengthening.
Patient Selection and Contraindications
| Classification / Condition | Surgical Indication | Contraindications & Considerations |
|---|---|---|
| Manske Type I | Ideal candidate for standard Barsky closure. | None, provided patient is medically stable for anesthesia. |
| Manske Type IIA | Barsky closure + First web Z-plasty. | Do not ignore the mild contracture; failure to address it will lead to worsening thumb adduction post-cleft closure. |
| Manske Type IIB & III | Cleft skin utilized for thumb web reconstruction (e.g., Snow-Littler). | Standard Barsky is contraindicated as an isolated procedure. Thumb web must be prioritized. |
| Manske Type IV & V | MCP stabilization, potential pollicization. | Absolute Contraindication for cleft closure. Closing the cleft destroys the only functional grasp space. |
| Severe Syndromic Presentation | Delay surgery until medically optimized. | Severe cardiac or respiratory anomalies (e.g., in EEC syndrome) that pose unacceptable anesthesia risks. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful cleft hand reconstruction. The evaluation begins with a meticulous clinical examination, observing the child's spontaneous use of the hand during play. The surgeon must assess the presence and strength of pinch, the capability for cylindrical grasp, and the independence of the border digits. The mobility and suppleness of the first web space must be rigorously tested to accurately assign a Manske and Halikis classification. Furthermore, the surgeon should evaluate for any associated syndactyly of the border digits (e.g., syndactyly of the ring and small fingers), which is a common concomitant finding that may require staged releases.
Radiographic evaluation is critical for mapping the aberrant osteology. Standard posteroanterior (PA), lateral, and oblique radiographs of the hand and wrist are mandatory. The surgeon must carefully template the alignment of the divergent metacarpals and actively search for transverse "cross-bones" or delta phalanges within the cleft space. These anomalous bony elements dictate the extent of the deep extraperiosteal dissection required. While advanced imaging modalities such as Magnetic Resonance Imaging (MRI) or high-resolution ultrasonography are not routinely required for typical cleft hands, they may be indicated in highly atypical presentations to map out complex neurovascular arborizations or anomalous intrinsic muscle bellies prior to surgical exploration.
The optimal timing for surgical intervention is a subject of ongoing academic debate, but the general consensus favors operative reconstruction between 12 and 18 months of age. At this developmental stage, the anatomical structures are sufficiently large to permit safe, meticulous dissection of the neurovascular bundles under loupe magnification. Crucially, intervening at this age allows for the restoration of normal hand architecture before the child's cortical motor patterns for pinch and grasp become hardwired to the deformed state. Early surgery harnesses the immense neuroplasticity of the pediatric brain, facilitating seamless functional integration of the newly reconstructed hand.
Operative setup requires the patient to be positioned supine on the operating table with the affected extremity extended onto a stable, radiolucent hand table to allow for intraoperative fluoroscopy. The procedure is performed under general anesthesia. A well-padded pediatric pneumatic tourniquet is applied to the proximal upper arm. Exsanguination is achieved gently via elevation or the use of an Esmarch bandage, and the tourniquet is inflated to an age- and weight-appropriate pressure, typically ranging from 200 to 250 mmHg. The use of surgical loupe magnification (minimum 2.5x to 3.5x) is an absolute necessity for the safe identification and preservation of the delicate, often anomalous, digital neurovascular structures.
Step-by-Step Surgical Approach and Fixation Technique
The Barsky technique is an elegant, highly effective procedure that relies on precise geometric flap design to create a natural, sloping commissure that resists the notorious complication of dorsal migration, commonly referred to as "web creep."
Flap Design and Incision
Precise preoperative marking is arguably the most critical step in preventing postoperative scar contractures. The hallmark of the Barsky technique is the distally based diamond flap. The surgeon must mark a diamond-shaped flap on one side of the opposing surfaces of the involved fingers—typically selecting the side with more mobile, redundant skin.
The positioning of this flap is paramount: it must be placed with a distinct dorsal bias. This dorsal positioning is essential to allow the flap to fold upon itself and create a gentle, natural volar slope of the reconstructed commissure, mimicking the normal anatomy of the human web space. The base of the diamond flap should be approximately 1 cm wide, and the length should be meticulously measured to be 1.5 times longer than the width. Under strict tourniquet control, the flap is sharply elevated.
A critical surgical warning must be heeded during this elevation: the flap must be defatted down to the level of the subdermal vascular plexus. Failure to adequately defat the flap will result in a bulky, functionally obstructive, and aesthetically displeasing web space. Conversely, aggressive defatting that violates the delicate subdermal plexus will inevitably lead to partial or complete flap necrosis. The surgeon must maintain a meticulous dissection plane just deep to the dermis. Once the diamond flap is safely elevated, a continuous incision is made from the free end of the flap proximally along the opposing surfaces of the V-shaped cleft, extending all the way to the proximal apex.
Deep Exposure and Extraperiosteal Dissection
Following the initial skin incisions, the dissection is deepened through the subcutaneous tissues. The immediate priority is the identification, mobilization, and absolute protection of the digital neurovascular bundles. Given the high propensity for anomalous branching patterns in cleft hands, the surgeon must trace the arteries and nerves proximally into the palm to ensure they are not tethered or at risk of traction injury during the subsequent metacarpal approximation. Any transverse neural communicating branches that tether the border digits must be carefully dissected and, if necessary, mobilized through epineurial interfascicular dissection to allow for tension-free approximation.
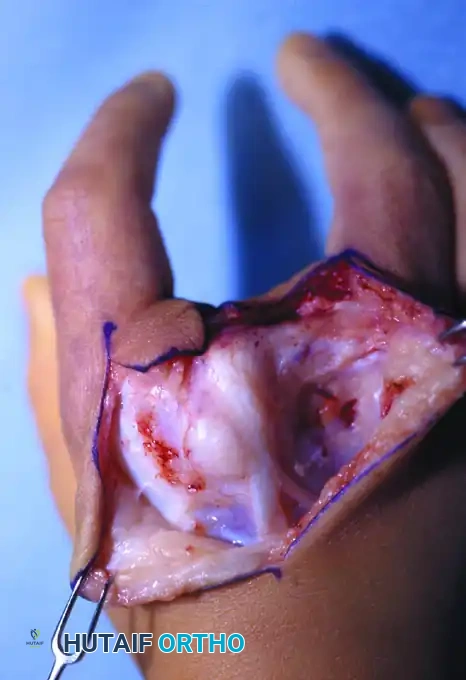
The deep dissection proceeds to expose the divergent metacarpals. It is of paramount importance that this exposure is performed extraperiosteally. In the pediatric patient, the periosteum is thick and highly osteogenic; stripping it can damage the delicate physes or lead to unpredictable, massive bony overgrowth and iatrogenic synostosis between the metacarpals. Maintaining a strict extraperiosteal plane preserves the robust vascular supply to the bone and protects the child's future growth potential.
Once the metacarpals are exposed, the surgeon must radically excise any excess soft tissue residing within the cleft. This includes anomalous intrinsic muscle bellies, dense fibrotic bands, and any polydactylous bony elements or transverse ossicles (cross-bones). These elements act as a rigid mechanical block; if they are not completely excised, apposing the metacarpals will be physically impossible, or it will place undue, catastrophic tension on the ligamentous reconstruction.
Metacarpal Approximation and Ligament Reconstruction
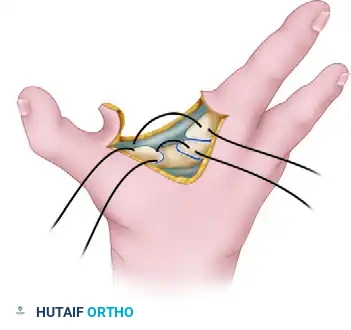
With the cleft space cleared of all mechanical blocks, the divergent metacarpals must be physically tethered to restore the transverse metacarpal arch and substitute for the absent deep transverse metacarpal ligament. Using a fine Kirschner wire (K-wire) or a small-diameter drill bit, the surgeon drills two transverse holes in each of the opposing metacarpals, positioning them just proximal to the metacarpal heads to avoid violating the distal physes or the articular cartilage.
A heavy, non-absorbable suture—typically a 0 or 2-0 braided polyester or polypropylene, depending on the absolute size of the child's skeletal structures—is passed through the drilled holes in a figure-of-eight or horizontal mattress configuration. The surgeon or an assistant then manually approximates the metacarpals, effectively closing the central cleft space and restoring the normal parallel alignment of the rays. While holding the bones firmly in their reduced, anatomical position, the heavy suture is tied securely.
In older children, or in cases presenting with severe, long-standing divergence, a simple heavy suture may be insufficient; it may eventually cut through the osteopenic bone (the "cheese-wire" effect) or stretch over time. In such robust instances, the surgeon should strongly consider augmenting the closure with a circumferential tendon graft. A slip of the extensor carpi radialis longus (ECRL), palmaris longus, or a local slip of an anomalous extensor tendon can be harvested and woven circumferentially through the metacarpal necks, providing a biological, durable reconstruction of the DTML.
Soft Tissue Reconstruction and Closure
With the skeletal and ligamentous architecture definitively restored, the surgeon's attention turns to the complex management of the soft tissue envelope. Closing a linear incision longitudinally within the web space is strictly and absolutely contraindicated. A straight-line closure across a joint or web space will inevitably lead to a longitudinal scar contracture, resulting in recurrent web creep and severe restriction of digital abduction.

To prevent this, the dorsal and palmar skin incisions are closed from proximal to distal utilizing interdigitating flaps. As the closure proceeds distally, the surgeon must excise excess skin in a precise geometric pattern to create multiple Z-plasties or W-plasties along both the dorsal and palmar surfaces. This technique breaks up the linear scar line, redistributes tension, and accommodates the complex three-dimensional contours of the hand.
The distally based diamond finger flap is then brought across the newly approximated intermetacarpal space and meticulously inset into the commissure. Because the wide V-shaped cleft has been mechanically closed, there will inevitably be a significant amount of redundant skin.

A crucial technical step must be observed here: before suturing the diamond flap into its final position, any excess skin must be excised from the dorsum of the hand, rather than trimming the flap itself. Trimming the carefully designed diamond flap risks compromising its precise geometric dimensions and its delicate subdermal vascular supply.

Ensure all skin edges are meticulously approximated with fine, absorbable sutures. In pediatric patients, the use of 5-0 or 6-0 chromic gut or fast-absorbing plain gut is highly recommended to completely avoid the psychological trauma and logistical difficulty of suture removal in the clinic setting.
Complications, Incidence Rates, and Salvage Management
While the Barsky technique is highly reliable when executed with precision, the complex, anomalous anatomy of the cleft hand inherently predisposes the procedure to several specific complications. Surgeons must be hyper-vigilant during both the operative execution and the postoperative monitoring phases to identify and mitigate these issues early.
| Complication | Estimated Incidence | Etiology / Prevention | Salvage Management |
|---|---|---|---|
| Flap Necrosis (Partial/Total) | 5% - 10% | Caused by overly aggressive defatting violating the subdermal plexus, or excessive tension during inset. Prevent by maintaining a superficial dissection plane and ensuring tension-free closure. | Superficial epidermolysis is managed with local wound care and non-adherent dressings. Full-thickness necrosis requires debridement and secondary full-thickness skin grafting. |
| Recurrent Clefting / Divergence | 10% - 15% | Results from heavy suture breakage, "cheese-wiring" through osteopenic bone, or failure to excise transverse bony cross-bones. Prevent by using thick non-absorbable sutures, tendon grafts, and radical extraperiosteal clearing. | Revision surgery with robust circumferential tendon grafting (e.g., palmaris longus) and potential temporary K-wire transfixion of the metacarpals. |
| Web Creep (Distal Migration) | 15% - 20% | Distal migration of the commissure due to longitudinal scar contracture. Prevented by strict adherence to interdigitating Z-plasties and ensuring the diamond flap has a dorsal bias. | Secondary web space deepening using dorsal rectangular flaps, V-Y advancement flaps, or four-flap Z-plasties. |
| First Web Space Contracture | Variable (often iatrogenic) | Occurs if a Manske Type II or III deficiency is misdiagnosed as Type I. The cleft is closed, but the hand is functionally poor due to lack of thumb opposition. | Staged reconstruction utilizing a Snow-Littler procedure, first dorsal interosseous fascia release, or index ray transposition to widen the thumb web. |
| Neurovascular Injury | < 2% | Iatrogenic transection of anomalous nerves or vessels crossing the cleft. Prevented by meticulous loupe-assisted dissection and proximal tracing of all structures. | Immediate microsurgical primary repair or interposition nerve/vein grafting. |
Flap necrosis is arguably the most immediate postoperative concern. It typically manifests within the first 48 to 72 hours as venous congestion (a dark, violaceous appearance with brisk capillary refill that rapidly becomes sluggish) or arterial insufficiency (a pale, cool flap with absent capillary refill). If venous congestion is noted, loosening of tight dressings and elevation are the first-line treatments; medicinal leeches (Hirudo medicinalis) are rarely practical in pediatric hand flaps but can be considered in catastrophic congestion. Total necrosis necessitates a return to the operating room for debridement and reconstruction, drastically compromising the final functional and aesthetic outcome.
Recurrent clefting and web creep are long-term complications that typically become apparent months to years after the initial reconstruction, often coinciding with periods of rapid skeletal growth. The pediatric skeleton's capacity for remodeling can sometimes overcome the static surgical tether, especially if the deforming forces of the intrinsic muscles were not adequately neutralized. Regular, long-term radiographic and clinical follow-up until skeletal maturity is essential to monitor for these late-onset complications.
Phased Post-Operative Rehabilitation Protocols
The ultimate success of the Barsky cleft closure relies just as heavily on strict, uncompromising postoperative immobilization as it does on meticulous surgical technique. The heavy inter-metacarpal sutures and the complex, interdigitating soft tissue flaps require an undisturbed environment to heal without tension.
Immobilization Phase (0 to 4 Weeks)
Immediately postoperatively, while the patient is still under anesthesia, a sterile, non-adherent dressing (e.g., Adaptic or Xeroform) is applied directly to the incision lines. A minimal amount of bulky, fluffed gauze is placed between the digits to absorb exudate, but the surgeon must strictly avoid excessive pressure or tight circumferential wrapping that could compromise the delicate venous outflow of the flaps.
A well-molded, fiberglass or plaster long-arm cast is then applied, extending from the proximal third of the humerus down to the level of the metacarpal heads, leaving the distal phalanges exposed for neurovascular monitoring. The rationale for a long-arm cast in this specific pediatric population is absolute. Pediatric patients possess cylindrical forearms; a short-arm cast is easily slipped off by an active toddler. Furthermore, a short-arm cast permits full pronation and supination of the forearm. These rotational movements generate significant shear forces across the carpus and metacarpals, which can easily pull out the newly placed metacarpal approximation sutures. A long-arm cast with the elbow immobilized at 90 degrees of flexion ensures absolute compliance and protects the surgical repair from rotational stress.
Functional Integration Phase (4 to 6+ Weeks)
The initial long-arm cast is worn continuously for a period of 3 to 4 weeks. At this milestone, the patient returns to the clinic, and the cast is carefully bivalved and removed. The surgeon must meticulously inspect the viability of all flaps, the integrity of the Z-plasties, and the clinical stability of the metacarpal approximation. If the thumb or border digits demonstrate a tendency to separate excessively upon cast removal, or if the child exhibits pain upon gentle passive manipulation, the bony and ligamentous healing is deemed insufficient. In this scenario, the patient is transitioned into another well-molded short-arm cast or a rigid thermoplastic splint for an additional 2 to 3 weeks.
Once clinical stability is unequivocally confirmed, rigid immobilization is discontinued. Due to the immense neuroplasticity and high adaptability of pediatric patients, formal, structured occupational therapy or specialized hand therapy is usually not required following a standard, uncomplicated Barsky closure. The child will naturally and instinctively incorporate the newly reconstructed, biomechanically sound hand into daily play, feeding, and exploratory activities. This spontaneous, play-based use serves as the absolute best form of functional rehabilitation, rapidly establishing new motor engrams in the cerebral cortex. However, parents must be thoroughly educated and instructed to perform gentle, daily scar massage using a non-perfumed emollient once the incisions are fully epithelialized and free of scabs. This massage helps to break down underlying subcutaneous adhesions, optimizes tissue pliability, and further mitigates the risk of late web space contracture.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for cleft hand anomalies is deeply rooted in a few landmark publications that continue to define modern orthopedic practice. Arthur J. Barsky’s seminal work, published in the Journal of Bone and Joint Surgery in 1964 ("Cleft Hand: Classification, Incidence, and Treatment"), remains the definitive text describing the geometric principles of the distally based diamond flap. Barsky was the first to articulate the necessity of the dorsal bias to recreate a natural commissure slope, a principle that has remained virtually unchanged for over half a century.
In 1995, Paul R. Manske and Christopher G. Halikis published their groundbreaking classification system in the Journal of Hand Surgery ("Surgical Classification of Central Deficiency According to the Thumb Web"). This paper fundamentally shifted the surgical paradigm away from merely closing the aesthetic central defect and toward prioritizing the functional mechanics of the first web space. The Manske and Halikis classification is now the universally accepted algorithm that dictates whether a patient requires a simple Barsky closure, a complex Snow-Littler procedure (which transfers the index ray ulnar-ward while utilizing the cleft skin to construct a massive thumb web), or if surgery is entirely contraindicated.
Further refinements have been contributed by Ueba (1981), who described the use of transverse flaps to prevent linear contractures, and Miura, who extensively documented the varied anomalous neurovascular anatomy encountered during these reconstructions. Current clinical guidelines, supported by the American Society for Surgery of the Hand (ASSH) and the Pediatric Orthopaedic Society of North America (POSNA), strongly advocate for early intervention (12-18 months), extraperiosteal dissection to protect physes, and the absolute prioritization of thumb opposition over the mere cosmetic closure of the central cleft.
