Surgical Management of Thumb Hypoplasia, Adduction Contractures, and Disproportion
Key Takeaway
Thumb hypoplasia and disproportion present complex reconstructive challenges. Management ranges from web space deepening for relative lengthening to complex opponensplasties for adducted thumbs. Conversely, macrodactyly requires the Millesi shortening technique. This guide details adduction contracture release via Z-plasty, opposition restoration using Huber or flexor digitorum superficialis transfers, and precise osteotomies, providing evidence-based protocols for orthopedic surgeons.
Comprehensive Introduction and Patho-Epidemiology
The thumb represents the singular most critical digit for human prehension, independently contributing to approximately 40% to 50% of overall hand function. Its highly specialized evolutionary development allows for the complex kinematic interplay required for opposition, precise tip-to-tip pinch, and powerful cylindrical grasp. Congenital or acquired anomalies that disrupt the morphological harmony, length, or spatial orientation of the thumb present profound functional and aesthetic challenges. The spectrum of thumb disproportion is vast, ranging from the structurally hypertrophied macrodactyly to the profoundly deficient hypoplastic or adducted thumb. As reconstructive orthopedic and hand surgeons, our mandate is to critically evaluate these deformities not merely as anatomical curiosities, but as complex biomechanical deficits requiring meticulous, individualized surgical restoration.
Thumb hypoplasia is intrinsically linked to radial longitudinal deficiency (RLD), representing a failure of formation along the preaxial (radial) border of the upper limb during the critical embryonic window between the fourth and eighth weeks of gestation. The incidence of thumb hypoplasia is estimated at 1 in 100,000 live births, though this figure rises significantly when considering minor morphological variants that never present for surgical evaluation. Bilateral involvement is observed in approximately 60% of cases. The patho-epidemiology of thumb hypoplasia is heavily characterized by its association with life-threatening systemic syndromes. The genetic disruptions affecting the zone of polarizing activity (ZPA) and the apical ectodermal ridge (AER) often concurrently impact the development of the cardiac, hematopoietic, and gastrointestinal systems.
A thorough understanding of the syndromic pathoanatomy is paramount. A morphologically short and slender metacarpal is a classic hallmark of Fanconi anemia (an autosomal recessive chromosomal instability disorder with severe aplastic anemia), Holt-Oram syndrome (characterized by cardiac septal defects), and VACTERL association. Conversely, a short and broad metacarpus may indicate Cornelia de Lange syndrome or diastrophic dwarfism. The presence of a slender distal phalanx demands immediate hematologic and cardiac screening. Furthermore, the isolated adducted thumb—often presenting with a severely contracted first web space and a flattened thenar eminence—is frequently transmitted as an autosomal dominant trait. This specific deformity is driven by an absence or severe hypoplasia of the thenar musculature, compounded by profound ligamentous laxity at the metacarpophalangeal (MCP) joint.
On the opposite end of the spectrum, thumb macrodactyly (local gigantism) is a rare, non-hereditary congenital anomaly characterized by the overgrowth of all mesenchymal elements, particularly fibroadipose tissue and bone. It may present in isolation or as a manifestation of syndromes such as Proteus syndrome, neurofibromatosis type 1 (NF1), or Klippel-Trenaunay-Weber syndrome. The disproportionately large thumb mechanically impedes hand function, obstructing the first web space and preventing effective opposition with the ulnar digits. Whether addressing the hypoplastic, adducted, or overgrown thumb, the surgeon must synthesize a deep understanding of embryology, genetics, and biomechanics to formulate a reconstructive strategy that prioritizes dynamic function over static appearance.
Detailed Surgical Anatomy and Biomechanics
The functional supremacy of the thumb is dictated by its unique osteoarticular architecture and the sophisticated balance of its intrinsic and extrinsic musculature. The foundation of thumb kinematics lies at the carpometacarpal (CMC) joint, a highly specialized biconcave saddle joint articulation between the trapezium and the first metacarpal. This geometric configuration permits a vast cone of circumduction, facilitating flexion, extension, abduction, adduction, and the critical rotational component of pronation required for opposition. Stability of the CMC joint is heavily reliant on a robust capsuloligamentous complex, most notably the anterior oblique ligament (the "beak ligament") and the dorsoradial ligament. In thumb hypoplasia (specifically Manske Type IIIB and above), the absence or severe dysplasia of the trapezium and these stabilizing ligaments renders the CMC joint incompetent, serving as the absolute contraindication for local reconstruction and the primary indication for index finger pollicization.
Distal to the CMC joint, the metacarpophalangeal (MCP) joint functions primarily as a condyloid hinge, providing crucial stability during pinch maneuvers. The MCP joint's stability is governed by the proper and accessory collateral ligaments, the volar plate, and the dynamic support of the intrinsic thenar musculature. In the adducted or hypoplastic thumb, the ulnar collateral ligament (UCL) is frequently attenuated or entirely absent. This pathoanatomy is critical; if an opponensplasty is performed without first addressing MCP joint instability, the newly transferred tendon will simply subluxate the proximal phalanx radially, resulting in a disastrous "Z-collapse" deformity (MCP hyperextension and interphalangeal flexion) rather than true opposition. The interphalangeal (IP) joint, stabilized by its own collateral ligaments and volar plate, relies on the balanced forces of the flexor pollicis longus (FPL) and extensor pollicis longus (EPL) for terminal control.
The musculotendinous anatomy of the thumb is divided into extrinsic and intrinsic groups. The extrinsics (EPL, EPB, APL, FPL) provide gross positioning and power, while the intrinsics (abductor pollicis brevis [APB], flexor pollicis brevis [FPB], opponens pollicis, and adductor pollicis) govern fine motor control and spatial orientation. True opposition is a composite movement driven primarily by the APB, which abducts, flexes, and pronates the first metacarpal. In congenital adduction contractures, the APB and opponens pollicis are typically aplastic. Surgical restoration of opposition (opponensplasty) requires routing a donor tendon (such as the flexor digitorum superficialis or abductor digiti minimi) along a specific vector—originating near the pisiform and inserting into the radial aspect of the MCP joint—to accurately replicate the biomechanical line of pull of the native APB.
Neurovascularly, the thumb is supplied by the princeps pollicis artery, a terminal branch of the radial artery, which bifurcates at the base of the proximal phalanx to form the radial and ulnar digital arteries. Venous drainage is predominantly dorsal. Sensation is mediated by the palmar digital branches of the median nerve and the dorsal sensory branch of the radial nerve (SBRN). In hypoplastic thumbs, the neurovascular bundles are often anomalous, displaced, or tethered by aberrant fascial bands (such as the "musculus lumbricalis pollicis"). Furthermore, in macrodactyly, the digital nerves are frequently grossly enlarged, tortuous, and infiltrated with fibroadipose tissue, complicating surgical dissection during debulking or shortening procedures. A profound respect for these anomalous neurovascular structures is mandatory to prevent catastrophic ischemic or neuropathic complications during reconstruction.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in thumb disproportion or hypoplasia must be rooted in a rigorous assessment of functional impairment rather than purely aesthetic deviation. A hypoplastic thumb that is merely short, yet possesses a stable CMC joint, functional intrinsic and extrinsic musculature, and adequate sensibility, rarely warrants surgical reconstruction. The primary goal of intervention is the restoration of prehension—specifically, the ability to achieve a stable, sensate, and powerful pinch and grasp. When the thumb's morphology or kinematics mechanically obstruct these functions, surgical correction becomes indicated. The timing of surgery is generally recommended between 12 and 24 months of age, capitalizing on the child's neuroplasticity for motor re-education while allowing sufficient anatomical growth to make delicate tissue handling feasible.
In the context of the short or hypoplastic thumb, the Manske classification dictates the surgical algorithm. Manske Types I and II generally require soft-tissue reconstruction, including first web space deepening, opponensplasty, and MCP joint stabilization. Type IIIA thumbs (deficient extrinsics and skeletal hypoplasia, but a stable CMC joint) represent the most complex reconstructive challenge, requiring staged tendon transfers and web space releases. The absolute critical determinant is the stability of the CMC joint. Manske Type IIIB (unstable CMC joint), Type IV (floating thumb), and Type V (complete aplasia) are absolute indications for index finger pollicization. Attempting to reconstruct a Type IIIB thumb is a historical error that universally results in a stiff, unstable, and non-functional post, ultimately requiring salvage amputation.
For the overgrown thumb (macrodactyly), indications for the Millesi shortening procedure or aggressive debulking include severe functional impairment due to spatial obstruction, progressive deviation of the digit, or inability to perform age-appropriate fine motor tasks. Contraindications to osseous shortening include active, rapidly progressive neurofibromatous overgrowth where the vascular supply is highly tenuous, or cases where the digital nerves are so massively infiltrated that any dissection would result in complete anesthesia. In such severe, progressive cases of macrodactyly where the digit is insensate and functionally obstructive, ray amputation may be the most prudent and functional choice.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Millesi Thumb Shortening | True macrodactyly causing functional impairment; Severe post-traumatic disproportion. | Dysvascular digit; Active, uncontrollable progressive overgrowth (e.g., severe Proteus syndrome). | Poor soft-tissue envelope; Pre-existing severe nail dystrophy. |
| First Web Space Deepening (Z-plasty / Flap) | Manske Type II & III hypoplasia; Congenital adduction contracture; Post-burn contracture. | Active local infection; Inadequate vascularity of donor flap site. | Mild contracture not limiting grasp (span < 30% reduced). |
| Opponensplasty (Huber / FDS Transfer) | Aplastic/hypoplastic thenar muscles (Manske II/IIIA); Median nerve palsy. | Unstable/absent CMC joint (Manske IIIB+); Stiff MCP joint without prior stabilization. | Lack of full passive thumb abduction (contracture must be released first). |
| MCP Joint Stabilization (Ligament Reconstruction) | Profound UCL/RCL laxity in hypoplastic thumb; Prevention of Z-collapse prior to opponensplasty. | Complete absence of proximal phalanx base or metacarpal head. | Mild laxity that dynamically stabilizes during active pinch. |
| Index Finger Pollicization | Manske Type IIIB, IV, and V hypoplasia/aplasia. | Severe anomalies of the index finger (stiff, insensate); Uncontrolled systemic illness. | Parental refusal (requires extensive preoperative counseling). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful reconstructive outcomes in congenital hand surgery. The initial evaluation extends far beyond the upper extremity. Given the high incidence of associated systemic anomalies in thumb hypoplasia, a multidisciplinary approach is mandatory. Every patient presenting with a hypoplastic thumb must undergo a comprehensive pediatric workup, including a complete blood count (CBC) to screen for Fanconi anemia, a renal ultrasound to rule out VACTERL association anomalies, and an echocardiogram to assess for Holt-Oram syndrome. Only after the patient is medically cleared by pediatric hematology, cardiology, and genetics should the orthopedic surgeon proceed with operative planning.
Clinical evaluation of the hand requires meticulous documentation of active and passive range of motion, pinch strength (if age-appropriate), and sensibility. The surgeon must critically assess the integrity of the first web space, measuring the absolute span of palmar abduction and the presence of any tight fascial bands. The stability of the CMC and MCP joints must be manually stressed under simulated pinch forces. For opponensplasty planning, the availability and strength of donor muscles (FDS of the ring finger, ADM, or EIP) must be confirmed. Radiographic evaluation includes standard posteroanterior, lateral, and Robert's view radiographs of both hands. In macrodactyly, these radiographs are utilized for precise digital templating. The surgeon must calculate the exact millimeter resection required from the proximal and distal phalanges to achieve symmetry with the contralateral digit. Advanced imaging, such as MRI or high-resolution ultrasound, is occasionally employed to confirm the presence or absence of specific extrinsic muscle bellies (e.g., FPL) or anomalous neurovascular structures prior to exploration.
In the operating theater, precise patient positioning and equipment setup are critical. The patient is placed supine with the affected upper extremity extended on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm over generous padding. For pediatric patients, the tourniquet pressure is typically set to 100 mmHg above the patient's systolic blood pressure, with strict adherence to inflation time limits (maximum 90 to 120 minutes before a reperfusion interval is required). The use of high-quality surgical loupe magnification (minimum 3.5x to 4.5x) is absolute standard of care, given the diminutive size of pediatric neurovascular structures and the necessity for meticulous soft-tissue handling.
Preparation of the surgical field must include the entire upper extremity up to the axilla, allowing for the harvest of proximal tendon grafts or the mobilization of regional flaps if required. A sterile marking pen is used to delineate all planned incisions, Z-plasty limbs, and flap designs prior to exsanguination and tourniquet inflation. This ensures that the natural resting tension of the skin is accurately represented in the markings. Intraoperative fluoroscopy (mini-C-arm) must be draped and readily available for the assessment of osteotomy alignment, joint reduction, and K-wire trajectory. The surgeon must also ensure the availability of fine pediatric hand instruments, including micro-osteotomes, 0.028-inch and 0.035-inch Kirschner wires, and fine non-absorbable monofilament sutures for matrix and nerve repair.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention for thumb disproportion demands an extraordinary level of precision. The tissues in pediatric congenital hands are diminutive, anomalous, and unforgiving of rough handling. Strict adherence to atraumatic soft-tissue techniques, preservation of the subdermal vascular plexus, and precise osteosynthesis are required to prevent catastrophic ischemic complications or growth arrest. The surgical approach is dictated by the specific pathology, whether it be the osseous reduction of macrodactyly or the complex soft-tissue reconstruction of the adducted, hypoplastic thumb.
The Millesi Procedure for Thumb Shortening
The Millesi technique is the gold standard for reducing both the osseous length and the soft-tissue envelope of the overgrown thumb while preserving the critical nail complex and tactile sensibility. Following exsanguination and tourniquet inflation, the procedure begins with the excision of the distal half of the nail plate, the underlying nail matrix, and the distal phalangeal tuft. This immediately reduces the overall width and length of the distal segment. A dorsal longitudinal incision is then created overlying the proximal and distal phalanges. The skin flaps are carefully elevated, strictly protecting the dorsal sensory branches of the radial nerve and the extensor pollicis longus (EPL) insertion.
The middle third of the distal phalanx is resected using an oscillating micro-saw or fine bone-cutting forceps, along with the middle third of the overlying nail and matrix. Attention is then directed to the proximal phalanx, where parallel oblique osteotomies are performed to excise its middle third. The oblique geometry of these cuts is critical; it significantly increases the surface area for cancellous bony healing compared to standard transverse osteotomies and allows for minor rotational adjustments. The two remaining longitudinal components of the distal phalanx are reduced, compressed, and rigidly fixed using a transverse 0.028-inch or 0.035-inch Kirschner wire.
The distal and proximal fragments of the proximal phalanx are then reduced into their new, shortened configuration. This osteotomy is secured with a single or crossed oblique K-wire construct, ensuring no step-off at the articular surfaces. Closure is performed by meticulously approximating the skin edges. The remaining nail matrix must be repaired with fine absorbable sutures (e.g., 6-0 chromic gut) under loupe magnification. Precise matrix repair is critical to prevent postoperative nail dystrophy, split nail deformity, or the dreaded hook-nail. The K-wires are left protruding through the skin, bent, and capped to facilitate easy removal in the outpatient clinic once radiographic healing is confirmed.
First Web Space Deepening and Contracture Release
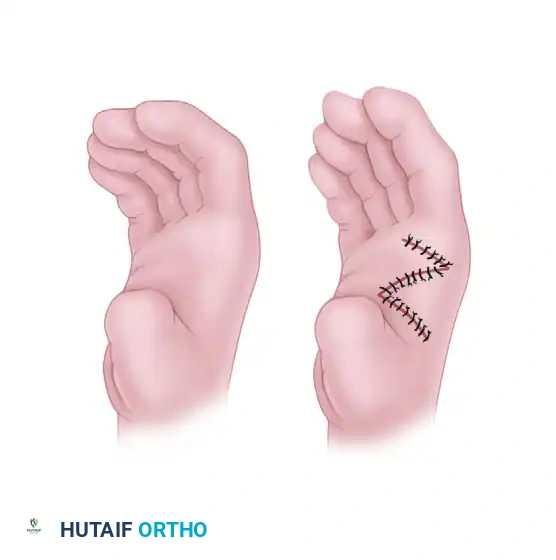
For the adducted thumb, the release of the first web space contracture is the obligatory first step; no tendon transfer can function against a fixed static contracture. For mild to moderate contractures, local tissue rearrangement via Z-plasty is utilized.
FIGURE 79-65: Simple Z-plasty of the thumb web. A, Incisions designed along the contracted web. B, Closure after reversal and transposition of the flaps to deepen the web space.
The standard two-limb Z-plasty or a four-limb (broad-based) Z-plasty is designed along the contracted web. The flaps must be elevated with a robust layer of subcutaneous fat to preserve the subdermal plexus. Deep to the skin, the deep investing fascia of the adductor pollicis and the first dorsal interosseous muscle must be completely released. Occasionally, the origin of the first dorsal interosseous must be partially recessed from the first metacarpal to achieve adequate palmar abduction.
For severe contractures where local tissue is insufficient, regional flaps are required. The Littler and Cooley pedicled abdominal flap provides a massive influx of healthy, vascularized tissue to reconstruct the soft tissue envelope of the severely adducted thumb.
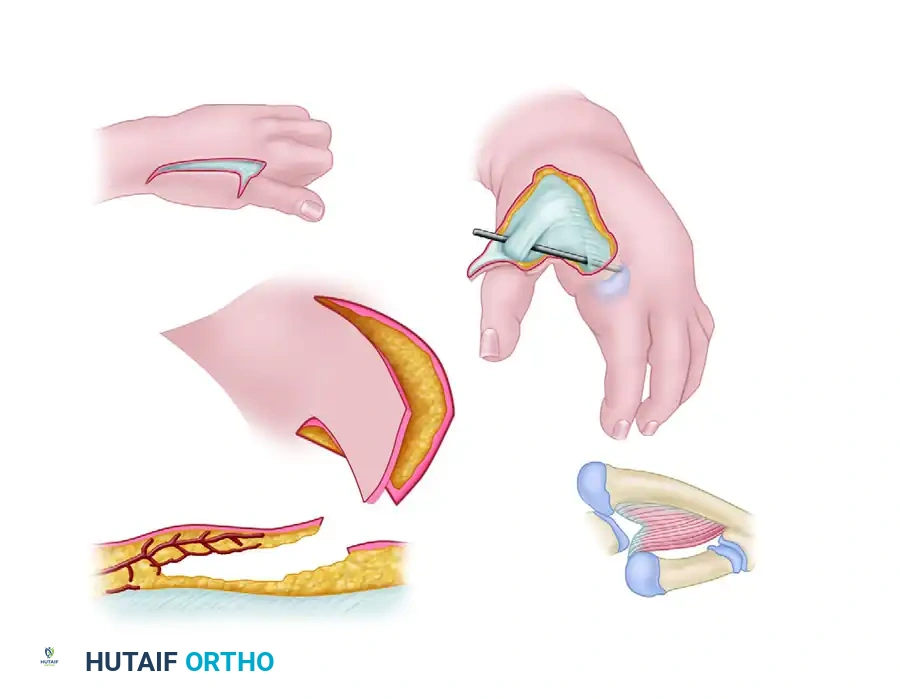
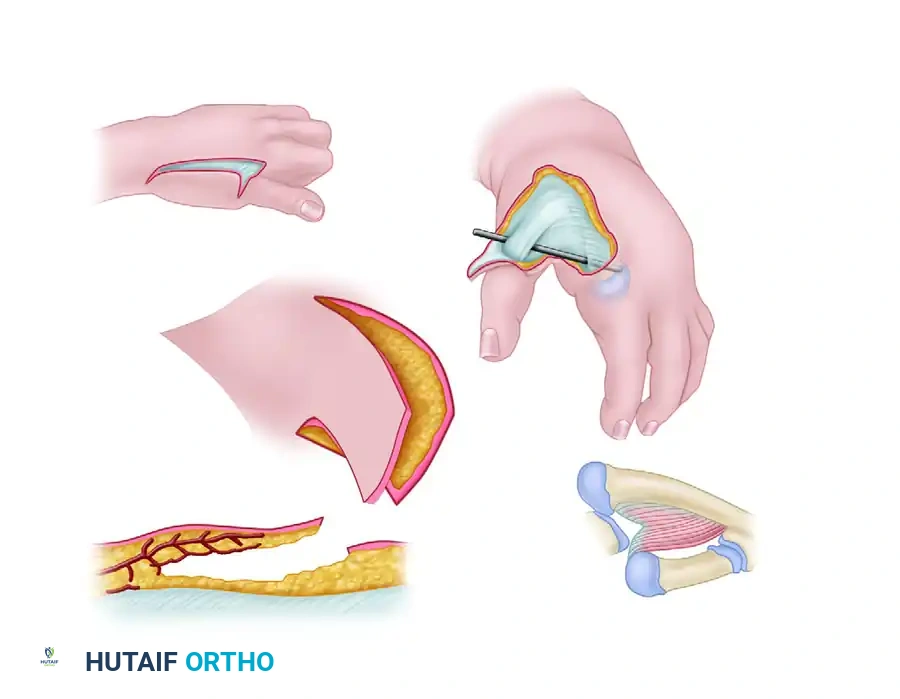
FIGURE 79-63: Littler correction of severe adduction contracture of the thumb utilizing an abdominal flap based on the thoracoepigastric vessels. Note the relationship to the extensor pollicis longus and the adduction-abduction axis.
Alternatively, pedicled distally based radial forearm or dorsal interosseous flaps can be utilized to provide robust, pliable tissue to the deficient web space without the need for a staged abdominal attachment.
Opponensplasty Techniques
Following web space release, dynamic opposition is restored. The Flexor Digitorum Superficialis (FDS) transfer is a workhorse procedure. The FDS of the ring finger is harvested via a transverse incision at the proximal interphalangeal joint crease. It is withdrawn into the palm and routed subcutaneously toward the thumb.
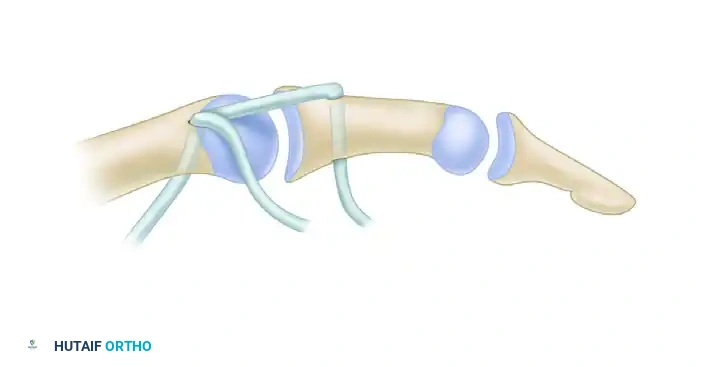
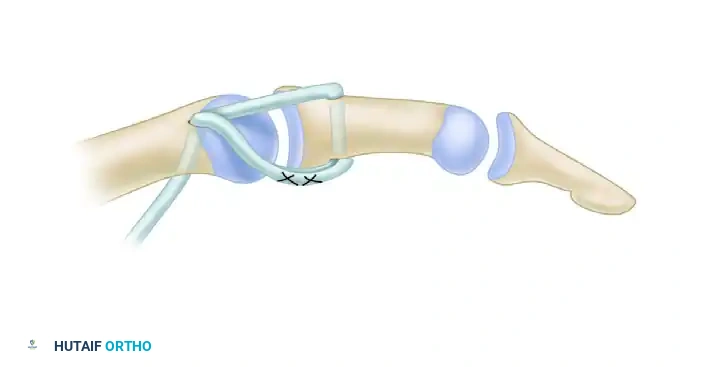
FIGURE 79-64: Flexor digitorum sublimis (superficialis) opposition transfer combined with collateral ligament repair. The tendon is routed to provide an optimal vector for palmar abduction and pronation.
To replicate the vector of the APB, the FDS tendon must be routed around a pulley—often constructed from a slip of the flexor carpi ulnaris (FCU) or the palmar aponeurosis near the pisiform. The tendon is then tunneled subcutaneously to the radial aspect of the thumb MCP joint. It is woven into the insertion of the APB, the dorsal capsule, or directly into the base of the proximal phalanx to provide both palmar abduction and pronation.
The Huber procedure (Abductor Digiti Minimi transfer) is an excellent alternative, particularly when the thenar eminence is severely flattened. The ADM is detached from its insertion on the proximal phalanx of the small finger, carefully mobilized on its neurovascular pedicle (preserving the ulnar artery and nerve branches), and folded over 180 degrees to reach the thumb. It is tunneled subcutaneously across the palm and inserted into the APB insertion. This transfer not only restores opposition but provides excellent aesthetic bulk to the deficient thenar cone.
Metacarpophalangeal Joint Stabilization
In the hypoplastic thumb, the MCP joint is frequently unstable due to profound laxity of the ulnar collateral ligament (UCL). Stabilization must be performed concurrently with the opponensplasty. Through a dorsal-ulnar incision over the MCP joint, the attenuated UCL is identified. If sufficient tissue exists, it is imbricated and advanced distally into the base of the proximal phalanx using a micro-suture anchor or transosseous sutures.
If the local tissue is entirely deficient, the joint must be reconstructed. This is often achieved by utilizing a slip of the transferred FDS tendon, routing it through a drill hole in the metacarpal head and securing it to the proximal phalanx. In older children or adolescents with intractable instability and early arthrosis, an MCP joint chondrodesis (fusion) is performed. The articular cartilage is denuded, the joint is positioned in 15 degrees of flexion and slight pronation, and rigid fixation is achieved with crossed K-wires or a miniature compression screw, providing a stable post for pinch.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction of thumb disproportion is fraught with potential complications, largely due to the anomalous anatomy, deficient soft-tissue envelopes, and the inherent challenges of pediatric compliance with postoperative immobilization. The surgeon must maintain a high index of suspicion for early postoperative complications, particularly vascular compromise. Flap necrosis following web space deepening or abdominal flap coverage is a devastating complication that can lead to severe recurrent contracture and deep infection. This is typically caused by excessive tension on the Z-plasty limbs or unrecognized kinking of a pedicled flap's vascular supply.
Tendon transfer failure is another significant concern. An opponensplasty may stretch out over time, particularly if the initial web space release was inadequate or if the patient fails to comply with postoperative splinting. Alternatively, if the MCP joint was not adequately stabilized prior to the transfer, the dynamic force of the new tendon will cause progressive radial subluxation of the proximal phalanx, leading to a profound Z-collapse deformity. In cases of osseous shortening (Millesi procedure), complications include nonunion of the phalangeal osteotomies, K-wire migration or pin tract infection, and severe nail dystrophy resulting from imprecise matrix repair.
When complications arise, rapid identification and aggressive salvage management are required. A failed opponensplasty may necessitate a secondary transfer using a different donor motor (e.g., EIP to APB) combined with a revision web space release. A Z-collapse deformity mandates immediate surgical intervention to fuse the MCP joint (arthrodesis) to restore a stable longitudinal axis. In the event of complete failure of reconstruction in a hypoplastic thumb—resulting in a stiff, insensate, and non-functional appendage—the ultimate salvage procedure remains ray amputation and formal index finger pollicization.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Flap/Z-plasty Necrosis | 5% - 10% | Ensure broad-based flaps; avoid tension; preserve subdermal plexus; adequate release of deep fascia. | Local wound care; secondary healing; full-thickness skin grafting; regional pedicled flap if severe. |
| Opponensplasty Stretching/Failure | 10% - 15% | Over-correct tension during transfer; rigid postoperative immobilization; adequate prior web release. | Revision tendon transfer (e.g., EIP or FPL if available); tenodesis. |
| MCP Joint Z-Collapse | 15% - 20% | Routinely stabilize UCL/RCL prior to or concurrent with opponensplasty; avoid excessive transfer tension. | MCP joint chondrodesis/arthrodesis to provide a rigid post. |
| Osteotomy Nonunion (Millesi) | < 5% | Use oblique osteotomies for greater surface area; rigid K-wire fixation; avoid thermal necrosis with saw. | Revision osteosynthesis with autologous bone grafting; prolonged immobilization. |
| Severe Nail Dystrophy | 10% - 25% | Meticulous repair of the nail matrix under loupe magnification; avoid over-resection of proximal matrix. | Nail bed reconstruction; ablation of the nail matrix if cosmetically unacceptable and painful. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of thumb reconstruction is inextricably linked to the quality of postoperative rehabilitation. The surgical procedure merely sets the anatomical stage; it is the rigorous, phased therapy protocol that dictates functional recovery. In the pediatric population, this requires intensive collaboration between the orthopedic surgeon, a specialized pediatric hand therapist, and the patient's parents. The rehabilitation protocol is generally divided into three distinct phases: immobilization, active re-education, and dynamic strengthening/stretching.
Phase I: Strict Immobilization (Weeks 0 - 4)
Immediately following surgery, the hand is placed in a bulky, well-padded thumb spica cast. For opponensplasties and web space releases, the thumb must be immobilized in maximum palmar abduction and opposition. The wrist is typically positioned in 15 to 20 degrees of flexion to remove tension from the FDS or ADM transfer. K-wires utilized for MCP stabilization or Millesi osteotomies are left in place beneath the cast. During this phase, the primary goals are the protection of the surgical repairs, mitigation of edema, and prevention of K-wire migration. Absolute compliance is mandatory; parents are instructed on cast care and the signs of neurovascular compromise.
Phase II: Active Cortical Re-education (Weeks 4 - 8)
At approximately 4 weeks postoperatively, the cast is removed. Radiographs are obtained to confirm osteotomy healing or joint stabilization, and K-wires are pulled in the clinic. A custom thermoplastic short opponens splint is fabricated, maintaining the thumb in abduction. This splint is worn at all times except during therapy sessions. The focus now shifts to active range of motion (AROM) and cortical re-education of the transferred muscle. For an FDS transfer, the child is taught to actively flex the donor ring finger, which now translates into thumb opposition. In pediatric patients, this is achieved through play therapy (e.g., pinching large blocks or grasping toys). Passive motion of the transferred tendon is strictly avoided to prevent stretching of the repair.
Phase III: Dynamic Stretching and Strengthening (Weeks 8 - 24+)
By the 8th postoperative week, the tendon transfer is considered robustly healed. The daytime splint is gradually weaned, though night splinting in wide palmar abduction is continued for up to 6 months to prevent recurrent contracture of the first web space Z-plasties. Therapy progresses to include passive stretching of the web space and progressive resistive exercises to build pinch and grasp strength. The therapist monitors for any signs of MCP joint instability or loss of opposition vector. Long-term follow-up is essential, as the child's growth spurts can occasionally lead to recurrent contractures or relative shortening of the transferred musculotendinous units, necessitating secondary releases.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for thumb hypoplasia and disproportion is chronicled through several landmark anatomical and clinical studies. The modern algorithmic approach is fundamentally based on the work of Paul R. Manske, whose classification system (Manske and McCarroll, 1992) revolutionized the decision-making process. By identifying the stability of the CMC joint as the absolute pivot point between reconstruction (Type IIIA) and pollicization (Type IIIB), Manske provided a reliable, reproducible framework that remains the global standard of care. Attempts to deviate from this guideline—specifically, attempting local reconstruction on a Type IIIB thumb—have been universally shown in long-term follow-up studies to yield poor functional results.
The techniques for restoring opposition have similarly evolved. Huber's original description of the abductor digiti minimi transfer in 1921 was a conceptual breakthrough, later popularized and refined by Littler and Cooley in the 1960s. Littler's emphasis on the precise anatomical vector required for true opposition—
