Surgical Management of Fixed Deformities and Charcot Arthropathy

Key Takeaway
Fixed deformities in the diabetic foot, combined with peripheral neuropathy, create high-pressure focal points that inevitably lead to ulceration. Surgical intervention, including Achilles tendon lengthening, metatarsal head resection, and corrective arthrodesis, is often required when conservative off-loading fails. In cases of Charcot neuropathic arthropathy, early recognition and total contact casting are paramount to prevent catastrophic midfoot collapse and preserve a plantigrade, ulcer-free foot.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of the diabetic foot, particularly in the context of fixed deformities and neuropathic (Charcot) osteoarthropathy, represents one of the most formidable challenges in modern orthopedic surgery. The global prevalence of diabetes mellitus has reached epidemic proportions, and the sequelae of this systemic disease manifest profoundly in the lower extremities. An essential, yet frequently underestimated, element in the treatment of diabetic forefoot ulceration and midfoot collapse is the presence of an underlying, rigid biomechanical fault. It is exceedingly difficult—and often impossible—to maintain long-term soft-tissue healing if the structural bony deformity remains uncorrected, even when initial epithelialization is achieved through rigorous off-loading, total contact casting, or advanced wound care modalities.
The pathophysiology of diabetic foot deformities is inextricably linked to the triad of neuropathy: motor, sensory, and autonomic. Motor neuropathy selectively denervates the intrinsic musculature of the foot, leading to an imbalance between the powerful extrinsic flexors and extensors and the weakened intrinsic stabilizers (lumbricals and interossei). This denervation results in the classic intrinsic-minus foot posture, characterized by hyperextension at the metatarsophalangeal (MTP) joints and flexion at the proximal and distal interphalangeal joints. Consequently, the protective plantar fat pad is drawn distally into the sulcus, leaving the metatarsal heads prominent, denuded of their natural cushioning, and highly vulnerable to vertical and shear forces during the terminal stance phase of gait.

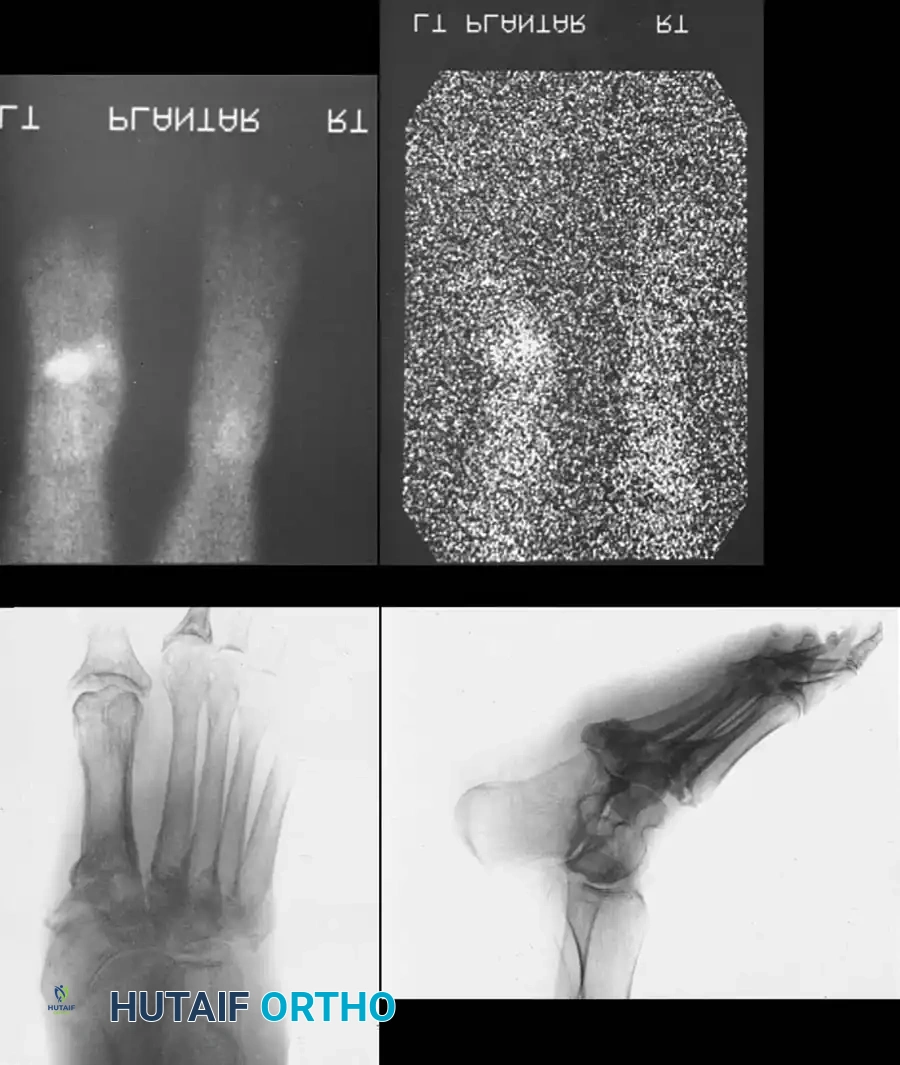
Concurrently, diabetic autonomic neuropathy leads to an "autosympathectomized" extremity. The profound loss of sympathetic tone results in a complete lack of sweating (anhidrosis), leaving the cutaneous envelope dry, scaly, and highly prone to fissuring. Furthermore, this sympathetic denervation causes a loss of precapillary sphincter control, leading to profound arteriovenous shunting and a localized hyperemic state. This hyperemia, as described by the neurovascular (French) theory of Charcot arthropathy, causes localized, aggressive osteopenia that weakens the structural integrity of the osseous architecture.
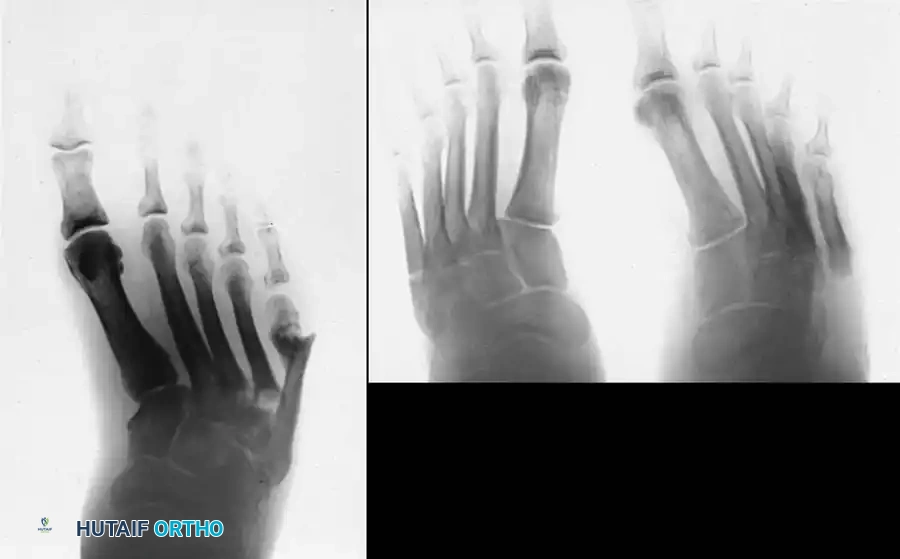
When this osteopenic bone is subjected to repetitive, unrecognized microtrauma due to profound somatosensory neuropathy (the neurotraumatic or German theory), the result is a catastrophic cycle of microfractures, ligamentous attenuation, and eventual joint collapse. This neuropathic osteoarthropathy (Charcot arthropathy) most frequently affects the midfoot (Lisfranc and Chopart joints), leading to the classic rocker-bottom deformity. The epidemiological burden of these fixed deformities is staggering, with a direct correlation between structural collapse, recalcitrant ulceration, deep space infection, osteomyelitis, and major lower extremity amputation.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of foot and ankle biomechanics is paramount for the orthopedic surgeon attempting to reconstruct the diabetic foot. The foot functions as a complex, dynamic adapter during the initial stance phase and transitions into a rigid lever arm for propulsion during terminal stance. This transition is heavily dependent on the integrity of the plantar fascia, the windlass mechanism, and the structural keystone of the midfoot arch.
In the forefoot, the stability of the MTP joints is governed by the plantar plate, the collateral ligaments, and the dynamic balance between the extrinsic and intrinsic musculature. The lumbricals, which originate from the flexor digitorum longus tendons, normally flex the MTP joints and extend the interphalangeal joints. When motor neuropathy causes lumbrical atrophy, the unopposed action of the extensor digitorum longus (EDL) hyperextends the MTP joint, while the flexor digitorum longus (FDL) flexes the PIP and DIP joints, creating a rigid claw toe. This fixed deformity exponentially increases peak plantar pressures beneath the metatarsal heads.


The midfoot relies on the osseous architecture of the Roman arch, where the base of the second metatarsal is recessed between the medial and lateral cuneiforms, acting as the keystone. The Lisfranc ligament complex, particularly the stout interosseous ligament spanning from the medial cuneiform to the base of the second metatarsal, provides critical stability. In Charcot arthropathy (Brodsky Type 1), this ligamentous complex undergoes catastrophic failure. The forefoot typically abducts and subluxates laterally, driven by the unopposed pull of the peroneus brevis. This subluxation forces the medial cuneiform and the base of the first metatarsal plantarward, creating a massive bony prominence that inevitably ulcerates.
Arguably the most critical biomechanical fault in the diabetic foot is the presence of an equinus contracture. A tight gastrocnemius-soleus complex forces the patient to "vault" over the forefoot during the stance phase of gait. This vaulting mechanism prevents normal ankle dorsiflexion, prematurely loading the forefoot and exponentially increasing peak plantar pressures beneath the metatarsal heads and the midfoot apex. The Silfverskiöld test is essential to differentiate between isolated gastrocnemius contracture and a combined gastrocnemius-soleus (Achilles) contracture, dictating whether a gastrocnemius recession or a percutaneous Achilles tendon lengthening (TAL) is required.



Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in fixed diabetic deformities and Charcot arthropathy is highly nuanced. Surgery in this patient population is fraught with severe complications, including hardware failure, nonunion, deep infection, and amputation. Therefore, surgical indications must be strictly defined and weighed against the patient's vascular status, glycemic control, and overall physiological reserve.
The primary indication for surgery is the presence of a severe, unbraceable deformity that has led to, or is at imminent risk of causing, recalcitrant ulceration. In the setting of Charcot arthropathy, the Eichenholz staging system dictates the timing of intervention. Historically, surgery was strictly contraindicated during the acute inflammatory phase (Stage 0 and I) due to the hyperemic, osteopenic nature of the bone, which precludes rigid fixation. However, modern paradigms have shifted. If a frank dislocation at the tarsometatarsal joint is identified early in Stage I—before extensive bony fragmentation and soft-tissue contracture occur—limited open reduction and primary arthrodesis (or percutaneous beaming) may be indicated to prevent inevitable rocker-bottom collapse.
Surgical Decision Matrix
| Parameter | Indications for Surgical Reconstruction | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Vascular Status | ABI > 0.9, TcPO2 > 40 mmHg, palpable pulses or biphasic Doppler signals. | Severe PAD (ABI < 0.5, TcPO2 < 20 mmHg) without prior revascularization. | Moderate PAD requiring multidisciplinary vascular optimization prior to orthopedic intervention. |
| Infectious Status | Chronic, non-infected ulceration failing off-loading; localized osteomyelitis amenable to en bloc resection. | Active, systemic sepsis; uncontrolled necrotizing fasciitis; unsalvageable pan-osteomyelitis. | Active superficial cellulitis (must be treated with IV antibiotics prior to definitive reconstruction). |
| Charcot Stage | Eichenholz Stage III (Consolidation) with unbraceable deformity; Early Stage I frank dislocation. | Eichenholz Stage II (Coalescence) with massive ongoing fragmentation and active hyperemia. | Eichenholz Stage 0/I without frank dislocation (best managed with Total Contact Casting). |
| Medical Optimization | HbA1c < 8.0%, optimized nutrition (Albumin > 3.5 g/dL), compliant patient. | Severe medical non-compliance; profound malnutrition; medically unstable for anesthesia. | HbA1c > 9.0% (requires endocrinology optimization to mitigate post-operative infection risk). |


Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful diabetic foot reconstruction. The diagnostic workup must be exhaustive. Standard weight-bearing radiographs (anteroposterior, lateral, and oblique views) are mandatory to assess the degree of collapse, the presence of fixed subluxations, and the Meary's angle (talo-first metatarsal angle), which is typically severely intersected in a rocker-bottom foot.
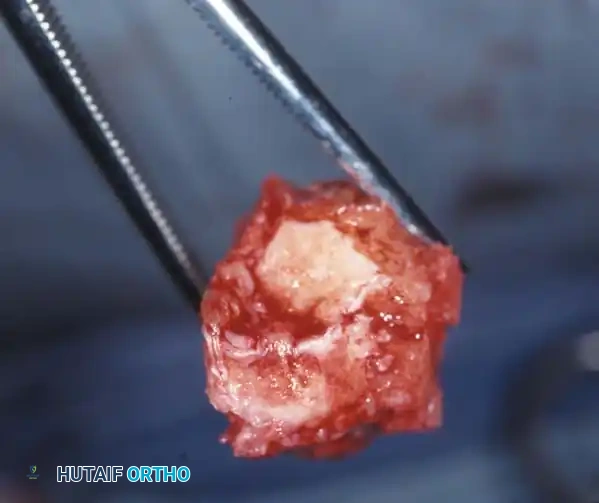
Advanced imaging is routinely required. A computed tomography (CT) scan with 3D reconstructions is invaluable for mapping the precise architecture of the fragmentation, identifying viable bone stock for hardware purchase, and planning osteotomy trajectories. Magnetic resonance imaging (MRI) is the gold standard for differentiating between acute Charcot osteoarthropathy (characterized by diffuse bone marrow edema and periarticular fluid) and underlying osteomyelitis (characterized by focal marrow replacement, cortical destruction, and sinus tract formation). In equivocal cases, Indium-111 labeled white blood cell scans combined with Technetium-99m bone marrow scans may be required to definitively diagnose osteomyelitis in the setting of Charcot.
Vascular clearance is a non-negotiable prerequisite. Non-invasive arterial studies, including Ankle-Brachial Indices (ABI), Toe-Brachial Indices (TBI), and transcutaneous oxygen tension (TcPO2), must be obtained. A TcPO2 of less than 30 mmHg severely compromises wound healing and necessitates vascular surgery consultation for potential endovascular angioplasty or open bypass grafting prior to any orthopedic intervention.


Patient positioning depends heavily on the planned procedure. For forefoot reconstructions and medial column Charcot fusions, the patient is placed supine with a bump under the ipsilateral hip to internally rotate the leg to a neutral position. For lateral column procedures, calcaneal osteotomies, or complex hindfoot reconstructions, a lateral decubitus position may be preferred. The use of a pneumatic thigh tourniquet is highly controversial in the diabetic population. In patients with significant peripheral arterial disease or heavily calcified vessels (Mönckeberg's arteriosclerosis), tourniquet inflation can cause catastrophic intimal sheer, leading to acute arterial thrombosis and subsequent limb loss. If a tourniquet is used, it should be inflated to the lowest effective pressure and for the shortest possible duration.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of the diabetic foot ranges from prophylactic soft-tissue releases to massive, limb-salvaging osseous reconstructions. The overarching goal is to create a plantigrade, stable, and braceable foot that is free of prominent pressure asperities.
Forefoot Deformity Correction
When conservative measures fail, surgical correction of fixed forefoot deformities is mandated to prevent recurrent ulceration and deep space infection. For fixed claw toe deformities, a stepwise approach is utilized. A dorsal longitudinal incision is made over the affected MTP and PIP joints. An extensor tendon lengthening (either a Z-lengthening or a simple tenotomy) is performed. A dorsal capsulotomy of the MTP joint is executed, releasing the collateral ligaments to allow the proximal phalanx to reduce plantarly. If the PIP joint deformity is fixed, a DuVries arthroplasty (resection of the distal condyles of the proximal phalanx) or a formal PIP arthrodesis is performed, stabilized with a smooth Kirschner wire driven retrogradely into the metatarsal.
For recalcitrant plantar ulcerations beneath the metatarsal heads, a metatarsal head resection may be necessary. In severe cases with multiple adjacent ulcers, a complete pan-metatarsal head resection through a dorsal approach is highly effective in relieving plantar pressure. Fixed flexion deformities of the hallux interphalangeal joint, which create massive pressure at the distal tip of the toe, are treated with an interphalangeal arthrodesis combined with an extensor hallucis longus (EHL) lengthening, utilizing a robust 4.0mm or 4.5mm cannulated screw for rigid compression.


Midfoot and Hindfoot Charcot Reconstruction
The reconstruction of the Charcot midfoot requires adherence to the principles of "superconstructs," as popularized by Sammarco. These principles dictate that fixation must extend far beyond the zone of injury, utilizing the strongest hardware possible (often oversized for the anatomical region), maximizing hardware surface area, and achieving rigid arthrodesis of both affected and adjacent unaffected joints.
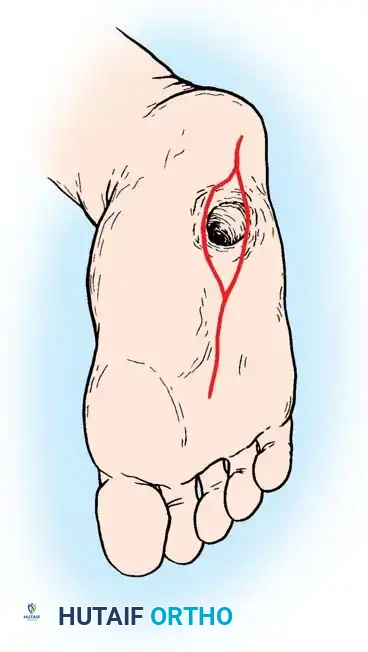
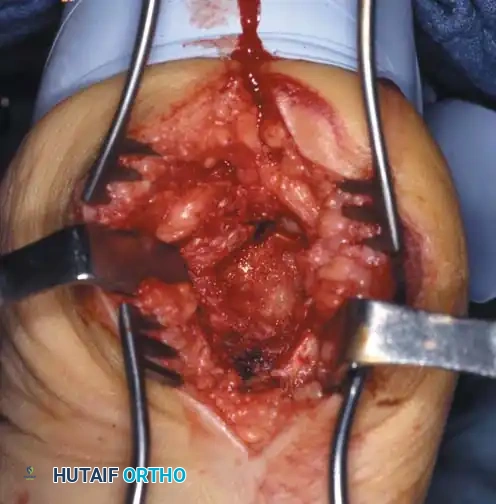
For the classic abducted forefoot (Type 1 Charcot), a medial utility incision is utilized, extending from the navicular tuberosity to the mid-shaft of the first metatarsal. The medial neurovascular bundle is carefully protected. The destroyed, hypertrophic bone of the tarsometatarsal joints is radically resected using an oscillating saw. It is critical to resect enough bone to allow for tension-free reduction of the deformity; attempting to lever the foot straight against contracted soft tissues will inevitably lead to hardware failure. The sclerotic bone ends are meticulously prepared with osteotomes and a high-speed burr ("fish-scaling") to expose bleeding subchondral bone.



Once the medial column is aligned (restoring Meary's line), fixation is achieved using massive intramedullary beaming screws. A 6.5mm or 7.3mm solid, fully threaded midfoot fusion bolt is driven antegrade from the base of the first metatarsal, across the cuneiforms and navicular, and anchored deeply into the body of the talus. This axial beaming neutralizes bending moments. This construct is then augmented with a stout, low-profile medial column locking plate to provide rigid, multi-planar stability.
For the adducted forefoot, which is notoriously difficult to treat, comprehensive realignment of the lateral column is required. Simply excising the prominent fifth metatarsal base is a critical error, as it transfers the pressure apex proximally to the cuboid. A lateral approach is utilized, the calcaneocuboid and cuboid-metatarsal joints are resected, and the lateral column is shortened and rigidly fixed with a combination of beaming screws and lateral locking plates.
Achilles Tendon Lengthening Techniques
No Charcot reconstruction or forefoot ulcer off-loading is complete without addressing the equinus contracture. A percutaneous Achilles tendon lengthening (TAL) is arguably the single most effective intervention in diabetic foot surgery. Using the Hoke technique, three percutaneous hemisections are made: the distal cut is made medially (to preserve the sural nerve laterally), the middle cut is made laterally, and the proximal cut is made medially. The ankle is then forcibly dorsiflexed to neutral, allowing the tendon fibers to slide and lengthen. Care must be taken not to over-lengthen, which would result in a devastating calcaneal gait and subsequent heel ulceration.

Complications, Incidence Rates, and Salvage Management
Surgical intervention in the diabetic, neuropathic foot carries one of the highest complication rates in orthopedic surgery. The host bone is profoundly osteopenic, the soft-tissue envelope is compromised by microvascular disease, and the patient's lack of protective sensation often leads to unrecognized, premature weight-bearing, which is catastrophic for rigid internal fixation.
Hardware failure (breakage, pull-out, or migration) is exceedingly common due to the massive cyclical loads placed on the superconstruct in the absence of proprioceptive feedback. Nonunion and pseudoarthrosis rates are significantly higher than in the non-diabetic population. While a stable, fibrous pseudoarthrosis may be clinically acceptable if the foot remains plantigrade and ulcer-free, an unstable nonunion will rapidly progress to recurrent deformity.
Complication Profile and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiologic Etiology | Salvage Management Strategy |
|---|---|---|---|
| Hardware Failure / Pull-out | 15% - 35% | Osteopenic host bone; premature weight-bearing due to neuropathy; inadequate initial fixation. | Revision open reduction internal fixation (ORIF) with larger diameter beaming screws; transition to circular external fixation (Ilizarov). |
| Surgical Site Infection (SSI) | 10% - 25% | Poor glycemic control (HbA1c > 8.0%); compromised microvascular perfusion; prolonged operative time. | Aggressive serial surgical debridement; hardware removal if stability is compromised; culture-directed intravenous antibiotic therapy; negative pressure wound therapy. |
| Symptomatic Nonunion | 10% - 20% | Avascularity of sclerotic bone ends; inadequate mechanical compression; smoking. | Revision arthrodesis utilizing autologous iliac crest bone graft (ICBG) or orthobiologics (rhBMP-2); prolonged immobilization. |
| Recurrent Ulceration | 20% - 40% | Failure to correct equinus contracture (missed TAL); transfer lesions to adjacent metatarsals; progressive midfoot collapse. | Exostectomy of new prominent asperities; revision TAL; custom-molded Charcot Restraint Orthotic Walker (CROW). |
| Major Amputation (BKA) | 5% - 15% | Unsalvageable deep space infection; ascending necrotizing fasciitis; catastrophic failure of reconstruction with severe PAD. | Below-knee amputation (BKA) utilizing long posterior flap (Burgess technique) to optimize prosthetic fitting and preserve mobility. |
When internal fixation fails catastrophically or in the setting of active osteomyelitis where internal hardware is contraindicated, the ultimate salvage procedure is the application of a circular external fixator (Ilizarov or Taylor Spatial Frame). Tensioned fine wires provide rigid stability even in severely osteopenic bone, allowing for gradual deformity correction, compression across arthrodesis sites, and simultaneous access for advanced soft-tissue wound care.


Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following diabetic foot reconstruction is arguably as critical as the surgical execution itself. The timeline for healing in the neuropathic foot is significantly protracted, often requiring two to three times the duration of immobilization compared to a neuro-intact patient.
Phase I: Maximum Protection (Weeks 0 to 6)
Immediately post-operatively, the patient is placed in a well-padded, short-leg splint and maintained in a strict, absolutely non-weight-bearing (NWB) status. Elevation is paramount to mitigate the profound post-operative edema characteristic of the hyperemic Charcot foot. At 10 to 14 days, sutures are removed. If the incisions are fully epithelialized, the patient is transitioned to a Total Contact Cast (TCC). The TCC is the gold standard for off-loading, as it distributes weight evenly across the entire plantar surface and lower leg, preventing shear forces. During this highly edematous phase, the cast must be changed every 1 to 2 weeks; as swelling rapidly subsides, a loose cast will cause pistoning, leading to devastating iatrogenic shear ulcers.
Phase II: Protected Consolidation (Weeks 6 to 16+)
The patient remains strictly non-weight-bearing in a TCC or a locked, rigid pneumatic fracture boot. Serial radiographs are obtained every 4 weeks to assess for hardware integrity and the progression of osseous consolidation across the arthrodesis sites. It is critical to understand that radiographic consolidation in a Charcot reconstruction routinely takes 4 to 6 months, with proximal joint involvement (hindfoot and ankle) requiring the longest durations.
Phase III: Progressive Loading and Bracing (Months 4 to 12)
Once definitive radiographic consolidation is confirmed and clinical signs of inflammation (erythema, edema, thermal gradients) have completely resolved, the patient may begin a meticulously supervised, progressive weight-bearing protocol. This must never be done in standard footwear. The patient is transitioned to a custom-molded Charcot Restraint Orthotic Walker (CROW) or a patellar tendon-bearing (PTB) brace. The CROW boot encapsulates the entire foot and lower leg, providing total contact and an unyielding rocker-bottom sole to facilitate gait without bending the midfoot.
Phase IV: Long-Term Maintenance
For the remainder of the patient's life, they must utilize custom-molded extra-depth diabetic shoes with rigid rocker-bottom soles and plastazote inserts. Routine podiatric or orthopedic follow-up every 3 to 4 months is mandatory for callus debridement and surveillance of the contralateral limb, which is at an exceptionally high risk for developing a subsequent Charcot event.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for fixed deformities and Charcot arthropathy is heavily grounded in landmark orthopedic literature. The foundational staging system proposed by Eichenholz in 1966 remains the cornerstone of clinical assessment, detailing the progression from acute fragmentation to eventual consolidation. Brodsky and Trepman's anatomical classification further refined the surgical approach by delineating the distinct biomechanical challenges of the midfoot (Type 1) versus the hindfoot (Type 2).
Historically, the prevailing dogma strictly prohibited surgical intervention during the acute, inflammatory phase of Charcot arthropathy. However, contemporary literature, spearheaded by authors such as Wukich, Armstrong, and Pinzur, has challenged this paradigm. Recent studies advocate for early, limited internal fixation or percutaneous beaming in Stage I Charcot when a frank dislocation is present, arguing that preventing the anatomical collapse is superior to attempting a massive reconstruction of a rigidly deformed, rocker-bottom foot in Stage III.
The concept of the "superconstruct" was definitively codified by Sammarco, establishing the biomechanical necessity of extending fixation beyond the traditional zones of injury and utilizing oversized, rigid hardware to counteract the unique destructive forces of the neuropathic foot. Furthermore, the critical importance of the Achilles tendon lengthening (TAL) in off-loading the forefoot and midfoot has been unequivocally validated by numerous prospective trials, demonstrating a precipitous drop in ulcer recurrence rates when TAL is combined with appropriate orthotic management.
In conclusion, the surgical management of fixed deformities and Charcot arthropathy demands a profound understanding of biomechanics, meticulous pre-operative optimization, rigid adherence to specialized fixation principles, and an exhaustively supervised post-operative rehabilitation protocol. Only through this comprehensive, multidisciplinary approach can the orthopedic surgeon hope to achieve a stable, plantigrade limb and prevent the devastating endpoint of major lower extremity amputation.
