Volar Approach: Optimal Exposure for the Volar aspect of the Distal Radius

Key Takeaway
This article provides essential research regarding Volar Approach: Optimal Exposure for the Volar aspect of the Distal Radius. The volar approach to the distal radius is a surgical technique primarily used for treating distal radial fractures, especially with locking plates. It provides excellent exposure of the volar aspect of the distal radius. This approach is also utilized for bone grafting, osteotomies, or radial styloid excision by developing a plane between the radial artery and flexor carpi radialis.
Comprehensive Introduction and Patho-Epidemiology
The volar approach to the distal radius has fundamentally revolutionized the operative management of distal radius fractures and associated wrist pathology. Historically, dorsal approaches were favored due to the dorsal displacement typical of Colles-type fractures; however, the advent of anatomically contoured, fixed-angle volar locking plates initiated a paradigm shift in orthopedic trauma surgery. The volar surface of the distal radius offers a flat, broad cortical expanse that is biomechanically ideal for plate application, providing a robust buttress against the deforming forces of the forearm musculature. Furthermore, the volar approach capitalizes on a thick envelope of soft tissue—specifically the pronator quadratus muscle—which serves as an excellent biological barrier between the orthopedic hardware and the delicate flexor tendons.
Epidemiologically, distal radius fractures represent approximately one-sixth of all fractures evaluated in emergency departments, exhibiting a classic bimodal distribution. High-energy trauma mechanisms, such as motor vehicle collisions or falls from significant heights, typically affect younger, predominantly male demographics, resulting in complex, intra-articular, and highly comminuted fracture patterns. Conversely, low-energy falls from a standing height disproportionately affect the elderly, osteopenic, or osteoporotic female population, commonly resulting in extra-articular bending fractures. The volar approach provides unparalleled access to address both of these disparate patho-anatomical entities, allowing for direct visualization of the volar cortex, restoration of volar tilt, and indirect reduction of the dorsal cortex through ligamentotaxis and subchondral support.
Beyond acute fracture management, the versatility of the volar approach extends to a myriad of reconstructive procedures. It is the workhorse exposure for corrective osteotomies of distal radius malunions, where precise restoration of radial inclination, volar tilt, and ulnar variance is paramount. The approach is equally efficacious for the application of vascularized or non-vascularized bone grafts in the setting of nonunions, excision of symptomatic radial styloid pathology, and the release of the brachioradialis tendon to facilitate reduction of complex fracture patterns. The anatomical plane utilized is essentially the distal extension of the modified Henry approach to the radius, but it specifically exploits the interval between the flexor carpi radialis (FCR) and the radial artery, rather than the more proximal interval between the brachioradialis and the pronator teres.

The transition to utilizing the volar approach almost exclusively for distal radius fixation is heavily supported by its relatively low rate of catastrophic soft tissue complications when executed flawlessly. Unlike the dorsal approach, where the extensor tendons are in intimate contact with the bone and highly susceptible to attrition and rupture over hardware, the volar approach allows for submuscular plating. However, this approach demands a profound understanding of the local neurovascular anatomy, specifically the radial artery, the median nerve, and its palmar cutaneous branch. Mastery of this surgical corridor is an absolute prerequisite for any orthopedic surgeon, resident, or hand fellowship trainee.
Detailed Surgical Anatomy and Biomechanics
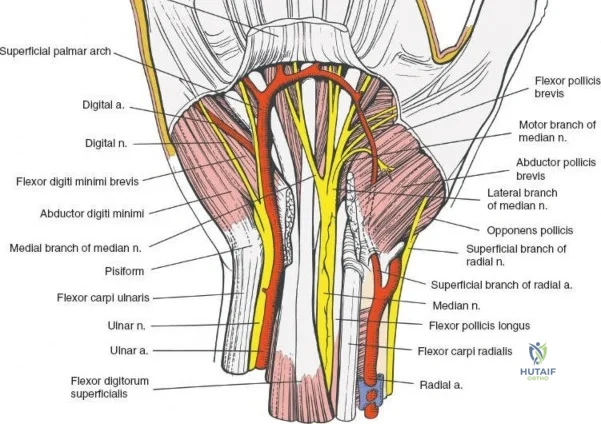
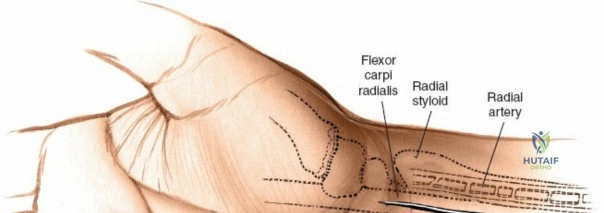
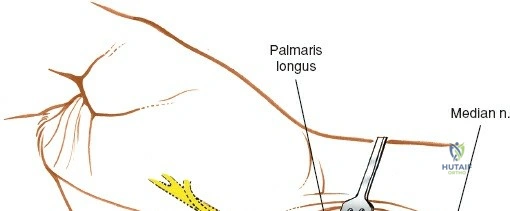
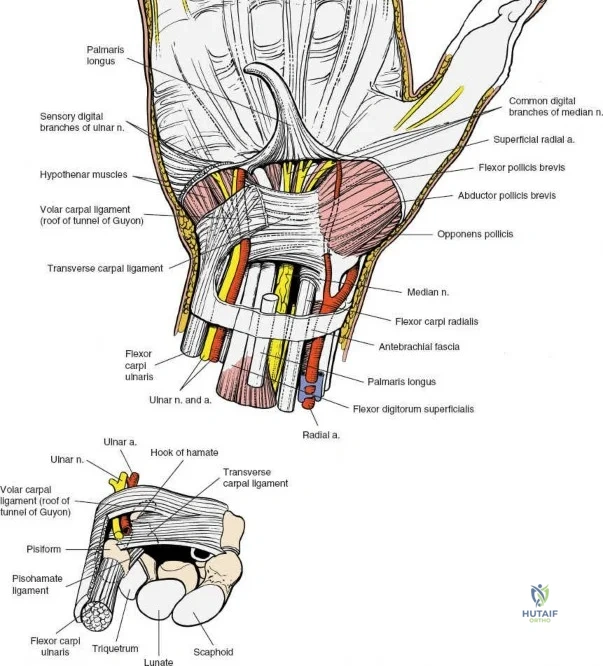
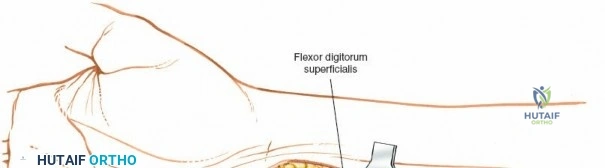
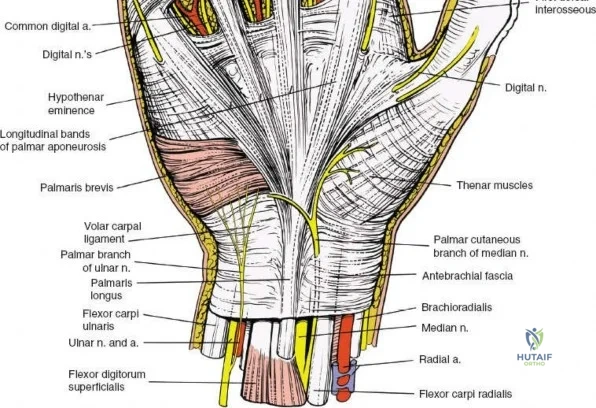
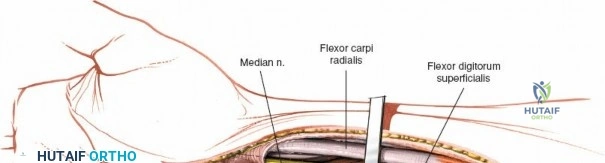
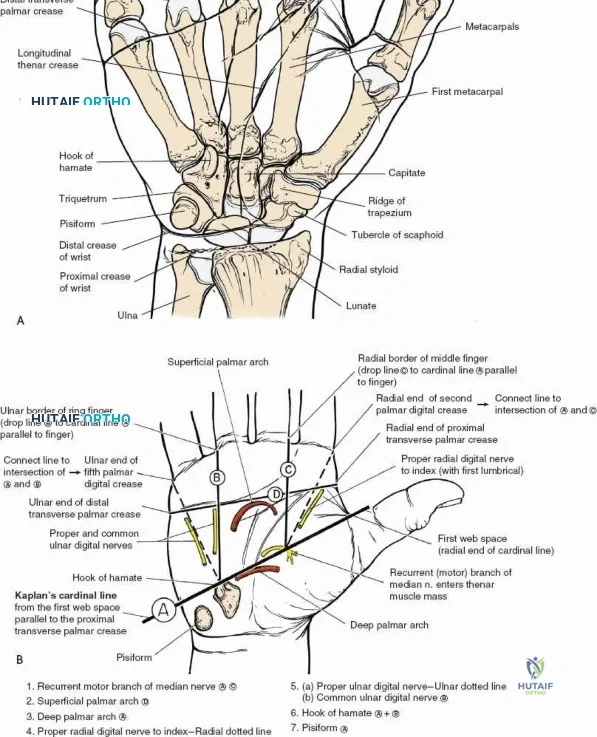
A rigorous understanding of the volar wrist anatomy is the cornerstone of a safe and effective volar approach. The surgical corridor relies on a precise internervous plane located between the flexor carpi radialis (FCR), which is innervated by the median nerve, and the brachioradialis, which is innervated by the radial nerve. However, in the distal forearm, the dissection is more accurately described as an inter-structural plane between the FCR tendon and the radial artery. The FCR tendon is a thick, robust structure that acts as the primary anatomical landmark. It lies radial to the palmaris longus (when present) and ulnar to the radial artery. Incising the FCR sheath and retracting the tendon ulnarly protects the median nerve, which lies deep and slightly ulnar to the FCR in the distal forearm.
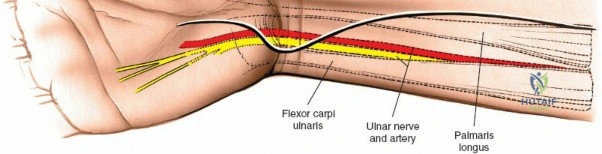
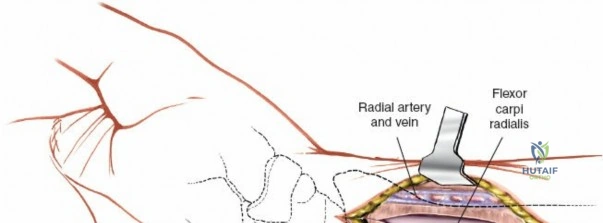
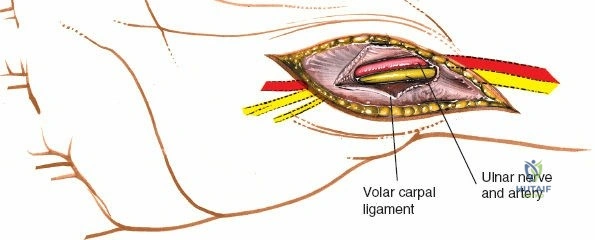
The radial artery is the primary vascular structure at risk during this exposure. It courses distally under the cover of the brachioradialis in the mid-forearm but becomes relatively superficial in the distal third, lying just radial to the FCR tendon. The artery is accompanied by venae comitantes, which can often be more visually prominent than the artery itself, especially when an exsanguinating tourniquet is utilized. Retraction of the radial artery radially is a critical step; however, excessive traction must be avoided to prevent vasospasm or intimal tear. Several small perforating branches from the radial artery supply the radial metaphysis and the brachioradialis; these often require meticulous bipolar electrocautery or ligation to mobilize the artery safely and access the radial styloid.
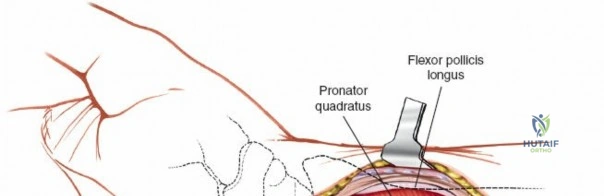
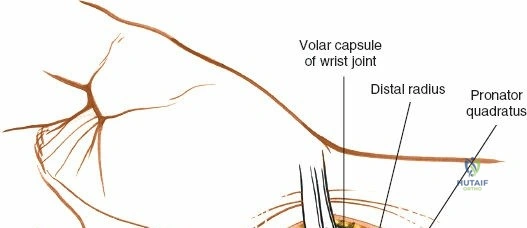
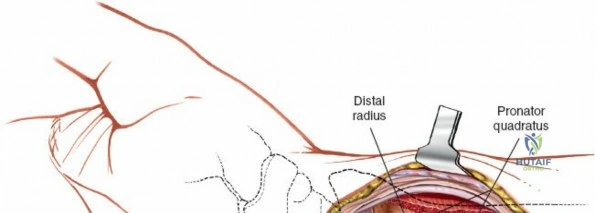
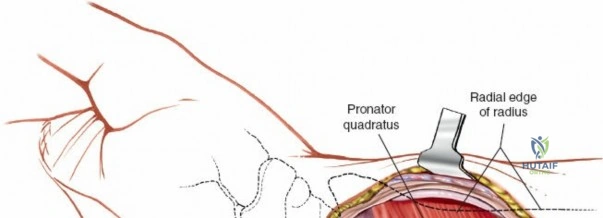
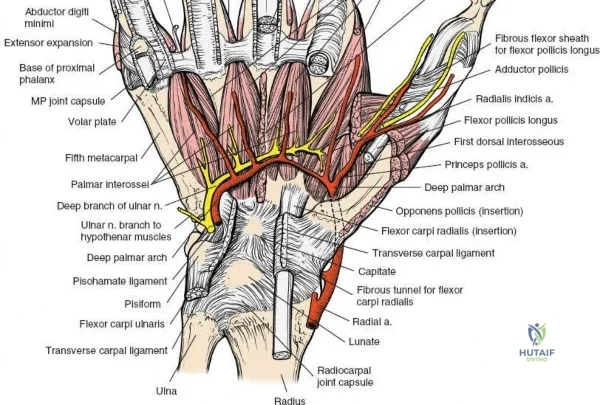
Deep to the superficial flexors lies the pronator quadratus (PQ) muscle, a quadrilateral muscle that spans the distal radioulnar joint. The PQ originates from the distal anterior ulna and inserts onto the distal anterior radius. It is innervated by the anterior interosseous nerve (AIN) and receives its blood supply from the anterior interosseous artery. The PQ serves as a critical anatomical landmark and a biological shield. The muscle covers the volar aspect of the distal radius, and its elevation is mandatory to visualize the fracture site. Distal to the PQ insertion lies the "watershed line," a transverse anatomical ridge on the volar margin of the distal radius. This line represents the distal limit of safe plate placement; hardware placed distal to this line directly impinges on the flexor pollicis longus (FPL) and deep flexor tendons, drastically increasing the risk of iatrogenic tendon rupture.
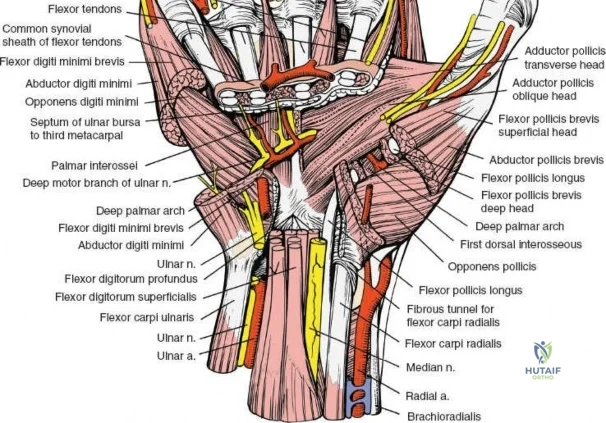
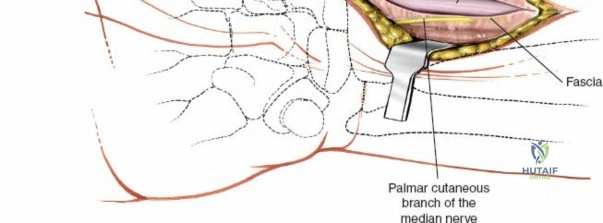
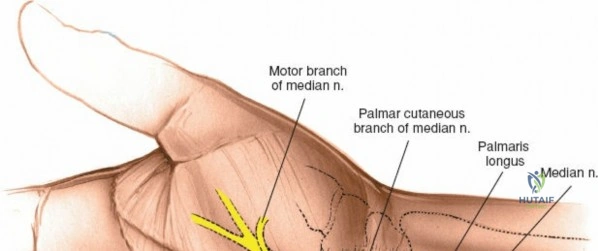
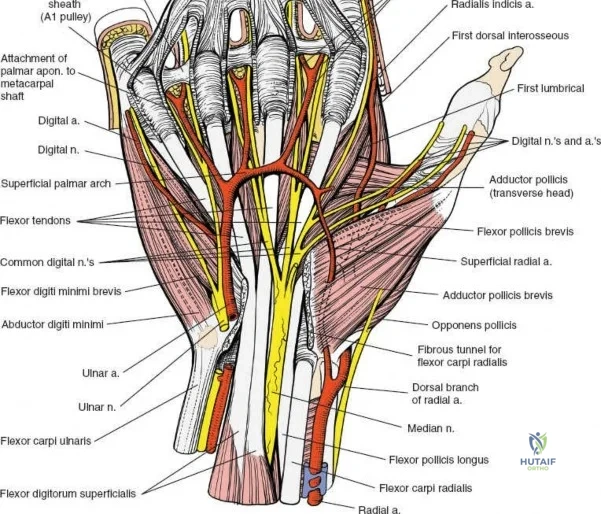
The median nerve and its palmar cutaneous branch (PCBMN) dictate the ulnar limits of the dissection. The PCBMN typically branches from the radial aspect of the median nerve approximately 5 cm proximal to the radiocarpal joint. It courses distally between the FCR and palmaris longus before piercing the antebrachial fascia to provide sensation to the base of the thenar eminence. By strictly maintaining the dissection deep to the FCR tendon sheath and retracting the FCR ulnarly, the surgeon effectively protects both the main trunk of the median nerve and the PCBMN. Straying ulnar to the FCR or failing to utilize the protective sheath exposes these critical neural structures to iatrogenic injury, retraction neuropraxia, or postoperative perineural fibrosis.
Exhaustive Indications and Contraindications
The volar approach is highly versatile, but patient selection and patho-anatomical considerations must dictate its utilization. It is the gold standard for the vast majority of distal radius fractures requiring operative intervention. Specifically, volar shear fractures (Barton's fractures), volarly displaced extra-articular fractures (Smith's fractures), and the majority of dorsally displaced fractures (Colles' fractures) are optimally managed via this route. The mechanical advantage of a volar locking plate acting as an internal fixator allows for the neutralization of bending forces and maintenance of reduction even in osteoporotic bone, making it highly indicated for the elderly population where prolonged cast immobilization is deleterious.
Beyond acute trauma, the volar approach is indicated for the management of delayed unions and nonunions of the distal radius, allowing for simultaneous rigid internal fixation and the application of autologous or allogeneic bone graft. It is the preferred approach for corrective osteotomies to address malunions, as the volar surface allows for easier application of structural grafts and fixed-angle plating to restore the critical volar tilt (normally 11 degrees). Furthermore, the approach can be utilized for the excision of a symptomatic radial styloid (e.g., in cases of scaphoid nonunion advanced collapse - SNAC wrist) or for the release of the brachioradialis tendon, which is often a major deforming force in radial styloid and complex intra-articular fractures.
Despite its ubiquity, strict contraindications exist. The volar approach is relatively contraindicated in the setting of severe, isolated dorsal highly comminuted fractures with significant dorsal bone loss where a volar plate cannot adequately capture or support the dorsal articular fragments. In such instances, a dorsal approach, fragment-specific fixation, or a dorsal spanning bridge plate may be required. Absolute contraindications include active volar soft tissue infection, severe compromised volar soft tissue envelopes (e.g., severe burns or degloving injuries), and specific complex radiocarpal fracture-dislocations where the primary pathology and capsular avulsions are entirely dorsal.
| Category | Specific Conditions | Rationale |
|---|---|---|
| Primary Indications | Volar shear (Barton's), Smith's, Colles' fractures | Allows direct buttressing of volar cortex; locking technology maintains reduction in osteoporotic bone. |
| Reconstructive Indications | Malunion osteotomies, nonunions, radial styloidectomy | Broad flat surface for corrective plating; easy access for bone grafting. |
| Soft Tissue Indications | Brachioradialis release, median nerve decompression | Extensile nature allows simultaneous carpal tunnel release and deforming force neutralization. |
| Relative Contraindications | Severe isolated dorsal comminution, small dorsal marginal fragments | Volar hardware may not capture dorsal fragments; risks articular subsidence. |
| Absolute Contraindications | Active volar infection, massive volar soft tissue loss | High risk of deep space infection and hardware exposure. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is essential for a successful outcome in distal radius surgery. Standard posteroanterior (PA), lateral, and oblique radiographs are the minimum requirement. However, for complex intra-articular fractures, a non-contrast Computed Tomography (CT) scan with 2D and 3D reconstructions is highly recommended. CT imaging allows the surgeon to delineate the exact number of articular fragments, identify central die-punch fragments, assess the integrity of the volar lunate facet (the critical keystone of the radiocarpal joint), and precisely plan screw trajectories. Digital templating should be performed to estimate plate size, length, and the necessity for supplemental fragment-specific fixation (e.g., radial styloid pins or ulnar-sided buttress plates).

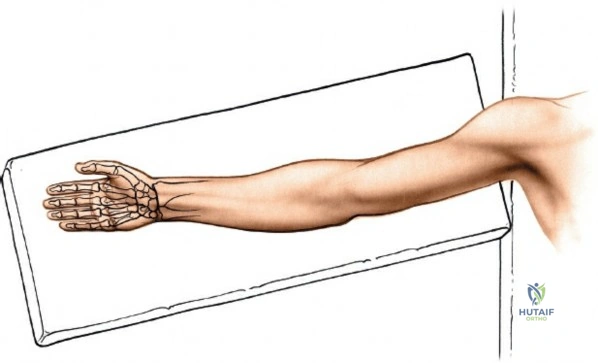
The patient is positioned supine on the operating table. The affected upper extremity is extended onto a radiolucent hand table. It is imperative that the hand table is completely radiolucent and free of metallic artifacts to allow for unimpeded fluoroscopic visualization in multiple planes. A well-padded pneumatic tourniquet is applied to the proximal arm. The arm is prepped and draped in a standard sterile fashion, allowing for visualization and manipulation of the elbow, forearm, and hand. Prior to inflation of the tourniquet, the limb is exsanguinated using an Esmarch bandage to ensure a bloodless surgical field, which is critical for identifying the delicate venae comitantes and the radial artery.
Intraoperative fluoroscopy (C-arm) positioning is a critical component of the setup. The C-arm should be brought in from the head or the foot of the table, perpendicular to the long axis of the limb. The surgeon must be able to obtain true PA and lateral views of the wrist. A "true lateral" is confirmed when the volar surface of the pisiform overlies the central third of the scaphoid pole, and the palmar cortices of the scaphoid and pisiform are collinear. Furthermore, to accurately assess intra-articular screw penetration, the surgeon must utilize a 10 to 15-degree lateral tilt view to account for the normal radial inclination, and a 20 to 30-degree elevated PA view to profile the radiocarpal joint space.


The surgeon typically sits in the axilla facing the hand, while the assistant sits opposite. The forearm is maintained in a supinated position so that the palmar aspect of the wrist faces directly upward. A rolled towel or a dedicated wrist bump is often placed under the dorsal aspect of the wrist to facilitate wrist extension, which aids in fracture reduction through ligamentotaxis and brings the volar anatomy into greater relief. However, care must be taken not to over-extend the wrist in cases of severe volar comminution, as this may exacerbate displacement.
Step-by-Step Surgical Approach and Fixation Technique
Superficial Dissection and Internervous Plane
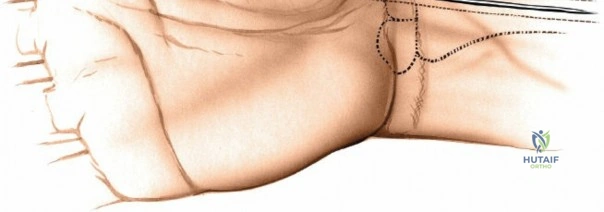
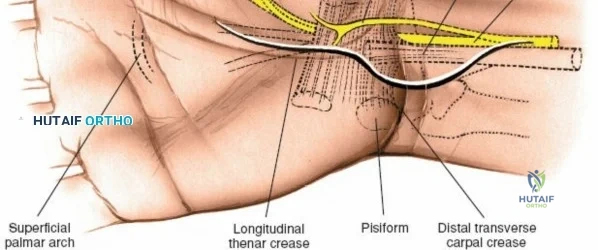
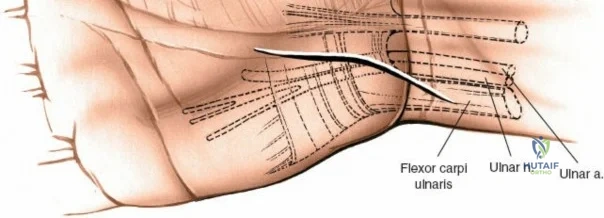
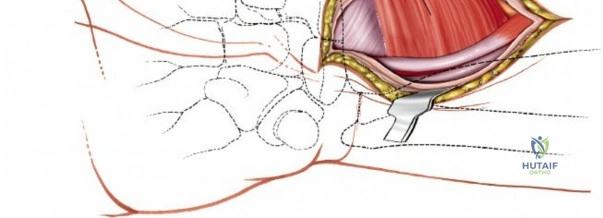
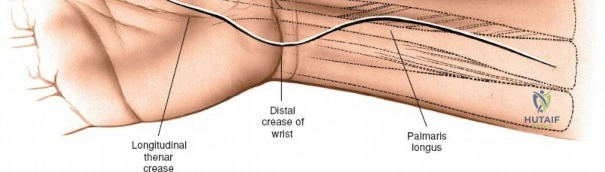
The superficial landmarks must be palpated and marked prior to incision. Identify the radial styloid process, the distal wrist flexion crease, and the thick, cord-like tendon of the flexor carpi radialis (FCR). A longitudinal incision, approximately 5 to 8 centimeters in length, is made directly overlying the FCR tendon. The incision begins just proximal to the distal wrist crease and extends proximally along the volar aspect of the forearm. The length of the incision is dictated by the fracture pattern and the anticipated length of the locking plate. For extensive diaphyseal extension, the incision can be carried proximally following the course of the FCR.
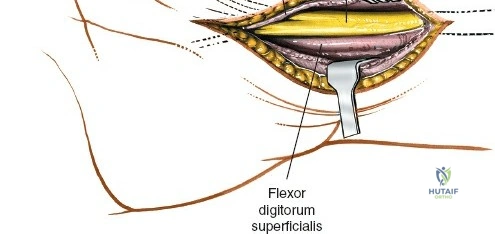
Subcutaneous tissue is divided sharply in line with the skin incision. Meticulous hemostasis is achieved using bipolar electrocautery to protect superficial sensory nerves. The deep fascia overlying the FCR tendon is identified and incised longitudinally. It is critical to incise the fascia directly over the tendon and enter the tendon sheath. The FCR tendon is then mobilized and retracted ulnarly using a blunt retractor (such as a Senn or Ragnell retractor). Retracting the FCR ulnarly is the key maneuver that protects the median nerve and its palmar cutaneous branch, which lie deep and ulnar to the tendon.
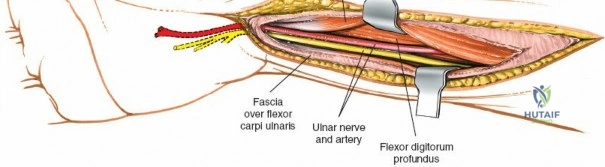
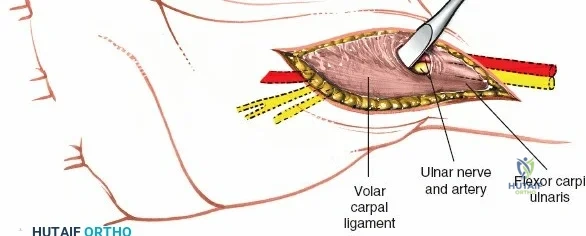
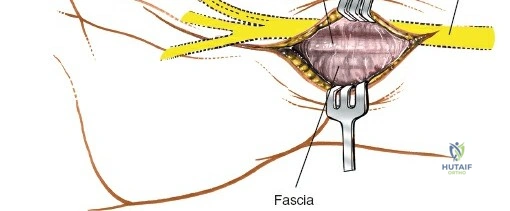
With the FCR retracted, the floor of the FCR sheath is incised to reveal the deep compartment. The radial artery and its venae comitantes are identified on the radial aspect of the exposure. The surgeon must carefully develop the plane between the radial artery (retracted radially) and the FCR tendon (retracted ulnarly). Blunt dissection with a sponge stick or a periosteal elevator is often sufficient to sweep the soft tissues and expose the underlying fascia of the pronator quadratus muscle. During this step, small perforating branches from the radial artery to the radial metaphysis may be encountered; these must be carefully isolated and cauterized to prevent troublesome bleeding upon tourniquet deflation.

Deep Dissection and Pronator Quadratus Management
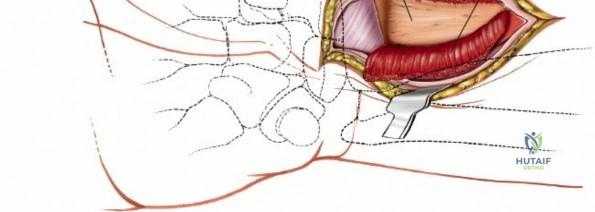
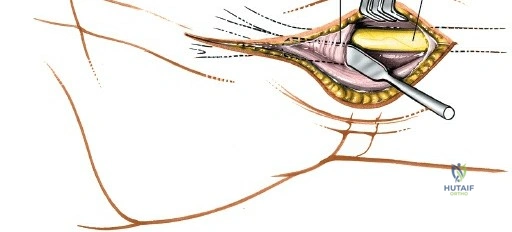
The deep surgical dissection centers on the management of the pronator quadratus (PQ) muscle, which blankets the volar aspect of the distal radius. There are three primary techniques for managing the PQ, and the choice depends on surgeon preference, fracture complexity, and the need for distal exposure. The most common and widely taught method is the Complete Muscle Detachment (L-shaped flap). An incision is made along the radial border of the radius (the insertion of the PQ) starting distal to the brachioradialis insertion and extending distally to the watershed line. A second, transverse incision is made along the distal margin of the PQ, parallel to the joint line. The muscle is then elevated subperiosteally from radial to ulnar, creating a robust, triangular or L-shaped musculofascial flap. This flap provides excellent visualization of the fracture and can be repaired over the plate during closure to protect the flexor tendons.
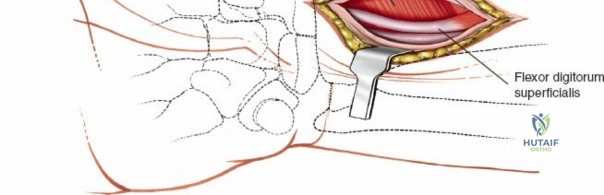
Alternatively, the Minimally Invasive Technique involves identifying the distal insertion of the PQ and detaching it sharply from the bone, leaving the lateral (radial) insertion intact. The surgeon then tunnels underneath the muscle belly to expose the anterior surface of the radius. While this technique preserves the radial blood supply to the PQ and is highly "soft-tissue friendly," it severely limits direct visualization of the fracture site. Reduction must be achieved indirectly via fluoroscopy, and screws are inserted through stab incisions directly through the muscle belly. This technique is generally reserved for simple, extra-articular fracture patterns.
The third method is the Classical Technique, which involves dividing the PQ muscle longitudinally in the line of the skin incision and elevating it medially and laterally. This approach is highly destructive to the muscle fibers and denervates the ulnar half of the muscle. Repair of the muscle is usually impossible due to tissue friability. Consequently, this technique has largely fallen out of favor in modern orthopedic practice, as it leaves the orthopedic hardware directly exposed to the deep flexor tendons, increasing the risk of postoperative tenosynovitis and tendon rupture. Therefore, the L-shaped subperiosteal elevation remains the gold standard.
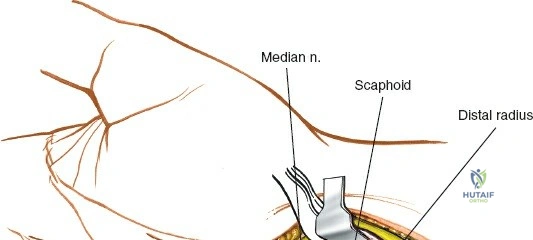
Extension to the Carpal Tunnel and Distal Structures
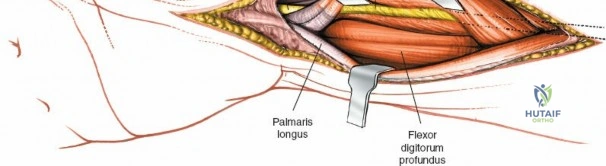
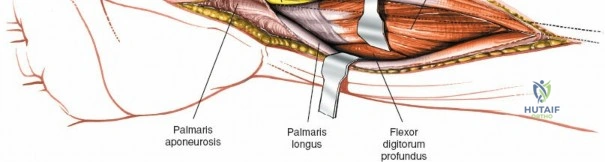
In cases of severe trauma, concomitant acute carpal tunnel syndrome, or when addressing complex radiocarpal fracture-dislocations (e.g., volar Barton's with carpal subluxation), the volar approach can be seamlessly extended distally to decompress the median nerve within the carpal tunnel. The skin incision is extended distally, crossing the wrist flexion creases obliquely (to prevent scar contracture) and continuing into the palm just ulnar to the thenar crease. The palmaris longus tendon (if present) is identified, and the dissection proceeds between the palmaris longus and the FCR.
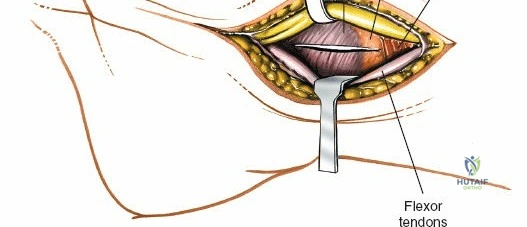
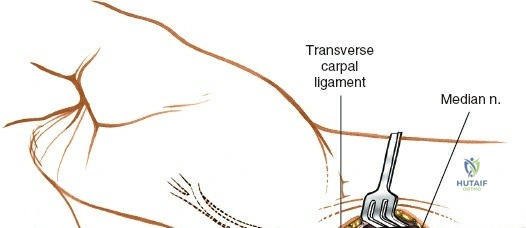
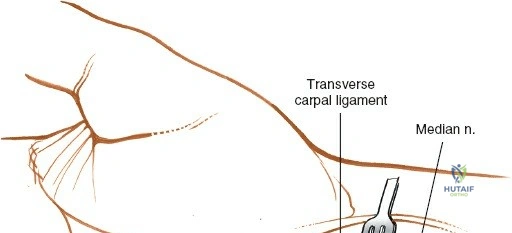
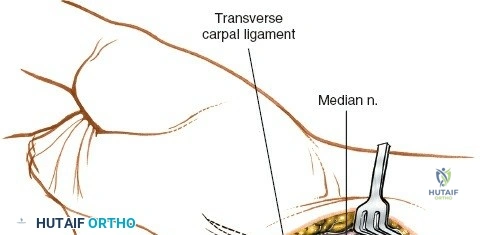
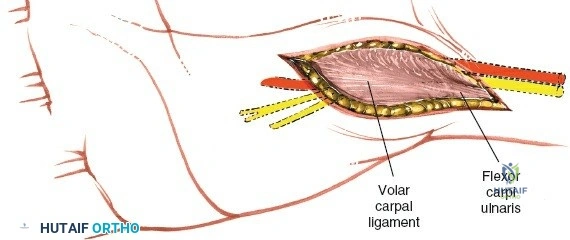
The superficial palmar fascia is incised, revealing the thick, transverse fibers of the flexor retinaculum (transverse carpal ligament). A blunt dissector, such as a McDonald or Freer elevator, is passed carefully down the carpal tunnel, deep to the retinaculum but superficial to the median nerve. The retinaculum is then sharply divided along its extreme ulnar border. Releasing the ligament on the ulnar side is a critical safety measure to avoid iatrogenic injury to the recurrent motor branch of the median nerve, which typically arises from the radial aspect of the nerve and curves upward into the thenar musculature.
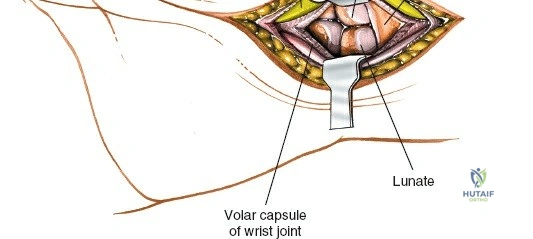
Once the carpal tunnel is open, the median nerve is gently retracted radially, and the flexor tendons are mobilized. This extensile exposure provides unparalleled access to the volar radiocarpal ligaments (radioscaphocapitate, long radiolunate, and short radiolunate ligaments), the volar lip of the lunate facet, and the proximal carpal row. It allows for the direct repair of capsular avulsions, synovectomy of the flexor tendons, or open reduction of transscaphoid perilunate dislocations. Following completion of the deep procedures, the carpal tunnel is left open, and only the skin is closed to prevent postoperative compartmental hypertension.

Complications, Incidence Rates, and Salvage Management
While the volar approach is generally safe, complications can be devastating and are often related to technical errors during hardware placement or soft tissue management. The most feared complication is iatrogenic tendon rupture. Flexor tendon rupture, specifically the Flexor Pollicis Longus (FPL), occurs in approximately 2-12% of cases. This is almost exclusively caused by placing the volar plate distal to the watershed line. The watershed line is the most volar margin of the distal radius; plates placed distal to this prominence will directly abrade the FPL tendon during active flexion. Prevention requires meticulous fluoroscopic evaluation to ensure the plate sits proximal to the watershed line. If FPL rupture occurs, salvage management requires hardware removal and tendon reconstruction, typically using a palmaris longus autograft or an FDS transfer.
Extensor tendon ruptures, particularly of the Extensor Pollicis Longus (EPL), are also well-documented, occurring in 1-5% of cases. In the context of a volar approach, EPL rupture is usually iatrogenic, resulting from dorsal screw penetration. The dorsal cortex of the distal radius is irregular, and Lister's tubercle can obscure the true length of screws on a standard lateral radiograph. Screws that protrude even 1-2 millimeters past the dorsal cortex can cause attrition of the EPL tendon within the third extensor compartment. Intraoperative prevention mandates the use of specialized fluoroscopic views (dorsal horizon view) to confirm screw length. Management of a ruptured EPL requires hardware removal and tendon transfer, most commonly utilizing the Extensor Indicis Proprius (EIP).

Neurological complications primarily involve the median nerve. Transient median nerve neuropraxia is common, often secondary to traction during retraction or postoperative swelling. However, direct injury to the palmar cutaneous branch of the median nerve (PCBMN) can lead to debilitating neuromas and Complex Regional Pain Syndrome (CRPS). Strict adherence to the internervous plane deep to the FCR sheath minimizes this risk. If a neuroma develops, management ranges from conservative therapies (gabapentin, nerve blocks) to surgical excision and implantation of the nerve stump into the pronator quadratus muscle.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| FPL Tendon Rupture | 2% - 12% | Prevention: Keep plate proximal to the watershed line. Salvage: Hardware removal, FDS transfer or interposition graft. |
| EPL Tendon Rupture | 1% - 5% | Prevention: Avoid dorsal screw penetration; use dorsal horizon fluoroscopy. Salvage: Hardware removal, EIP to EPL tendon transfer. |
| Median Nerve Neuropathy | 5% - 15% | Prevention: Avoid excessive ulnar retraction; prophylactic carpal tunnel release if indicated. Salvage: Corticosteroid injections, formal carpal tunnel release. |
| Loss of Reduction / Hardware Failure | 2% - 5% | Prevention: Ensure adequate subchondral screw purchase; recognize severe osteopenia. Salvage: Revision ORIF with bone grafting or salvage wrist arthrodesis. |
Phased Post-Operative Rehabilitation Protocols
The primary advantage of rigid internal fixation via a volar locking plate is the ability to initiate early postoperative rehabilitation, thereby mitigating the stiffness and capsular contractures historically associated with prolonged cast immobilization. The rehabilitation protocol is phased, respecting the biology of bone healing while maximizing functional return. Phase 1 (0-2 weeks) focuses on edema control and immediate digital motion. The patient is placed in a bulky soft dressing and a removable volar orthosis immediately postoperatively. Active and passive range of motion of the fingers and thumb is initiated on postoperative day one to prevent tendon adhesions. Elevation and compressive wrapping are utilized to combat swelling, which is the primary antagonist to early motion.
Phase 2 (2-6 weeks) begins at the first postoperative visit following suture removal. The patient is transitioned to a
Clinical & Radiographic Imaging Archive