Operative Management of Septic Arthritis and Post-Infectious Deformities
Key Takeaway
Septic arthritis requires prompt surgical intervention to prevent irreversible joint destruction, ankylosis, and severe contractures. This comprehensive guide details the operative management of acute joint sepsis in the wrist, alongside advanced reconstructive osteotomies for post-infectious deformities in the ankle, knee, and hip. Mastery of these techniques is essential for orthopedic surgeons to restore biomechanical alignment and optimize functional outcomes in complex post-septic joints.
Acute Septic Arthritis of the Wrist
Septic arthritis of the wrist is encountered less frequently than in large weight-bearing joints and typically manifests following direct penetrating trauma, intra-articular injections, or hematogenous spread in immunocompromised hosts. The clinical signs may be deceptively subtle, lacking the dramatic erythema and swelling seen in superficial joints, which frequently leads to a delayed or missed diagnosis.
Prompt recognition followed by early incision and drainage is paramount. Failure to decompress and sterilize the joint rapidly inevitably leads to devastating complications, including fibrous or bony ankylosis, periarticular osteomyelitis, or contiguous suppurative flexor tenosynovitis.
Diagnostic Aspiration
Aspiration is the critical first step in both diagnosis and targeted antimicrobial therapy. The procedure is strictly performed on the dorsal aspect of the wrist to avoid the complex volar neurovascular structures (radial and ulnar arteries, median nerve).
Several safe aspiration corridors exist on the dorsum of the wrist:
* Primary Site (Radiocarpal Joint): The most common and accessible site is located between the first and second extensor compartments at the radiocarpal level. The needle is introduced immediately adjacent to the intersection where the extensor pollicis longus (EPL) crosses the extensor carpi radialis longus (ECRL) and brevis (ECRB).
* Alternative Sites: Aspiration can also be safely performed between the third and fourth extensor compartments (ulnar to Lister's tubercle) or between the fourth and fifth extensor compartments.
Surgical Warning: Always use a sterile technique and a large-bore needle (18-gauge) to ensure thick, purulent fluid can be successfully aspirated. Fluid must be sent immediately for cell count, Gram stain, and aerobic/anaerobic cultures.
Surgical Drainage Approaches
The wrist joint can be adequately decompressed and drained via lateral, medial, or posterior (dorsal) approaches. The choice of approach depends on the primary site of fluctuance and the surgeon's preference.
Clinical Pearl: Regardless of the approach chosen, meticulous care must be taken to avoid inadvertently opening adjacent uninvolved tendon sheaths, which can rapidly convert an isolated joint infection into a catastrophic pan-compartmental tenosynovitis.
🔪 Surgical Technique: Lateral Drainage
- Incision: Make a 5 cm longitudinal incision centered over the radial aspect of the wrist. The interval lies between the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons volarly, and the extensor pollicis longus (EPL) tendon dorsally.
- Deep Dissection: Deepen the incision directly into the anatomical snuffbox.
- Neurovascular Protection: Identify and gently retract the superficial sensory branch of the radial nerve. Exercise extreme caution to identify and protect the radial artery, which traverses the floor of the snuffbox.
- Arthrotomy: Incise the radial collateral ligament and the underlying synovium longitudinally to enter the radiocarpal joint. Evacuate all purulent material.
- Irrigation and Closure: Copiously irrigate the joint with normal saline (minimum 3-5 liters). Leave the capsule open. Close the skin loosely over a passive drain (e.g., Penrose) or leave the wound open for delayed primary closure.
🔪 Surgical Technique: Medial Drainage
- Incision: Make a 5 cm longitudinal incision over the ulnar head, utilizing the interval between the flexor carpi ulnaris (FCU) and the extensor carpi ulnaris (ECU) tendons.
- Neurovascular Protection: Carefully dissect the subcutaneous tissues to identify and protect the dorsal sensory branch of the ulnar nerve, which crosses from volar to dorsal in this vicinity.
- Arthrotomy: Expose the ulnar collateral ligament and the joint capsule. Incise the capsule distal to the ulnar styloid process.
- TFCC Preservation: Do not detach or violate the triangular fibrocartilage complex (TFCC), as this will lead to chronic distal radioulnar joint (DRUJ) instability.
- Irrigation: Evacuate the pus and irrigate thoroughly.
🔪 Surgical Technique: Dorsal Drainage
- Incision: Make a 5 cm dorsal longitudinal incision. The preferred intervals are either between the EPL and the extensor indicis proprius (EIP) tendons, or more ulnarly between the ECU and the extensor digiti minimi (EDQ) tendons.
- Arthrotomy: Incise the extensor retinaculum (dorsal carpal ligament) to mobilize the tendons. Perform a longitudinal capsulotomy to enter the radiocarpal joint.
- Postoperative Care: The wrist is splinted in the functional position (20-30 degrees of extension) until the acute inflammation subsides and the wound stabilizes. Active range-of-motion (ROM) exercises are initiated as soon as clinically permissible to prevent capsular contracture.
Operations to Correct Deformities After Septic Arthritis
When acute septic arthritis is missed or inadequately treated, the end result is often severe joint destruction leading to fixed contractures or ankylosis. Reconstructive surgery is frequently required to restore a functional, plantigrade limb.
The Ankle: Management of Equinus Deformity
Post-infectious ankle deformities most commonly present as a fixed equinus contracture. The management algorithm is dictated by whether the contracture is purely soft-tissue in nature or the result of bony ankylosis.
Soft-Tissue Contractures:
When the ankle is fixed in equinus due to posterior capsular and musculotendinous contracture, conservative measures such as Quengel casting (low-load, prolonged stretch) or serial wedged casts may be attempted. If refractory, operative intervention is required. Lengthening of the Achilles tendon (TAL), combined with a comprehensive posterior ankle capsulotomy, is generally highly effective in restoring a plantigrade foot position.
Bony Ankylosis:
When fixed equinus is caused by solid bony ankylosis across the tibiotalar joint, soft-tissue releases are futile. A corrective cuneiform osteotomy through the fused joint mass is indicated.
🔪 Surgical Technique: Ankle Cuneiform Osteotomy
- Approach: Expose the ankylosed ankle joint through a standard anterolateral approach.
- Osteotomy: Using a sharp osteotome or oscillating saw, resect a cuneiform (wedge-shaped) segment of bone from the fused joint mass. The base of the wedge must be anterior to correct the equinus deformity.
- Soft-Tissue Balancing: If necessary, perform a percutaneous or open Achilles tendon lengthening and posterior capsulotomy. This prevents the need to resect an excessive amount of bone to achieve correction, which would result in unacceptable limb shortening.
- Alignment: Dorsiflex the foot to a neutral (0 degrees) plantigrade position. Ensure the bony surfaces of the osteotomy are accurately apposed and flush.
- Fixation: Apply rigid fixation. An external fixation device (e.g., Ilizarov or Taylor Spatial Frame) or robust internal compression plating (as used in primary ankle arthrodesis) is applied to maintain compression across the osteotomy site.
- Postoperative Care: The limb is maintained in a non-weight-bearing cast or fixator until radiographic union is confirmed, typically at 8 to 12 weeks.
The Knee: Management of Flexion Contractures
Severe flexion contractures of the knee following sepsis are notoriously difficult to manage. While mild soft-tissue contractures may respond to serial casting or posterior soft-tissue releases, rigid fibrous or bony ankylosis requires complex osteotomies.
Surgical Warning: Acute correction of severe knee flexion contractures (>60 degrees) carries a high risk of traction injury to the peroneal nerve and popliteal artery. Staged correction using circular external fixators should be strongly considered for extreme deformities.
Transverse Supracondylar Osteotomy of the Femur
A flexion deformity can be corrected indirectly by a supracondylar osteotomy that creates a compensatory extension deformity in the distal femur. This is indicated for mild-to-moderate flexion deformities where the joint itself is unsuitable for manipulation or release. In pediatric patients, the osteotomy must be meticulously planned well proximal to the distal femoral physis.
🔪 Surgical Technique: Transverse Supracondylar Osteotomy
- Approach: Make a 2.5 cm lateral longitudinal incision just proximal to the lateral femoral condyle. Incise the fascia lata and split the vastus lateralis to expose the femoral metaphysis.
- Bone Cut: Insert an osteotome and turn it transversely. Divide the femur laterally and posteriorly through approximately two-thirds of its cortical thickness.
- Correction: By manual manipulation, create a controlled greenstick fracture in the remaining intact medial/anterior cortex. Extend the distal fragment to correct the flexion deformity.
- Adjuncts: If the preoperative flexion contracture exceeds 45 degrees, a fractional lengthening of the hamstring tendons should be performed prior to the osteotomy to reduce tension.
- Postoperative Care: Apply a long-leg cast with a pelvic band. At 2 weeks, the cast is wedged or changed to permit further gradual correction. At 8 to 12 weeks, transition to a long-leg orthosis locked in neutral extension.
V-Osteotomy of the Femur (Thompson Technique)
Ankylosis of the knee in flexion may also be addressed via the Thompson V-osteotomy, which provides inherent multi-planar stability through its geometric bone cuts.
🔪 Surgical Technique: Thompson V-Osteotomy
- Bone Cuts: Divide the anterior cortex of the femur using a V-shaped osteotomy. Divide the medial and lateral cortices obliquely, and complete the cut by dividing the posterior cortex transversely.
- Impaction: Create an excavation (trough) in the cancellous bone of the distal fragment. Insert the pointed, V-shaped end of the proximal fragment directly into this trough, creating a stable telescoping effect.
- Decompression: If the correction places undue tension on the posterior neurovascular structures, resect a measured portion of the proximal fragment to shorten the limb slightly and relieve tension.
Supracondylar Controlled Rotational Osteotomy of the Femur
This modification of the Osgood osteotomy is indicated when a functional arc of flexion remains beyond the fixed flexion contracture. The goal is to rotate the functional arc into a more physiological position (restoring full extension), though this inherently sacrifices some maximum flexion.
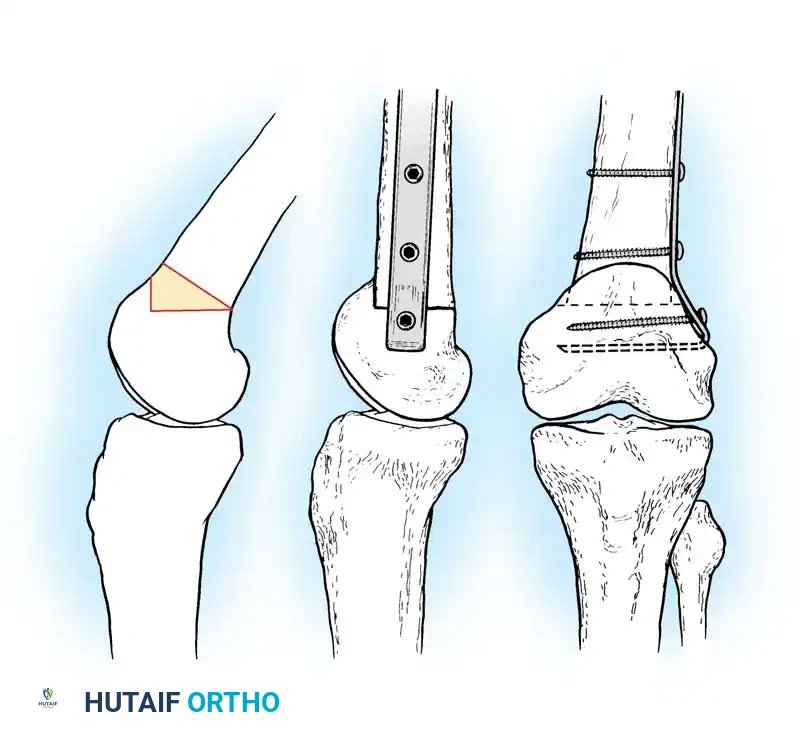
Fig. 17-25 Modification of Osgood supracondylar controlled rotation osteotomy of femur. A, Yellow area illustrates section of bone to be removed. B, After osteotomy, corrected position is maintained by blade plate.
🔪 Surgical Technique: Rotational Osteotomy
- Approach: Through a 10 cm lateral incision, subperiosteally expose the supracondylar area of the femur laterally and anteriorly.
- Osteotomy: Using a reciprocating motor saw, remove a small quadrilateral segment of bone. Cut the distal end of the proximal fragment transversely, and the proximal end of the distal fragment at a calculated angle.
- Rotation: Rotate the distal femoral condyles anteriorly to achieve full clinical extension.
- Fixation: Bend a Blount blade plate (or modern 95-degree condylar blade plate/locking plate) to slightly more than a right angle. Insert the blade transversely into the distal fragment parallel to the joint line, and secure the plate to the proximal femoral shaft with cortical screws.
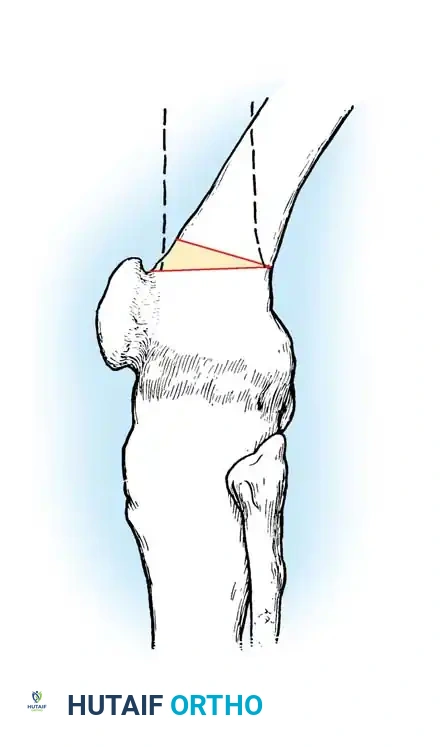
Supracondylar Cuneiform Osteotomy of the Femur
When the flexion contracture exceeds 60 degrees, a simple transverse osteotomy provides insufficient bony apposition once the deformity is corrected. A cuneiform (wedge) osteotomy is required, particularly in adult patients with dense bone.
Fig. 17-24 Cuneiform osteotomy based anteriorly. Section of bone removed is indicated by yellow area. Dotted lines show position of femur after osteotomy, with complete apposition of raw surfaces of fragments.
🔪 Surgical Technique: Cuneiform Osteotomy
- Approach: Make a 7.5 cm lateral longitudinal incision starting just proximal to the lateral femoral condyle. Divide the fascia lata, split the vastus lateralis, and retract it anteriorly.
- Wedge Resection: Remove a wedge-shaped section of bone from the anterior surface of the femoral metaphysis. The angle of the resected wedge should be approximately half the angle of the clinical flexion contracture.
- Closure: Extend the knee to close the anterior gap. This maneuver will simultaneously open a small gap posteriorly.
- Fixation: Secure the osteotomy with a compression clamp, rigid internal plating, or a circular external fixator. Rigid fixation is critical to hasten union, especially when the knee is solidly ankylosed.
Intraarticular Osteotomy
In cases where intraarticular osseous ankylosis has occurred in extreme flexion, weight-bearing is impossible. If total knee arthroplasty (TKA) is contraindicated due to young age, high physical demands, or history of recalcitrant infection, an intraarticular osteotomy is the procedure of choice.
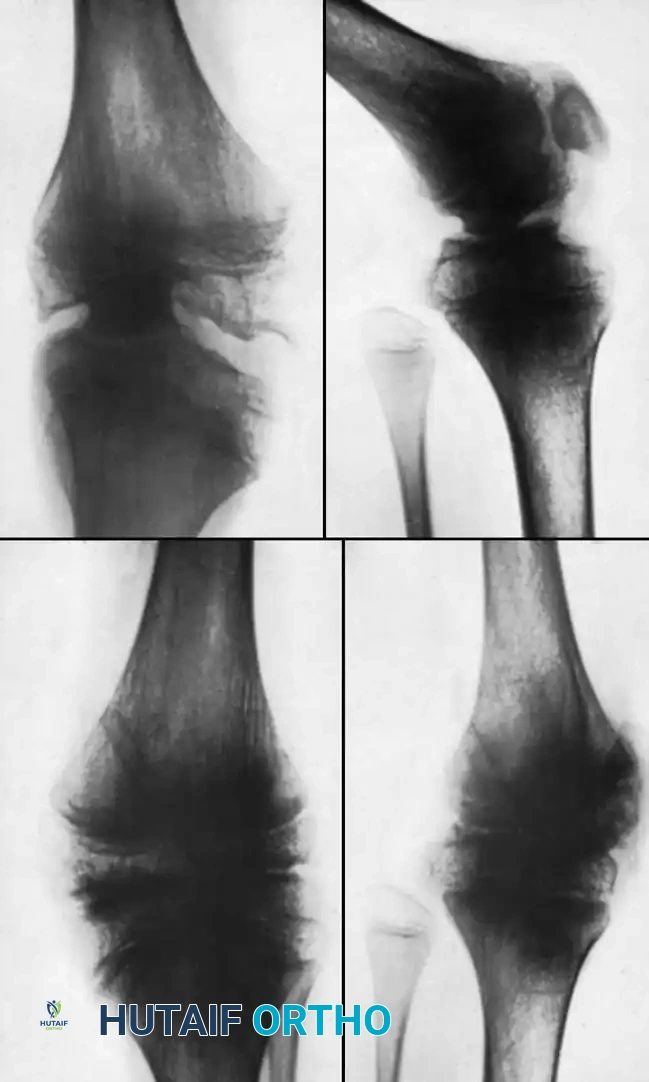
Fig. 17-26 A, Ankylosis and deformity of knee after pyogenic arthritis. B, After intraarticular osteotomy and arthrodesis. Physes were not injured by surgery.
Pediatric Consideration: In children, the distal femoral and proximal tibial physes must be meticulously identified and protected. Injury to these growth plates will result in severe limb length discrepancies and secondary angular deformities.
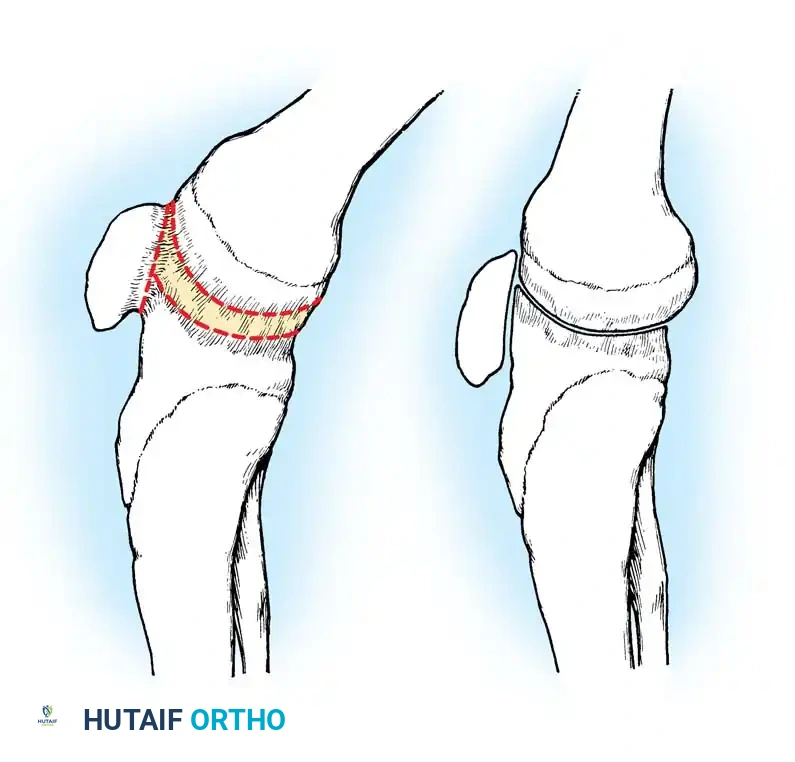
Fig. 17-27 Intraarticular osteotomy for ankylosis of knee in flexion. A, Broken lines show where bone is divided, conforming to general contour of joint surfaces. B, After correction.
🔪 Surgical Technique: Intraarticular Osteotomy
- Approach: Utilize a standard medial parapatellar arthrotomy. Free the patella from the femur (if fused) and strip the soft tissues subperiosteally from the anterior surfaces of the femur and tibia.
- Moderate Deformity: Make the osteotomy cuts parallel to the native contour of the femoral condyles and tibial plateau.
- Extreme Deformity: Remove a large anterior wedge of bone encompassing the fused joint line.
- Staged Correction: If the deformity is extreme, do not attempt full acute correction, as this will stretch the popliteal artery and peroneal nerve. Instead, partially correct the deformity by excising bone. Two weeks later, perform a posterior capsulotomy and hamstring lengthening, followed by gradual extension casting or external fixation.
- Fixation: Once satisfactory alignment is achieved, immobilize the joint with robust external fixation or dual orthogonal plating to achieve solid arthrodesis.
The Hip: Post-Septic Reconstruction
Reconstructive surgery for a hip destroyed by septic arthritis is highly complex and should be significantly delayed until all clinical and laboratory signs of infection have completely subsided.
The rationale for delayed reconstruction is threefold:
1. Infection Control: The risk of reactivating a dormant bacterial biofilm is minimized.
2. Bone Reconstitution: In pediatric patients, early radiographs may mimic complete destruction and osteonecrosis of the femoral head. Given time, the necrotic bone often revascularizes, and abscess cavities fill in, drastically improving the bone stock available for reconstructive surgery.
3. Biomechanical Optimization: Allowing the bone to strengthen increases the likelihood of successful hardware purchase and osteotomy healing.
However, an unstable, dislocated hip should not be left untreated throughout the entire period of growth, nor should a severe fixed deformity be allowed to persist indefinitely, as this leads to secondary spinal and pelvic obliquity.
Arthroplasty Options
- Interposition or Cup Arthroplasty: Historically useful in younger patients with an ankylosed hip to restore motion. While largely replaced by modern techniques, it remains a salvage option in specific scenarios.
- Total Hip Arthroplasty (THA): The gold standard for older patients with post-septic arthritis. THA in this setting must be performed in close collaboration with an infectious disease consultant. Extensive preoperative workup (including joint aspiration for cultures) and targeted perioperative antibiotics are mandatory.
Operations to Stabilize the Hip
When arthroplasty is contraindicated, the hip may be stabilized via several time-tested, albeit complex, reconstructive procedures:
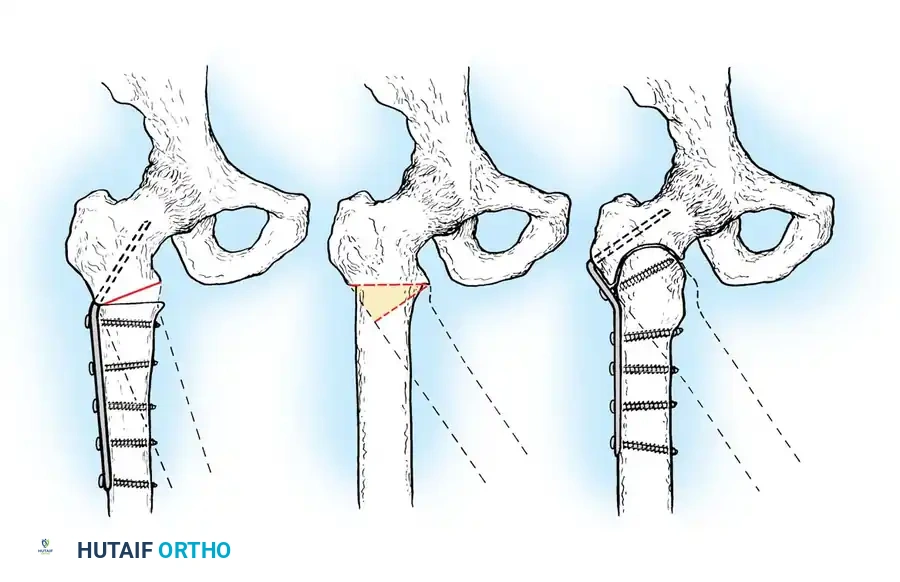
Radiographic and diagrammatic representation of proximal femoral osteotomies utilized for pelvic support and stabilization in the post-septic hip.
- Arthrodesis: Provides a stable, painless hip at the cost of mobility. It is highly effective in young, heavy laborers who would rapidly wear out a THA.
- Pelvic Osteotomy: Procedures such as the Salter innominate osteotomy or Chiari pelvic displacement osteotomy are invaluable in children. They provide crucial superior coverage and support for a proximally migrated femur when the native head and neck have been resorbed by infection. This decreases the Trendelenburg limp and preserves mobility.
- Proximal Femoral Osteotomy (Schanz): A pelvic support osteotomy that redirects the femoral shaft to abut the pelvis, providing a stable fulcrum for weight-bearing when the femoral head is absent.

Postoperative radiograph demonstrating a high-angle proximal femoral osteotomy to restore mechanical alignment and abductor tension.
- Trochanteric Arthroplasty (Colonna): Involves placing the greater trochanter into the acetabulum to serve as a new femoral head, often combined with a proximal femoral osteotomy to restore the mechanical axis.
- Harmon or L’Episcopo Reconstruction: Advanced salvage procedures designed to reconstruct the proximal femur and stabilize the hip joint using local bone grafts and muscle transfers. While considered antiquated by some, mastery of these techniques provides the reconstructive surgeon with critical salvage options in catastrophic, bone-depleted scenarios.
