Pediatric Septic Arthritis: Risk Factors, Epidemiology, and Critical Meta-Analysis
Key Takeaway
Age under 3 years and male sex are significant risk factors for pediatric septic arthritis. Younger children are vulnerable due to immature immune systems. Bias and heterogeneity analysis in meta-analyses are crucial for ensuring the reliability of pooled evidence, helping orthopedic surgeons make informed clinical decisions by accounting for methodological study quality.
As orthopedic surgeons and medical educators, our approach to septic arthritis must be grounded in robust clinical evidence, critically evaluating not only the identified risk factors but also the methodological rigor of the studies informing our understanding. The presented meta-analysis data, delineated across supplementary tables S3, S4, and S5, provides a crucial framework for understanding pediatric septic arthritis risk factors, while simultaneously highlighting the paramount importance of bias and heterogeneity assessment in synthesizing medical literature.
Septic arthritis remains an acute orthopedic emergency, demanding prompt recognition and aggressive intervention to preserve joint function and prevent devastating long-term sequelae such as osteonecrosis, growth plate arrest, and degenerative arthrosis. While clinical presentation and laboratory markers guide diagnosis, identifying patient populations at higher risk facilitates early suspicion and intervention. The data presented here scrutinizes age and sex as risk factors, providing a lens through which to consider the quality and consistency of the underlying evidence.
Introduction and Epidemiology
Septic arthritis, or pyogenic arthritis, represents a severe inflammatory condition of a joint, typically bacterial in origin, characterized by the presence of pus in the joint space. It is an orthopedic emergency because unchecked infection can rapidly destroy articular cartilage, leading to permanent joint damage, functional impairment, and systemic complications including sepsis and death. The condition can affect any joint but is most common in large weight-bearing joints such as the hip and knee, particularly in children.
The incidence of pediatric septic arthritis varies with age, geography, and underlying comorbidities. Global estimates range from 4 to 10 cases per 100,000 children annually. Distinct age-related incidence peaks are observed: neonates (0-3 months), infants (3-12 months), and young children (1-5 years). Neonates are particularly vulnerable due to immature immune systems and the unique metaphyseal vascular anatomy allowing infection to transgress the physis into the epiphysis and joint capsule. Predisposing factors include prematurity, low birth weight, umbilical catheterization, intravenous drug use in adolescents, and immunocompromised states. Recent trauma, skin infections, or distant foci of infection can also precede septic arthritis.
The most common causative organism in pediatric septic arthritis is Staphylococcus aureus, accounting for a significant majority of cases across all age groups. Other prevalent pathogens vary by age:
* Neonates: Staphylococcus aureus, Group B Streptococcus (Streptococcus agalactiae), and Gram-negative bacilli (e.g., Escherichia coli) are common.
* Infants and Young Children (3 months to 5 years): Kingella kingae has emerged as an important pathogen, often difficult to culture with standard methods but identifiable via PCR. Staphylococcus aureus remains primary.
* Older Children and Adolescents: Staphylococcus aureus, Group A Streptococcus (Streptococcus pyogenes), and Neisseria gonorrhoeae in sexually active adolescents.
* Immunocompromised Patients: A broader spectrum of organisms, including atypical bacteria and fungi, must be considered.
Understanding risk factors such as age and sex, as illuminated by rigorous meta-analyses, enhances diagnostic suspicion. While males have historically been reported to have a slightly higher incidence, robust meta-analyses provide a more nuanced understanding, adjusting for potential biases inherent in individual studies. The rapid progression of articular cartilage destruction by bacterial enzymes and inflammatory mediators necessitates expeditious diagnosis and management to mitigate devastating long-term sequelae.
Surgical Anatomy and Biomechanics
A profound understanding of pediatric joint anatomy and its unique biomechanical properties is paramount in managing septic arthritis. The susceptibility and specific sequelae of infection are often dictated by age-dependent anatomical features, particularly regarding the growth plates and vascular supply.
Pediatric Joint Anatomy and Vascularity
The hip joint is frequently affected in septic arthritis, particularly in infants. The epiphyseal blood supply to the femoral head, crucial for its viability, is predominantly intracapsular. Increased intra-articular pressure from a purulent effusion can tamponade these vessels, leading to avascular necrosis (AVN) of the femoral head, a devastating complication. The synovial lining of the hip capsule extends to the femoral neck. In neonates and infants, metaphyseal vessels may perforate the physis, providing a pathway for metaphyseal osteomyelitis to directly seed the joint. The close proximity of the physis to the joint capsule also makes it vulnerable to damage from infection and surgical intervention.
The knee joint, another common site, possesses a large synovial space, allowing for significant accumulation of purulent fluid. While less prone to AVN than the hip, extensive cartilage destruction can occur rapidly due to the large surface area and direct contact with infected fluid. The patella, distal femoral epiphysis, and proximal tibial epiphysis contain multiple growth centers, all vulnerable to infectious damage. The synovial membrane's extensive folds and villi can harbor persistent infection if not adequately debrided.
Other joints like the shoulder, elbow, and ankle also present specific anatomical considerations. The shoulder's generous joint capsule can accommodate large effusions. The elbow has multiple growth plates around the humerus, radius, and ulna, which are critical for future limb length and alignment. The ankle joint, while less commonly involved, can also suffer significant cartilage damage, particularly in the talar dome.
Biomechanical Implications of Infection
The immediate biomechanical insult in septic arthritis stems from the elevated intra-articular pressure and the enzymatic degradation of articular cartilage. Purulent exudate increases pressure within the confined joint space, potentially compromising the delicate epiphyseal blood supply, especially in the hip. This pressure can also mechanically stretch the joint capsule and ligaments, contributing to joint laxity if chronic.
Articular cartilage, a living tissue, is highly susceptible to damage. Bacterial proteases and lysosomal enzymes released by inflammatory cells (neutrophils) rapidly degrade proteoglycans and collagen fibers, altering the cartilage's mechanical properties. This degradation reduces the cartilage's ability to withstand compressive and shear forces, leading to softening, fibrillation, and ultimately full-thickness loss. Once damaged, articular cartilage has limited capacity for self-repair, resulting in degenerative changes, pain, and functional impairment.
Long-term biomechanical consequences include joint stiffness from fibrosis, osteonecrosis leading to collapse and deformity, growth arrest or stimulation from physeal involvement resulting in limb length discrepancy or angular deformity, and secondary degenerative arthropathy. Early and effective drainage is crucial to reduce intra-articular pressure and remove enzymatic load, thereby preserving the structural integrity and long-term biomechanical function of the joint.
Indications and Contraindications
The decision-making process for the management of pediatric septic arthritis hinges on a rapid and accurate assessment of clinical presentation, laboratory findings, and imaging, aiming to identify the need for surgical intervention.
Operative Indications
The primary indication for operative intervention in pediatric septic arthritis is the presence of purulent material within the joint space, confirmed by aspiration or highly suspected based on clinical parameters and imaging. Specific operative indications include:
* Positive Joint Aspiration: The definitive diagnostic and therapeutic step. Frank pus or turbid fluid on aspiration strongly indicates surgical drainage.
* Failure of Non-Operative Management: If clinical symptoms, inflammatory markers (ESR, CRP), and joint effusion do not improve after 24-48 hours of appropriate intravenous antibiotic therapy and repeated aspiration attempts.
* Hip Septic Arthritis: Considered an absolute orthopedic emergency for surgical drainage. The enclosed nature of the hip capsule and the vulnerability of the femoral head's blood supply make emergent surgical decompression imperative to prevent avascular necrosis.
* Large or Loculated Effusion: When imaging (ultrasound or MRI) demonstrates a significant effusion, particularly with loculations that may not be effectively drained by needle aspiration.
* Presence of Osteomyelitis: If concomitant osteomyelitis is identified adjacent to the joint, open debridement may be necessary to address both components of the infection.
* Uncertain Diagnosis: In cases where the diagnosis remains equivocal after aspiration, but clinical suspicion is high, diagnostic arthrotomy or arthroscopy may be warranted.
* Presence of Systemic Sepsis: If the patient is hemodynamically unstable and the joint is suspected to be the source of sepsis, emergent drainage is indicated.
Non-Operative Indications
Non-operative management typically involves repeated needle aspiration, antibiotic therapy, and immobilization. This approach is generally reserved for specific scenarios:
* Non-Hip Joints with Clear Fluid: If joint aspiration yields serous or serosanguinous fluid, or if initial Gram stain is negative and culture results are pending, especially if inflammatory markers are only mildly elevated and clinical signs are not severe.
* Early, Mild Cases: In very early presentations where the synovial fluid is not frankly purulent, and the child is otherwise well, a trial of intravenous antibiotics and close monitoring with serial aspirations may be considered. However, this carries a higher risk and requires vigilant monitoring.
* Septic Bursitis or Cellulitis: Conditions that can mimic septic arthritis but do not involve the joint space. These are managed primarily with antibiotics, though incision and drainage may be required for large abscesses.
* Joints Amenable to Serial Aspiration: For joints that are easily accessible for repeated needle aspiration (e.g., knee, ankle), multiple aspirations combined with antibiotics may be successful if the effusion is not loculated and the infection resolves quickly.
Operative versus Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Joint Aspiration | Purulent fluid, Gram stain positive | Serous/serosanguinous fluid, Gram stain negative initially |
| Joint Involvement | Hip joint septic arthritis (emergent) | Non-hip joints (knee, ankle, shoulder, elbow) with milder presentation |
| Clinical Course | Worsening clinical status despite antibiotics, systemic sepsis | Rapid improvement with antibiotics, stable vital signs |
| Effusion Size | Large effusion, loculated effusion on imaging | Small to moderate effusion, non-loculated |
| Response to Initial Rx | Failed serial aspiration and antibiotics (>24-48h) | Resolution of symptoms and inflammatory markers post-aspiration and antibiotics |
| Concomitant Issues | Concomitant osteomyelitis requiring debridement | Isolated joint infection without bone involvement |
| Special Cases | Persistent fever, inability to bear weight, severe pain | Mild pain, partial weight-bearing possible (non-hip) |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for optimizing outcomes in pediatric septic arthritis, encompassing diagnostic confirmation, patient stabilization, and precise surgical execution.
Preoperative Diagnostics and Assessment
-
Laboratory Studies:
- Complete Blood Count (CBC): To assess for leukocytosis or anemia.
- Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP): Crucial inflammatory markers. Both are typically elevated and serve as indicators of disease activity and response to treatment. CRP is more acute and responsive than ESR.
- Procalcitonin: Can be useful, especially in differentiating bacterial from viral infections, and as a prognostic marker.
- Blood Cultures: Obtained prior to antibiotic administration, if possible. Positive in a minority of cases (25-50%) but vital for definitive pathogen identification and guiding targeted antibiotic therapy.
- Joint Aspiration: The cornerstone. Performed under sterile conditions. Aspirated fluid sent for:
- Cell Count and Differential: Typically >50,000 WBC/mm³ with >75% neutrophils.
- Gram Stain: Provides rapid presumptive identification of bacteria (positive in 30-70% of cases).
- Bacterial Culture and Sensitivity: Definitive diagnosis and antibiotic guidance.
- Glucose and Protein: Reduced glucose and elevated protein compared to serum are characteristic.
- Crystal Analysis: To rule out crystal-induced arthropathy (rare in children but important for completeness).
- PCR for Kingella kingae: Increasingly recommended, especially in young children, due to its fastidious nature in culture.
-
Imaging Studies:
- Plain Radiographs: Often normal in early septic arthritis. May show soft tissue swelling, joint space widening (due to effusion), or osteopenia with chronicity. Can rule out fracture or obvious osteomyelitis.
- Ultrasound: Highly sensitive for detecting joint effusions, particularly in the hip. Can guide needle aspiration and assess for synovial thickening.
- Magnetic Resonance Imaging (MRI): The most sensitive and specific imaging modality. Can visualize joint effusion, synovial enhancement, cartilage changes, adjacent osteomyelitis, and abscesses. Not always required emergently but invaluable for complex cases or uncertain diagnoses.
- Computed Tomography (CT): Less useful for soft tissue and cartilage but can delineate bony destruction and sequestra in chronic cases or for surgical planning in complex anatomy.
-
Medical Optimization: Address any systemic symptoms of sepsis, stabilize hemodynamics, and initiate broad-spectrum intravenous antibiotics immediately after cultures are obtained, often prior to surgical drainage.
Anesthesia Considerations
Pediatric patients undergoing surgery for septic arthritis often present with pain, fever, and potential dehydration. Anesthetic planning must consider:
* Fluid Management: Correct dehydration and maintain euvolemia.
* Temperature Regulation: Prevent hypothermia, especially in infants.
* Pain Management: Multimodal approach including regional blocks if appropriate.
* Airway Management: Ensure adequate ventilation in a potentially ill child.
Patient Positioning and Surgical Approach Planning
The choice of surgical approach depends on the affected joint, surgeon preference, and patient anatomy. Careful positioning is crucial for adequate exposure and access while protecting neurovascular structures.
-
Hip Septic Arthritis:
- Positioning: Supine on a radiolucent operating table. Ensure adequate exposure for the planned approach. A fracture table is generally not needed.
- Approaches:
- Anterolateral (Smith-Petersen or Watson-Jones): Common for anterior capsular access. Incision centered over the anterior superior iliac spine, extending distally. Internervous plane between tensor fascia lata (superior gluteal nerve) and sartorius (femoral nerve).
- Anterior (Direct Anterior): Incision along the bikini line, medial to ASIS, between sartorius and rectus femoris.
- Posterior (Kocher-Langenbeck): Rarely used for acute drainage unless posterior pathology is suspected, but provides excellent exposure for complex debridement or chronic cases.
-
Knee Septic Arthritis:
- Positioning: Supine with a tourniquet on the proximal thigh. Knee can be flexed or extended.
- Approaches:
- Anteromedial or Anterolateral Arthrotomy: Standard for open drainage. Incision parallel to the patella.
- Arthroscopic Drainage: Increasingly common, especially in older children and adolescents, offering minimally invasive benefits. Requires specific portal placement (e.g., anteromedial, anterolateral) and adequate flow for irrigation.
-
Shoulder Septic Arthritis:
- Positioning: Supine with arm draped free.
- Approaches:
- Anterior (Deltopectoral): Standard approach. Incision in the deltopectoral groove.
- Arthroscopic Drainage: Feasible in older children.
-
Elbow Septic Arthritis:
- Positioning: Supine with arm draped free, or lateral.
- Approaches:
- Posterolateral: Incision over the olecranon, extending distally.
- Medial or Lateral: Depending on pus location.
-
Ankle Septic Arthritis:
- Positioning: Supine with tourniquet.
- Approaches:
- Anteromedial or Anterolateral Arthrotomy: Standard. Incision over the joint line.
Prior to incision, sterile preparation and draping should ensure a wide surgical field. Fluoroscopy may be used to confirm joint entry or drain placement in complex cases.
Detailed Surgical Approach and Technique
The surgical objective in pediatric septic arthritis is thorough drainage of purulent material, debridement of necrotic or infected synovium, and copious irrigation, while minimizing iatrogenic damage to the articular cartilage and physes. The technique varies by joint.
General Principles of Surgical Drainage
- Incision: Positioned to provide direct access to the joint space with minimal soft tissue dissection, respecting vital neurovascular structures and future growth.
- Capsulotomy: Carefully incise the joint capsule to release the pressurized purulent effusion. For the hip, this is crucial for decompressing the femoral head vascularity.
- Drainage and Debridement: Aspirate all pus. Collect samples for Gram stain, culture, and sensitivity. Systematically explore the joint, debriding all necrotic, inflamed, and hyperplastic synovial tissue using curettes, rongeurs, or shavers (arthroscopic). Ensure all loculations are broken down.
- Irrigation: Copiously irrigate the joint with several liters of sterile normal saline. Pulsatile lavage can be effective. Avoid adding antibiotics to the irrigation fluid as this is not proven to be more effective and may contribute to antibiotic resistance.
- Drain Placement: Consider placing a closed suction drain (e.g., Jackson-Pratt) in larger joints or those prone to re-accumulation of fluid, particularly the hip. Drains are typically removed when output is minimal (e.g., <20-30 mL/24h) and serosanguinous.
- Closure: Close the capsule loosely or leave it open to prevent fluid build-up. Close superficial layers and skin meticulously.
Joint-Specific Surgical Approaches
Hip Septic Arthritis
- Anterolateral Approach (Modified Smith-Petersen):
- Incision: Longitudinal incision from the anterior superior iliac spine (ASIS) extending distally 8-10 cm along the course of the sartorius.
- Dissection: Incise skin and subcutaneous tissue. Identify the interval between the tensor fascia lata laterally and the sartorius medially. Retract the sartorius and rectus femoris medially, and tensor fascia lata and gluteus medius/minimus laterally.
- Capsulotomy: The direct anterior aspect of the hip capsule is exposed. A T-shaped or longitudinal capsulotomy is performed to fully decompress the joint and allow thorough exploration.
- Drainage and Debridement: Aspirate pus. Explore the joint with a curved clamp and suction. Perform a limited synovectomy, especially in areas of significant inflammation. Irrigate copiously.
- Drainage: Place a pediatric Jackson-Pratt drain deep to the tensor fascia lata, into the joint space.
- Closure: Close subcutaneous tissue and skin.
Knee Septic Arthritis
-
Open Arthrotomy (Anteromedial or Anterolateral):
- Incision: Longitudinal incision, 4-6 cm, parallel to the patella, either medially or laterally, usually over the area of maximal tenderness or swelling.
- Dissection: Incise skin, subcutaneous tissue, and retinaculum. Carefully incise the joint capsule adjacent to the patella, avoiding damage to the patellar tendon and menisci.
- Drainage and Debridement: Aspirate pus. Explore the suprapatellar pouch, medial and lateral gutters, and the intercondylar notch. Perform limited synovectomy if necessary.
- Irrigation: Copious saline irrigation.
- Drainage: A small drain can be placed if significant effusion is anticipated.
- Closure: Close retinaculum and skin.
-
Arthroscopic Drainage:
- Advantages: Minimally invasive, better visualization, complete lavage.
- Technique: Standard anteromedial and anterolateral portals are established. A large-bore inflow cannula is inserted through one portal, and a scope through the other. A motorized shaver is used to debride inflamed synovium. Copious irrigation is performed until the fluid is clear. Additional posteromedial or posterolateral portals may be needed for posterior compartment drainage in specific cases.
- Drainage: Usually not required after arthroscopic drainage if the lavage is thorough.
Shoulder Septic Arthritis
- Anterior (Deltopectoral) Approach:
- Incision: Longitudinal incision in the deltopectoral groove.
- Dissection: Identify the interval between the deltoid and pectoralis major. Retract the cephalic vein laterally. Incise the clavipectoral fascia. The subscapularis tendon and shoulder capsule are exposed.
- Capsulotomy: Longitudinal incision in the capsule parallel to the subscapularis.
- Drainage and Debridement: Aspirate pus, explore, debride, and irrigate.
- Drainage: Place a drain.
- Closure: Layered closure.
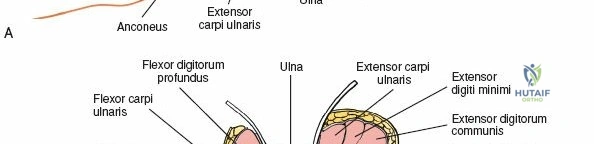
Elbow Septic Arthritis
- Posterolateral Approach:
- Incision: Longitudinal incision over the lateral epicondyle, extending distally.
- Dissection: Incise subcutaneous tissue. Identify the common extensor origin. Access the joint through the interval between the anconeus and the extensor carpi ulnaris, or directly through the posterolateral capsule.
- Drainage and Debridement: Aspirate pus, explore the joint, debride synovium, irrigate.
- Drainage: Drain placement if needed.
- Closure: Layered closure.
Ankle Septic Arthritis
- Anteromedial or Anterolateral Approaches:
- Incision: Longitudinal incision over the tibiotalar joint line, either anteromedially (between tibialis anterior and extensor hallucis longus) or anterolaterally (between extensor digitorum longus and peroneus tertius).
- Dissection: Careful dissection to avoid neurovascular structures (dorsalis pedis artery, deep peroneal nerve). Incise the capsule.
- Drainage and Debridement: Aspirate, explore, debride, and irrigate.
- Drainage: Drain placement if needed.
- Closure: Layered closure.
Throughout all surgical procedures, meticulous hemostasis is maintained, and efforts are made to protect the physeal plates and articular cartilage to minimize long-term sequelae.
Complications and Management
Despite prompt and aggressive management, pediatric septic arthritis can lead to a range of severe complications, necessitating vigilant monitoring and strategic salvage interventions.
Common Complications and Incidence
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Avascular Necrosis (AVN) of Epiphysis | 10-50% (Hip) | Early: Joint decompression, antibiotics. Late: Physiotherapy, bracing to protect joint. Severe: Osteotomies (femoral/pelvic) to improve coverage, reconstructive procedures (e.g., vascularized fibular graft), total hip arthroplasty (THA) in adulthood for severe degenerative disease (though rare in pediatric context, considered for mature skeleton). |
| Growth Plate Arrest/Disturbance | 5-20% (all joints) | Mild: Observation. Moderate: Epiphysiodesis on contralateral limb for length equalization, guided growth (hemiepiphysiodesis) for angular deformity. Severe: Corrective osteotomies, limb lengthening procedures. |
| Articular Cartilage Destruction | High (variable) | Acute: Thorough debridement, antibiotics. Chronic: Activity modification, bracing, physiotherapy. Severe: Debridement, microfracture, osteochondral autograft transplantation (OATS), allograft transplantation, ultimately arthrodesis or arthroplasty (for mature skeletons). |
| Chronic Osteomyelitis | 2-10% | Extensive surgical debridement (sequestrectomy), prolonged targeted antibiotic therapy (IV and oral), bone grafting, external fixation for stability, reconstructive flaps. |
| Joint Stiffness/Contracture | 10-30% | Aggressive physical therapy, serial casting, dynamic splinting, manipulation under anesthesia. Resistant: Capsulectomy, release of adhesions. |
| Pathologic Dislocation/Subluxation | 5-15% (Hip) | Closed or open reduction, often with capsulorrhaphy. Salvage involves reconstructive osteotomies (e.g., Salter, Dega, Pemberton) to improve hip stability and coverage, or rarely, arthrodesis. |
| Recurrence of Infection | 2-5% | Re-aspiration, repeat surgical drainage and debridement, re-evaluation of antibiotic regimen, investigation for retained foreign body or immunocompromised state. |
| Sepsis and Death | Rare (<1%) | Intensive care support, aggressive fluid resuscitation, vasopressors, broad-spectrum antibiotics, source control (urgent drainage). |
Management Strategies for Complications
-
Avascular Necrosis (AVN) of the Femoral Head: Early recognition is key. Regular clinical and radiographic follow-up is critical. Management varies from observation for mild cases to femoral and/or pelvic osteotomies to improve coverage and concentric reduction for more severe deformities. In cases of severe collapse and non-reconstructible anatomy, arthrodesis or even total hip arthroplasty in adulthood may be considered, though challenging in the pediatric population.
-
Growth Plate Arrest/Disturbance: Identified through serial limb length discrepancy measurements and radiographs. Mild discrepancies (<2 cm) may be observed. Greater discrepancies or angular deformities require surgical intervention such as contralateral epiphysiodesis, guided growth techniques (e.g., hemiepiphysiodesis with plates or screws), or corrective osteotomies and limb lengthening procedures using internal or external fixation.
-
Articular Cartilage Destruction: Leads to early degenerative changes. Acute management focuses on thorough debridement. Long-term management involves activity modification, physiotherapy, and symptomatic treatment. For focal defects, microfracture, osteochondral autograft transplantation (OATS), or allograft may be options in older children or adolescents. For widespread destruction, arthrodesis or prosthetic replacement (in skeletally mature patients) might be the last resort.
-
Chronic Osteomyelitis: Requires aggressive surgical debridement of all infected and necrotic bone (sequestrectomy) until healthy bleeding bone is reached. This is often combined with prolonged, culture-directed intravenous and oral antibiotic therapy, sometimes for months. Bone grafting may be necessary to fill defects, and vascularized flaps can be considered for large soft tissue defects.
-
Joint Stiffness/Contracture: Primarily managed with intensive physical therapy, stretching exercises, and dynamic splinting. Serial casting or manipulation under anesthesia may be necessary for resistant contractures. Surgical release of adhesions or capsulotomy may be performed in refractory cases.
-
Pathologic Dislocation/Subluxation: Most common in the hip. Initial management is closed or open reduction. If the hip is unstable or recurrently dislocates due to acetabular or femoral head deformity, reconstructive osteotomies (e.g., Salter innominate osteotomy, Dega osteotomy, Pemberton osteotomy for the pelvis; femoral varus derotation osteotomy) are often required to improve joint stability and coverage.
-
Recurrence of Infection: Demands immediate re-evaluation, including repeat aspiration, imaging, and laboratory studies. Often necessitates repeat surgical drainage and debridement. The antibiotic regimen should be reassessed based on new cultures and sensitivities. Investigation for atypical organisms or immunocompromised states should be considered.
Prevention of complications starts with early diagnosis, aggressive surgical intervention, appropriate antibiotic therapy, and diligent postoperative monitoring. Long-term follow-up is critical for identifying and managing delayed sequelae.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is an integral component of comprehensive management for pediatric septic arthritis, aiming to restore joint function, prevent stiffness, and facilitate recovery while ensuring adequate infection control. Protocols must be individualized based on the joint involved, extent of damage, and patient's age and compliance.
Acute Postoperative Period (Days 0-7)
- Antibiotic Therapy: Continue broad-spectrum intravenous antibiotics initiated preoperatively, transitioning to targeted, culture-sensitive antibiotics once results are available. Duration is typically 2-4 weeks intravenously, followed by oral antibiotics for another 2-4 weeks, guided by clinical response and normalization of inflammatory markers (ESR, CRP). Total duration usually ranges from 4 to 6 weeks, but can be longer for osteomyelitis or resistant organisms.
- Pain Management: Aggressive pain control using multimodal analgesia (acetaminophen, NSAIDs, opioids as needed). Regional blocks can be beneficial immediately post-op. Adequate pain control facilitates early mobilization.
- Wound Care and Drain Management: Monitor surgical incision for signs of infection, dehiscence, or excessive drainage. Drains, if placed, are typically removed when output is minimal (<20-30 mL/24h) and serous.
- Joint Rest/Immobilization:
- Hip: Initially, gentle skin traction or a spica cast may be applied for comfort and to maintain joint reduction in cases of instability or severe inflammation. However, prolonged immobilization is generally avoided to prevent stiffness.
- Knee, Ankle, Elbow, Shoulder: Brief period of splinting or casting for comfort, usually for 3-7 days.
- Early Range of Motion (ROM): As soon as comfort allows, gentle passive or active-assisted range of motion exercises are initiated to prevent adhesions and stiffness. This is particularly crucial for the hip.
- Hip: Gentle passive flexion, extension, abduction, and rotation within the pain-free range.
- Knee: Continuous passive motion (CPM) machine may be used, or gentle active/passive flexion and extension exercises.
- Other Joints: Similarly, gentle ROM exercises tailored to the specific joint.
Subacute Rehabilitation Phase (Weeks 1-6)
- Progressive Mobilization: Gradually increase the intensity and duration of ROM exercises.
- Weight Bearing: Non-weight bearing or touch-down weight bearing for 2-4 weeks, especially for lower extremity joints like the hip and knee, to protect healing cartilage and bone. Progress to partial and then full weight bearing as tolerated and guided by clinical and radiographic assessment. Crutches or a walker are used.
- Strengthening: Introduce isometric and then isotonic strengthening exercises for muscles surrounding the affected joint. Focus on core stability and hip abductor strength for lower extremity involvement.
- Physical Therapy and Occupational Therapy:
- Physical Therapy: Tailored exercises to improve strength, flexibility, balance, and proprioception. Address gait deviations.
- Occupational Therapy: For upper extremity involvement, focus on fine motor skills and activities of daily living.
- Monitoring for Complications: Continue monitoring inflammatory markers (ESR, CRP) weekly until normalization. Clinically assess for pain, swelling, fever, and signs of recurrent infection. Radiographs are repeated periodically to monitor for AVN, growth plate disturbances, or osteomyelitis.
Long-Term Rehabilitation and Follow-up (Months to Years)
- Activity Progression: Gradually return to age-appropriate activities and sports. High-impact activities may need to be limited initially or permanently if significant joint damage has occurred.
- Continued Monitoring: Long-term follow-up is crucial, especially for hip septic arthritis, to detect delayed complications.
- Radiographic Surveillance: Periodic radiographs for 1-2 years, or longer, to assess for AVN, growth disturbances, limb length discrepancies, and early degenerative changes. MRI may be indicated for specific concerns.
- Clinical Assessment: Monitor joint function, pain levels, and overall growth and development.
- Addressing Sequelae: If complications like AVN, growth arrest, or significant functional limitations arise, specialized interventions (e.g., osteotomies, limb lengthening, bracing) will be incorporated into the rehabilitation plan. Psychological support for children coping with chronic conditions or disabilities should also be considered.
Successful rehabilitation hinges on a multidisciplinary approach involving orthopedic surgeons, infectious disease specialists, physical therapists, occupational therapists, and pediatricians, with active engagement from the patient and family.
Summary of Key Literature and Guidelines
The management of pediatric septic arthritis is continually refined by robust clinical research, meta-analyses, and evidence-based guidelines from leading orthopedic societies. The core principles of early diagnosis, prompt surgical drainage, and targeted antibiotic therapy remain sacrosanct.
Key Literature Insights
- Early Diagnosis and Intervention: Numerous studies underscore the critical importance of early diagnosis and surgical decompression, especially for hip septic arthritis, to mitigate the risk of devastating complications such as avascular necrosis and growth plate damage. Delays beyond 24-48 hours significantly worsen outcomes.
- Pathogen Spectrum Evolution: The recognition of Kingella kingae as a significant pathogen in young children (6 months to 4 years) has been a pivotal development. This organism is difficult to culture using standard methods, leading to increased reliance on PCR testing of synovial fluid. Treatment regimens have been adapted to cover this pathogen.
- Role of Inflammatory Markers: ESR and CRP are consistently identified as highly sensitive, though non-specific, markers for diagnosis and monitoring treatment response. Rapid decline in CRP is a strong indicator of successful treatment, while persistent elevation should prompt re-evaluation for inadequate drainage or resistant infection.
- Meta-Analyses and Risk Factors: As highlighted in the initial prompt, rigorous meta-analyses provide crucial insights into risk factors such as age and sex, enabling clinicians to refine their diagnostic suspicion. Critically evaluating heterogeneity and bias in these studies ensures that clinical decisions are based on the strongest available evidence. For instance, while male sex has been a frequently cited risk factor, meta-analyses clarify the extent and statistical significance of this association across diverse populations.
- Arthroscopic vs. Open Drainage: Literature supports arthroscopic drainage for suitable joints (e.g., knee, shoulder) in older children, demonstrating comparable efficacy to open arthrotomy with potential benefits of smaller incisions, less pain, and faster recovery. However, for the hip, open arthrotomy remains the standard, especially in infants, due to the critical need for complete decompression and debridement.
- Antibiotic Duration: Evidence supports a total antibiotic course of 4-6 weeks, with an initial intravenous phase (2-4 weeks) followed by oral therapy, guided by clinical response and normalization of inflammatory markers. Prolonged courses beyond this are generally reserved for complicated cases, such as concomitant osteomyelitis or immunocompromised patients.
Guidelines and Consensus Recommendations
Major orthopedic organizations, such as the Pediatric Orthopaedic Society of North America (POSNA) and the American Academy of Orthopaedic Surgeons (AAOS), provide guidelines and consensus statements that inform best practices:
- Diagnostic Algorithm: A consistent approach emphasizing immediate joint aspiration for suspected septic arthritis. Synovial fluid analysis (cell count, Gram stain, culture, PCR) is paramount. Blood cultures and inflammatory markers are adjuncts.
- Emergency Management: All guidelines stress that hip septic arthritis is an orthopedic emergency requiring immediate surgical decompression and drainage to prevent devastating long-term sequelae.
- Antibiotic Regimens: Initial broad-spectrum intravenous antibiotics are recommended, covering Staphylococcus aureus, Group A Streptococcus, and Kingella kingae in younger children, and broadening coverage for neonates and immunocompromised patients. Antibiotics are then streamlined based on culture and sensitivity results.
- Postoperative Care: Emphasis on early range of motion, pain control, and judicious use of immobilization. Close clinical and laboratory follow-up is recommended to monitor for treatment response and identify potential complications. Long-term radiographic surveillance, particularly for the hip, is crucial to detect delayed sequelae like AVN or growth disturbances.
- Role of Imaging: Ultrasound for effusion detection, MRI for comprehensive assessment of joint and adjacent bone.
The critical meta-analysis of risk factors, as detailed in our tables S3, S4, and S5, serves to strengthen the evidence base for these guidelines, ensuring that our understanding of pediatric septic arthritis is robust, current, and applied with maximum clinical efficacy. Continuous evaluation of new data and refinement of treatment protocols remains essential to improve outcomes for these vulnerable patients.
