Mastering Elbow Arthroscopy: A Comprehensive Intraoperative Guide
Key Takeaway
This masterclass provides an exhaustive, real-time guide to elbow arthroscopy. Fellows will learn critical neurovascular anatomy, meticulous patient positioning, and granular, step-by-step intraoperative execution. We cover precise instrument handling, portal creation, and essential pearls to navigate complex elbow pathologies safely and effectively, emphasizing complication prevention and management.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the definitive guide on elbow arthroscopy. The evolution of elbow arthroscopy over the past three decades represents one of the most profound advancements in orthopedic surgery. Initially relegated to a purely diagnostic role due to the intimidating proximity of vital neurovascular structures, the procedure has rapidly transformed into a sophisticated therapeutic modality. Today, we utilize arthroscopy for complex reconstructive procedures, capsular releases, osteochondritis dissecans (OCD) management, and fracture fixation. However, this transition from open to minimally invasive techniques demands an uncompromising, unparalleled understanding of intricate three-dimensional anatomy and meticulous intraoperative technique.
Unlike the knee or shoulder, the elbow's compact nature and the immediate adjacency of critical nerves and vessels elevate the surgical stakes exponentially. The margin for error is measured in millimeters. A minor deviation in portal placement or a momentary lapse in spatial awareness can result in catastrophic, irreversible neurovascular compromise. Therefore, mastering elbow arthroscopy is not merely about acquiring technical dexterity; it is about cultivating a profound respect for the regional anatomy and adhering strictly to established safety protocols. Our objective in this chapter is to provide you with a comprehensive, immersive experience, guiding you through every critical decision, anatomical landmark, and surgical maneuver required to execute this procedure safely and effectively.
The epidemiology of elbow pathologies amenable to arthroscopic intervention is diverse, encompassing both athletic populations and the aging demographic. Overhead athletes, particularly baseball pitchers and gymnasts, frequently present with valgus extension overload, posteromedial impingement, and capitellar OCD lesions. Conversely, the older population more commonly requires arthroscopic management for degenerative joint disease, primary osteoarthritis, and post-traumatic arthrofibrosis. Recognizing the specific demographic and patho-mechanical etiology is crucial, as it dictates not only the surgical approach but also the preoperative planning and postoperative rehabilitation trajectory.
As you embark on mastering this technique, you must acknowledge the steep learning curve associated with elbow arthroscopy. The initial phases of your training should focus heavily on cadaveric dissection and supervised portal placement. The transition to independent practice requires a systematic, unvarying approach to patient positioning, joint insufflation, and sequential compartment evaluation. By internalizing the principles detailed in this chapter, you will mitigate the inherent risks and harness the full therapeutic potential of elbow arthroscopy, ultimately optimizing functional outcomes for your patients.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the patient's skin, a three-dimensional, almost tactile understanding of the elbow's surrounding neurovascular anatomy is absolutely paramount. This is the crucible where surgical competence is tested, and where the vast majority of devastating complications arise if the surgeon is not acutely vigilant.
Neurovascular Relationships and the No-Go Zones
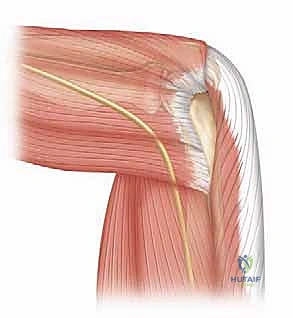
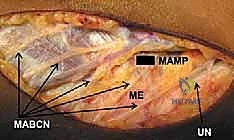
The radial nerve is notoriously vulnerable, particularly during the establishment of anterolateral portals. Anatomical studies have consistently demonstrated that it can pass within a mere 6 mm of the joint capsule in a 90-degree flexed, insufflated elbow. Crucially, the distance from the arthroscopic sheath to the radial nerve averages 4.9 mm in flexion (ranging from 2 to 10 mm) versus a frighteningly close 1.4 mm in extension (ranging from 0 to 4 mm) for the distal anterolateral portal. The radial nerve courses anterior to the lateral epicondyle, deep to the brachioradialis and extensor carpi radialis longus (ECRL), before bifurcating into its superficial sensory and deep motor (posterior interosseous nerve) branches. Our anterolateral portals typically traverse the muscular interval between the brachioradialis and ECRL, demanding blunt dissection to avoid transection.
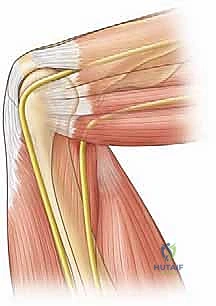
Located anteromedially, the median nerve also lies in perilous proximity to our working space, passing within 6 mm of the joint capsule in a flexed, insufflated elbow. While it is, on average, 3 mm further from the capsule than the radial nerve, it remains highly susceptible to iatrogenic injury. The median nerve passes deep to the bicipital aponeurosis and descends between the two heads of the pronator teres. Anteromedial portals must be placed with extreme caution in this vicinity, utilizing a strict "nick and spread" technique with a hemostat to protect the nerve and the adjacent brachial artery, which runs parallel to it in the cubital fossa.
The ulnar nerve is arguably the most vulnerable structure in the entire elbow, essentially lying directly on the joint capsule posteromedially, particularly within the confines of the cubital tunnel. The tunnel is formed by the medial epicondyle anteriorly, the olecranon laterally, and the arcuate ligament (Osborne's fascia) superficially. Its superficial, fixed location makes it highly susceptible to direct mechanical trauma during posteromedial portal placement, as well as indirect compression from fluid extravasation if outflow is not meticulously managed.
The Protective Effect of Flexion and Insufflation
To navigate these treacherous anatomical waters safely, we rely heavily on two fundamental biomechanical principles: elbow flexion and capsular insufflation. Portal placement is significantly safer when the elbow is flexed to exactly 90 degrees compared to full extension. Flexion dynamically alters the regional anatomy, increasing the critical nerve-to-portal distances. Specifically, flexion increases the lateral distance to the radial nerve (from 3.5 to 5.1 mm) and the medial distance to the median nerve (from 1.4 to 5.6 mm). Flexion is safety; extension is peril.
Maximal joint distention with sterile saline prior to establishing any portals is the second non-negotiable safety measure. Insufflation significantly increases the bone-to-nerve distances (averaging 12 mm for the median nerve, 6 mm for the radial nerve, and 1 mm for the ulnar nerve), effectively creating a protective fluid cushion that pushes the neurovascular structures away from the advancing trocar. However, it is critical to understand that the capsule-to-nerve distance changes very little with insufflation; the nerve moves outward with the distended capsule. Furthermore, this protective fluid effect is entirely negated if the elbow is allowed to fall into extension.
Finally, the strategic selection of portal sites plays a major role in risk mitigation. For anterior access, more proximal portals (such as the proximal anteromedial and proximal anterolateral portals) consistently offer a greater nerve-to-portal distance than their more distal counterparts. This proximal shift enhances safety, especially regarding the radial nerve laterally and the median nerve medially, by taking advantage of the diverging course of these nerves as they travel distally into the forearm.
Exhaustive Indications and Contraindications
The decision to proceed with elbow arthroscopy must be rooted in a rigorous clinical evaluation, balancing the potential therapeutic benefits against the inherent risks of the procedure. Patient selection is the ultimate determinant of surgical success.
Diagnostic and Therapeutic Indications
Therapeutic indications for elbow arthroscopy have expanded dramatically. The most common indication remains the extraction of intra-articular loose bodies, often secondary to synovial chondromatosis, osteoarthritis, or trauma. Arthroscopy provides unparalleled visualization of the anterior and posterior compartments, allowing for complete clearance of mechanical blocks to motion. Furthermore, the arthroscopic management of osteochondritis dissecans (OCD) of the capitellum has become the gold standard, permitting precise debridement, marrow stimulation (microfracture), or internal fixation of unstable lesions with minimal morbidity.
Arthroscopic contracture release (arthrolysis) is an advanced indication that yields excellent results in the hands of an experienced surgeon. By systematically resecting the anterior and posterior capsule, removing impinging osteophytes from the coronoid and olecranon fossae, and releasing intra-articular adhesions, surgeons can restore functional range of motion in patients with post-traumatic or degenerative arthrofibrosis. Additionally, arthroscopy is highly effective for treating lateral epicondylitis (tennis elbow) that has failed conservative management, allowing for precise debridement of the extensor carpi radialis brevis (ECRB) origin from within the joint.
Other emerging indications include the evaluation and treatment of subtle instability patterns, such as posterolateral rotatory instability (PLRI), where the arthroscope can confirm the diagnosis via the "drive-through" sign before proceeding to open or arthroscopic ligamentous reconstruction. Arthroscopically assisted fracture fixation, particularly for radial head and capitellar fractures, is also gaining traction, offering the benefit of direct articular reduction without the soft tissue stripping associated with traditional open approaches.
Absolute and Relative Contraindications
Despite its versatility, elbow arthroscopy is not universally applicable. Absolute contraindications include active localized soft tissue or intra-articular infection, which risks systemic dissemination or catastrophic joint destruction. Additionally, any condition that physically prevents adequate capsular distention—such as severe, bridging heterotopic ossification (HO) or profound extra-articular contractures—renders the procedure unacceptably dangerous, as the protective fluid cushion cannot be established, placing the neurovascular structures at extreme risk during trocar insertion.
Relative contraindications require careful preoperative deliberation. A history of prior elbow trauma or complex open surgery (particularly ulnar nerve transposition) significantly alters the normal neurovascular anatomy. In such cases, the standard safe zones for portal placement are no longer reliable. If arthroscopy is deemed necessary in a patient with a prior ulnar nerve transposition, a mini-open incision to visually identify and protect the nerve is mandatory before establishing medial portals.
Complex Regional Pain Syndrome (CRPS) is another strong relative contraindication. The surgical trauma of arthroscopy, combined with fluid extravasation, can severely exacerbate the dystrophic pain cycle, leading to devastating postoperative stiffness and hyperalgesia. Finally, severe distortion of the bony anatomy from malunited fractures may disorient the surgeon intraoperatively, making navigation perilous and increasing the risk of iatrogenic cartilage damage or instrument breakage.
| Category | Specific Condition | Rationale / Clinical Consideration |
|---|---|---|
| Indications | Loose Bodies / Synovial Chondromatosis | Excellent visualization for complete extraction; resolves mechanical catching. |
| Osteochondritis Dissecans (OCD) | Allows for microfracture, debridement, or precise in-situ fixation. | |
| Arthrofibrosis / Contracture | Facilitates capsular release and osteophyte resection to restore ROM. | |
| Recalcitrant Lateral Epicondylitis | Permits targeted intra-articular debridement of the ECRB origin. | |
| Contraindications | Active Infection (Absolute) | Risk of systemic spread and severe septic arthritis. |
| Inability to Distend Capsule (Absolute) | Loss of protective fluid cushion; extreme risk to neurovascular structures. | |
| Prior Ulnar Nerve Transposition (Relative) | Altered anatomy requires open exposure of the nerve prior to medial portal placement. | |
| Complex Regional Pain Syndrome (Relative) | High risk of exacerbating the pain cycle and causing profound postoperative stiffness. |
Pre-Operative Planning, Templating, and Patient Positioning
A successful arthroscopy begins long before the patient enters the operating theater. It requires meticulous preparation, advanced imaging analysis, and a deliberate strategy for patient positioning and instrumentation.
Clinical Evaluation and Advanced Imaging
A thorough history and physical examination are foundational. We must actively search for clues that might alter our surgical approach, such as previous incisions, signs of ulnar neuropathy, or a history of significant trauma. Routine radiographs are mandatory, including a true lateral, a standard AP, and an AP view of both the distal humerus and proximal forearm if motion loss prevents full extension. Specialized views are often required: the Cubital Tunnel View (AP projection in maximal flexion) is essential for assessing medial epicondyle morphology, while the Capitellum View (AP of the ulna with 45 degrees flexion) provides a tangential look at OCD lesions.
Advanced imaging is invaluable for complex cases. High-resolution Computed Tomography (CT) with 3D reconstructions is the imaging modality of choice when planning a contracture release, as it provides precise spatial localization of impinging osteophytes in the coronoid and olecranon fossae. Magnetic Resonance Imaging (MRI), particularly MR arthrography, is superior for evaluating soft tissue constraints, cartilage integrity, and the stability of OCD lesions.
Intraoperative fluoroscopy must be readily available and properly positioned before prepping and draping. It is absolutely essential if we plan on drilling, pinning, or performing internal fixation of lesions like OCD or fractures. The C-arm should be brought in from the contralateral side of the table to allow unhindered access to the operative elbow.
Anesthesia and Instrumentation Considerations
General anesthesia is typically preferred for elbow arthroscopy. It provides complete muscle relaxation, which is crucial for safe joint manipulation, maximal capsular distention, and unhindered portal placement. While regional anesthesia (supraclavicular or axillary blocks) can be utilized, many surgeons prefer to assess the patient's baseline neurovascular status in the immediate recovery period before administering regional blockade, particularly after complex contracture releases where nerve stretch injuries are a risk.
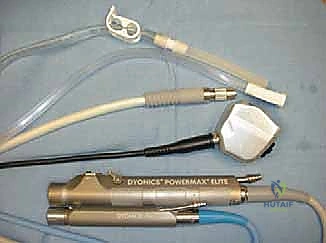
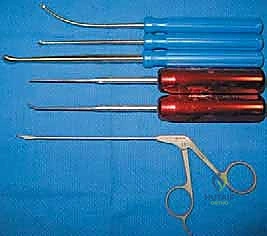
The instrumentation required for elbow arthroscopy is highly specialized. Our primary workhorse is a standard 4.0-mm, 30-degree offset arthroscope. In exceptionally tight joints or pediatric patients, a 2.7-mm scope may be necessary. Crucially, we must utilize an arthroscope sheath without side flow ports. Side ports allow pressurized fluid to escape directly into the surrounding soft tissues, rapidly leading to massive extravasation and potential compartment syndrome.

Beyond the scope, the basic tray must include an 18-gauge spinal needle for joint distention, a fine hemostat for blunt portal dissection, and Wissinger rods for switching portals safely. Specialized instruments, such as curved and straight arthroscopic retractors, curettes, and specific hand biters, are essential for safe anterior capsular resection during contracture release, allowing the surgeon to cut tissue while simultaneously protecting the anterior neurovascular bundle.

Patient Positioning: Supine, Lateral, and Prone Options
The choice of patient position dictates the flow of the surgery and influences the ease of access to different compartments. We primarily utilize four positions, each with distinct biomechanical advantages.
The Supine Cross-Body Position involves placing the patient supine with the operative arm draped across the chest. This is highly effective when combining a less demanding arthroscopic procedure with an open surgery (e.g., arthroscopic debridement followed by open ligament reconstruction), as it prevents the need for intraoperative repositioning. However, the elbow is not rigidly stabilized, making complex procedures more challenging and increasing the risk of inadvertent movement during delicate maneuvers.

The Supine Suspended Position utilizes a traction device (typically sterile finger traps on the index and long fingers) connected to a boom, suspending the arm vertically. This provides excellent, rigid stabilization of the elbow at 90 degrees of flexion, optimizing the safe zones for anterior portal placement. It allows for seamless transition between the anterior and posterior compartments and provides excellent access for the C-arm.

The Lateral Decubitus Position places the patient on their non-operative side with the operative arm resting over a bolstered post or suspended. This position offers unparalleled access to the posterior compartment and is favored by many surgeons for extensive posterior osteophyte resection or triceps pathology. It also allows gravity to pull the anterior neurovascular structures away from the joint capsule, theoretically increasing safety during anterior work.

The Prone Position is an excellent alternative that provides exceptional stability and access to the posterior elbow. The patient is prone, and the arm hangs freely over the side of the table over a padded post, naturally resting at 90 degrees of flexion. This position is highly ergonomic for the surgeon when working in the posterior compartment and eliminates the need for complex suspension systems, though airway management requires an experienced anesthesia team.

Step-by-Step Surgical Approach and Fixation Technique
Executing an elbow arthroscopy requires a choreographed, systematic approach. Haphazard portal placement or random joint exploration invites disaster. We must adhere to a strict sequence of distention, portal establishment, and compartmental evaluation.
Joint Distension and Portal Establishment
The procedure invariably begins with maximal joint distention. With the elbow flexed to 90 degrees, an 18-gauge spinal needle is introduced through the lateral "soft spot"—the triangle formed by the lateral epicondyle, the radial head, and the tip of the olecranon. We inject 20 to 30 cc of sterile saline until backflow is brisk and the capsule is tense. This step is critical; it displaces the anterior neurovascular bundle away from the joint line, creating our safe working margin.
Our primary viewing portal is typically the Proximal Anteromedial (PAM) Portal. Located 2 cm proximal and 1 cm anterior to the medial epicondyle, it offers an expansive view of the anterior articulation. A superficial skin incision is made with a #11 blade. Crucially, we utilize a small hemostat to bluntly dissect down to the capsule—the "nick and spread" technique—pushing the cutaneous nerves and the median nerve/brachial artery complex safely aside. A blunt trocar is then directed toward the center of the joint, aiming for the radial head.

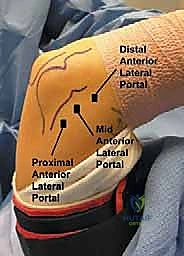
Once the PAM portal is established and the scope is inserted, we create the Proximal Anterolateral (PAL) Portal under direct intra-articular visualization. An 18-gauge spinal needle is inserted 2 cm proximal and 1 cm anterior to the lateral epicondyle, aiming toward the center of the joint. Once the optimal trajectory is confirmed visually, the skin is incised, blunt dissection is performed, and the working cannula is introduced. This portal provides excellent access for instrumentation of the coronoid and anterior capsule.

Anterior Compartment Diagnostic Sweep
With both anterior portals established, we commence a systematic diagnostic sweep. Starting from the PAM portal, we evaluate the coronoid process, the anterior capsule, and the trochlea. We look for loose bodies hiding in the coronoid fossa, signs of capsular contracture, or chondral defects on the trochlear ridge. The scope is then swept laterally to inspect the radial head and the capitellum.
The radiocapitellar joint is a common site for pathology, particularly OCD lesions in young athletes or degenerative wear in older patients. We dynamically assess the joint by pronating and supinating the forearm, observing the tracking of the radial head against the capitellum. Any loose bodies or unstable chondral flaps are meticulously debrided using a motorized shaver introduced through the PAL portal.

During anterior work, fluid management is paramount. The elbow capsule is small (capacity ~25-30 cc), and prolonged high-pressure inflow will inevitably lead to fluid extravasation into the forearm compartments. We must frequently vent the joint, maintain inflow pressures strictly below 40 mmHg, and utilize gravity flow whenever possible to minimize the risk of iatrogenic compartment syndrome.
Posterior Compartment Access and Evaluation
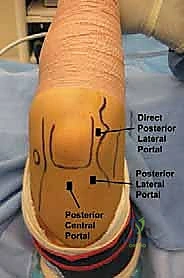
After completing the anterior work, the fluid is evacuated, and attention is turned posteriorly. The elbow is maintained at 90 degrees of flexion. The primary portals for the posterior compartment are the Posterolateral Portal (located just proximal to the tip of the olecranon, off the lateral border of the triceps) and the Posterior Central Portal (located directly through the triceps tendon, 3 cm proximal to the olecranon tip).
Using the same "nick and spread" technique, the posterolateral portal is established first for viewing. The posterior central portal is then created under direct vision using a spinal needle for localization. The posterior sweep begins with an evaluation of the olecranon fossa, looking for impinging osteophytes or loose bodies that limit extension.

We then evaluate the medial and lateral gutters. The posteromedial gutter is particularly critical; aggressive shaver use here can easily compromise the ulnar nerve, which lies just outside the thin capsule. Debridement in this area must be performed with the shaver blade facing away from the capsule at all times. Resection of olecranon tip osteophytes (valgus extension overload) is performed with a burr, dynamically checking extension to ensure complete decompression without violating the articular surface of the trochlea.