Elbow Fracture-Dislocation: A Masterclass in Complex Instability Reconstruction

Key Takeaway
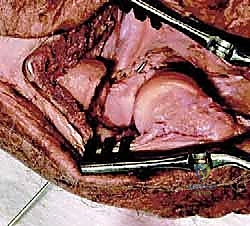
Join us in the OR for an immersive masterclass on open reduction and internal fixation of complex elbow fracture-dislocations. We'll meticulously reconstruct the elbow, addressing coronoid and radial head fractures, and repairing ligamentous injuries. This guide covers critical anatomy, step-by-step intraoperative techniques, neurovascular precautions, and strategies for achieving concentric stability and early motion, crucial for preventing long-term stiffness and recurrent instability.
Comprehensive Introduction and Patho-Epidemiology
The management of complex elbow instability, colloquially and aptly termed the "terrible triad" of the elbow, represents one of the most formidable challenges in orthopaedic traumatology. This injury pattern is defined by the simultaneous occurrence of an elbow dislocation, a fracture of the radial head, and a fracture of the coronoid process of the ulna. Historically, these injuries were fraught with dismal outcomes, primarily due to a lack of understanding regarding the intricate interplay of the elbow's bony and ligamentous stabilizers. Patients frequently suffered from chronic, debilitating instability, profound stiffness, and early-onset post-traumatic osteoarthritis. Today, however, the paradigm has shifted. Through a meticulous, protocol-driven surgical approach, we can systematically reconstruct the osteoarticular and ligamentous anatomy, thereby restoring concentric stability and permitting the early, protected motion that is absolutely critical for functional recovery.
The pathogenesis of the terrible triad is invariably linked to high-energy trauma. The classic mechanism of injury involves a fall onto an outstretched hand (FOOSH), typically with the arm in a position of extension and supination. As the axial load is transmitted through the forearm to the elbow, a valgus moment is introduced, coupled with a posterolateral rotatory force. This complex application of forces initiates a sequential cascade of soft tissue and bony failure, classically described by O'Driscoll as the "circle of Horii." The disruption typically begins on the lateral side with the avulsion or rupture of the lateral collateral ligament (LCL) complex, proceeds anteriorly to shear the coronoid process against the trochlea, impacts the radial head against the capitellum causing it to fracture, and finally culminates in the disruption of the medial collateral ligament (MCL) complex as the elbow frankly dislocates posteriorly.

Epidemiologically, these fracture-dislocations exhibit a bimodal distribution. They are frequently observed in younger, active males following high-velocity injuries such as motor vehicle collisions, falls from significant heights, or contact sports. Conversely, a secondary peak occurs in older, osteopenic females who sustain these injuries from simple ground-level falls. Regardless of the patient demographic, the overarching therapeutic mandate remains identical: to achieve a stable, concentric reduction of both the ulnohumeral and radiocapitellar articulations. Failure to recognize the severity of this injury or to adequately address every component of the triad invariably condemns the patient to a cycle of recurrent subluxation, accelerated articular wear, and profound functional impairment.
Detailed Surgical Anatomy and Biomechanics
Osteoarticular Stabilizers
A profound comprehension of elbow biomechanics is the bedrock upon which successful reconstruction is built. The elbow joint is a highly constrained hinge, deriving its stability from a synergistic combination of articular congruity and capsuloligamentous tension. The primary static stabilizer is the ulnohumeral joint. The highly congruent, saddle-shaped greater sigmoid notch of the ulna tightly captures the humeral trochlea. The coronoid process serves as the vital anterior buttress of this articulation. It prevents posterior subluxation of the ulna and serves as the insertion footprint for the anterior bundle of the MCL and the anterior capsule. Even seemingly innocuous Type I (tip) fractures of the coronoid, according to the Regan and Morrey classification, represent significant capsular avulsions that destabilize the joint when combined with radial head and lateral ligamentous disruptions.
The radiocapitellar joint functions as a crucial secondary stabilizer. While it facilitates forearm pronation and supination, its primary biomechanical role in the context of trauma is to resist valgus stress and longitudinal radioulnar translation. When the MCL is intact, the radial head transmits roughly 60% of the axial load across the elbow. However, when the MCL is compromised—as is universally the case in a complete terrible triad dislocation—the radial head becomes the primary restraint to valgus force. Consequently, excision of a fractured radial head in the setting of ligamentous instability is an absolute contraindication, as it will inevitably lead to catastrophic valgus collapse and proximal radial migration (Essex-Lopresti phenomenon).

The synergistic relationship between the radial head and the coronoid process cannot be overstated. They act in concert to resist posterior translation of the forearm relative to the humerus. Biomechanical studies have elegantly demonstrated that isolated deficiencies of either the radial head or the coronoid can be tolerated if the other structures remain intact. However, combined deficiencies, even minor ones, exponentially decrease the force required to dislocate the elbow. Therefore, the surgical restoration of both of these bony anterior columns is non-negotiable.
Ligamentous and Dynamic Stabilizers
The collateral ligament complexes are the primary soft-tissue restraints of the elbow. The Medial Collateral Ligament (MCL) complex is composed of anterior, posterior, and transverse bundles. The anterior bundle is the most biomechanically significant, serving as the primary restraint to valgus stress throughout the entire arc of flexion. It originates from the anteroinferior surface of the medial epicondyle and inserts onto the sublime tubercle, a distinct prominence at the medial base of the coronoid process. Because Type III coronoid fractures involve the sublime tubercle, they inherently compromise MCL integrity, necessitating rigid fixation of the coronoid fragment to restore medial stability.
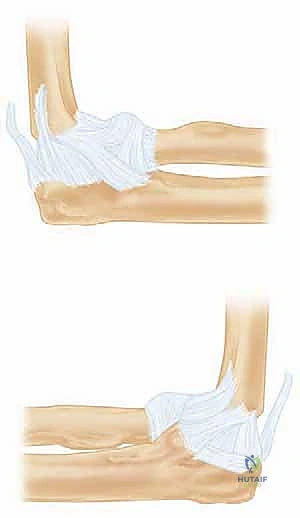
The Lateral Collateral Ligament (LCL) complex is the primary defense against posterolateral rotatory instability (PLRI). The key structure within this complex is the lateral ulnar collateral ligament (LUCL), which originates from the lateral epicondyle, courses posterior to the radial head, and inserts onto the supinator crest of the ulna. In the terrible triad, the LCL is almost universally avulsed from its isometric origin on the lateral epicondyle, leaving a characteristic "bare spot" that must be identified and utilized as the anatomical footprint for repair.
Dynamic stabilizers, including the common extensor and flexor origins, the brachialis, and the triceps, provide secondary compressive forces across the joint. The common extensor origin, intimately blended with the LCL complex laterally, is frequently torn during the dislocation event. Repair of this tendinous origin, along with the underlying LCL, is a critical step in restoring the lateral tension band and preventing recurrent posterolateral rotatory subluxation.
Neurovascular Topography
Navigating the surgical approaches to the elbow requires a meticulous understanding of the regional neurovascular topography. The ulnar nerve is at significant risk during medial approaches or when managing extensive posteromedial instability. It courses posterior to the medial epicondyle within the cubital tunnel before piercing the two heads of the flexor carpi ulnaris. In cases requiring MCL repair or fixation of anteromedial coronoid facets, the ulnar nerve must be definitively identified, neurolyzed, and carefully protected, occasionally requiring anterior transposition if tension or hardware impingement is a concern.
The Posterior Interosseous Nerve (PIN), a deep branch of the radial nerve, is the structure most at risk during lateral approaches to the radial head and neck. As it courses through the arcade of Frohse and between the two heads of the supinator muscle, it wraps around the radial neck. The crucial anatomical pearl here is that maintaining the forearm in full pronation during lateral exposure and hardware placement maximizes the distance between the PIN and the operative field. Pronation moves the nerve anteriorly and medially, safely away from the posterolateral surgical window.
The anterior neurovascular bundle, comprising the brachial artery and the median nerve, is rarely injured directly during the initial trauma unless there is a severe hyperextension mechanism with frank anterior soft tissue disruption. However, these structures can be compromised by massive anterior swelling, hematoma formation, or overzealous anterior retraction during coronoid fixation. Vigilant assessment of distal pulses and median nerve function is imperative throughout the perioperative period.
Exhaustive Indications and Contraindications
The management of complex elbow fracture-dislocations has evolved significantly, moving away from historical attempts at closed management toward algorithmic, protocol-driven surgical reconstruction. Non-operative management of a true terrible triad injury is almost universally condemned in modern orthopaedic practice. The inherent instability resulting from the combined loss of the anterior bony buttress (coronoid), the lateral column (radial head), and the ligamentous restraints guarantees that the joint will subluxate or dislocate in a cast or splint. Prolonged immobilization in an attempt to maintain a tenuous closed reduction leads directly to severe, intractable stiffness and the formation of heterotopic ossification (HO).
Therefore, surgical intervention is the absolute standard of care. The primary indication for surgery is the presence of an elbow dislocation associated with fractures of the radial head and coronoid process, regardless of the degree of fracture displacement. The goal is not merely to fix fractures, but to reconstruct the stabilizing envelope of the elbow to permit early, active mobilization. Even if a concentric reduction can be achieved closed, the joint will remain dynamically unstable, and surgery is required to repair the LCL and address the bony deficiencies.
Relative indications, or situations where non-operative management might theoretically be entertained, are exceedingly rare and strictly limited. They include patients who are medically unfit for general anesthesia or prolonged surgery due to severe medical comorbidities. In such salvage scenarios, the patient must accept a high likelihood of chronic instability, pain, and severely restricted function. Another highly theoretical relative indication is a truly concentric reduction with non-displaced, hairline fractures of the radial head and coronoid tip, combined with a stable arc of motion under fluoroscopy—a clinical unicorn that is almost never encountered in high-energy trauma.
Contraindications to immediate internal fixation include active, untreated local infection, which necessitates thorough debridement and delayed reconstruction. Severe soft tissue compromise, such as massive degloving injuries, severe blistering, or open fractures with gross contamination, may preclude immediate definitive fixation. In these scenarios, a staged approach is mandatory: initial aggressive debridement, provisional stabilization with a spanning external fixator, and meticulous soft tissue management, followed by definitive internal reconstruction once the soft tissue envelope has declared itself and healed sufficiently.
| Category | Specific Conditions | Rationale / Management Strategy |
|---|---|---|
| Absolute Indications | Terrible Triad Injury (Dislocation + Radial Head Fx + Coronoid Fx) | Surgery is mandatory to restore bony buttresses and ligamentous tension to permit early ROM. |
| Absolute Indications | Persistent ulnohumeral subluxation post-reduction | Indicates catastrophic failure of static stabilizers; requires immediate operative reconstruction. |
| Absolute Indications | Mechanical block to motion | Intra-articular osteochondral fragments or displaced fractures preventing concentric tracking. |
| Relative Indications (Non-Op) | Extreme medical comorbidities | Patient cannot tolerate anesthesia; must accept chronic instability and stiffness. Treatment is a sling and early motion within pain limits. |
| Absolute Contraindications | Active local infection | Requires serial debridement, antibiotics, and temporary external fixation prior to definitive reconstruction. |
| Relative Contraindications | Severe soft tissue degloving / blistering | Delay definitive ORIF. Utilize spanning external fixator until soft tissues recover to safely permit surgical incisions. |


Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Imaging
Meticulous pre-operative planning is the absolute cornerstone of a successful outcome in these highly complex reconstructive procedures. Evaluation begins with a rigorous adherence to Advanced Trauma Life Support (ATLS) protocols, as these high-energy injuries are frequently associated with concomitant systemic or musculoskeletal trauma. A thorough secondary survey is mandatory, with particular attention paid to the ipsilateral shoulder and wrist to rule out longitudinal injuries such as an Essex-Lopresti fracture-dislocation. A comprehensive, meticulously documented pre-operative neurovascular examination is critical, specifically assessing the function of the ulnar, median, and radial nerves, as well as the posterior interosseous and anterior interosseous branches.
Imaging begins with high-quality, orthogonal plain radiographs (Anteroposterior and true Lateral views) of the elbow. These must be obtained both before and after any attempts at closed reduction. The lateral radiograph is particularly crucial for assessing the concentricity of the ulnohumeral joint; the "teardrop" of the distal humerus should align perfectly with the greater sigmoid notch, and a line drawn down the center of the radius must bisect the capitellum in all views. Any widening of the joint space or loss of parallelism indicates persistent subluxation and trapped soft tissue or bony fragments.

While plain films are informative, Computed Tomography (CT) scans with 2D multiplanar reformats and 3D reconstructions are the gold standard and are absolutely mandatory for pre-operative planning in terrible triad injuries. CT provides an unparalleled, three-dimensional understanding of the fracture morphology. It allows the surgeon to accurately classify the coronoid fracture (differentiating a simple tip avulsion from a complex anteromedial facet fracture), assess the degree of radial head comminution, and identify occult intra-articular osteochondral shear fragments that could block rotation or flexion.
Equipment Preparation and Templating
Armed with high-resolution CT data, the surgeon must anticipate every necessary implant and instrument. The operating room must be stocked with small and mini-fragment sets (1.5mm, 2.0mm, 2.4mm, and 2.7mm), headless compression screws (Herbert screws) for articular fragments, and robust suture anchors (loaded with high-tensile, non-absorbable tape or suture) for ligamentous repairs. Furthermore, a modular, metallic radial head arthroplasty system must be immediately available. The surgeon must never assume a comminuted radial head can be fixed until it is directly visualized intraoperatively.
Templating involves utilizing the CT scan or radiographs of the contralateral, uninjured elbow to estimate the required size of the radial head prosthesis. Precise sizing is critical; overstuffing the radiocapitellar joint by even 2 millimeters alters elbow kinematics, increases contact pressures on the capitellum leading to early arthritis, and can prevent concentric reduction of the ulnohumeral joint. It must be explicitly stated that silicone radial head implants are biomechanically inadequate, fail to resist valgus or longitudinal forces, induce severe inflammatory synovitis, and have absolutely no role in the modern management of elbow fracture-dislocations.
Patient Positioning and Anesthesia
The procedure is performed under general anesthesia to ensure complete muscle relaxation, which is vital for joint reduction and dynamic stability testing. The patient is typically positioned supine on the operating table. The operative extremity is supported on a dedicated, radiolucent hand table. This setup allows the surgeon and assistant to sit comfortably and provides unimpeded, 360-degree access for the C-arm fluoroscopy unit.
A sterile tourniquet is applied high on the brachium, ensuring adequate padding to protect the skin and neurovascular structures. The entire upper extremity, from the axilla down to the fingertips, is prepped and draped free. This is a critical step; the surgeon must be able to freely manipulate the elbow through a full, unrestricted arc of flexion, extension, pronation, and supination to assess stability intraoperatively. In cases where the pre-operative CT suggests massive bone loss requiring structural grafting, the ipsilateral iliac crest should also be prepped and draped. The fluoroscopy unit (C-arm) is positioned parallel to the floor, entering from the head or the foot of the table, allowing for rapid acquisition of true AP and lateral images without requiring awkward repositioning of the patient's arm.
Step-by-Step Surgical Approach and Fixation Technique
The Standardized Surgical Protocol
The surgical execution for a terrible triad injury must follow a rigorous, standardized protocol to ensure success. This protocol is based on the principle of rebuilding the elbow from the "inside out" or "deep to superficial." The established sequence is: 1) Fixation of the coronoid process; 2) Reconstruction or replacement of the radial head; 3) Repair of the Lateral Collateral Ligament (LCL) complex; 4) Dynamic assessment of stability; and 5) Repair of the Medial Collateral Ligament (MCL) or application of a hinged external fixator if residual instability persists.
The choice of surgical incision is debated, but a universal posterior midline incision is highly versatile. It allows access to both the medial and lateral sides of the joint through the elevation of full-thickness fasciocutaneous flaps. This minimizes the risk of injury to the medial and lateral antebrachial cutaneous nerves and provides extensile exposure if the surgical plan changes. Alternatively, separate direct lateral (Kocher or Kaplan) and medial incisions can be utilized, though the skin bridge between them must be sufficiently wide (at least 7 cm) to prevent necrosis.
Deep exposure on the lateral side typically utilizes the traumatic rent in the extensor origin and the LCL complex. The Kocher interval (between the extensor carpi ulnaris and the anconeus) provides excellent access to the radial head and posterolateral capsule. The Kaplan interval (between the extensor digitorum communis and the extensor carpi radialis brevis) provides a more direct, anterior view of the coronoid but places the posterior interosseous nerve (PIN) at slightly higher risk. Regardless of the interval, the forearm must be kept in full pronation to protect the PIN.
Coronoid and Radial Head Reconstruction
The coronoid must be addressed first, as it is the deepest structure and the cornerstone of ulnohumeral stability. Once the radial head is fixed or replaced, access to the coronoid is severely restricted. For small, Type I or II tip fractures, which are essentially capsular avulsions, fixation is best achieved using a "suture lasso" technique. Heavy, non-absorbable sutures (#2 FiberWire or similar) are passed through the anterior capsule and the coronoid fragment, then shuttled through drill holes exiting the posterior cortex of the proximal ulna, and tied over a bony bridge. For larger, basal Type III fractures, rigid internal fixation using mini-fragment screws or a dedicated anterior buttress plate is required, often necessitating a separate medial or anteromedial approach.
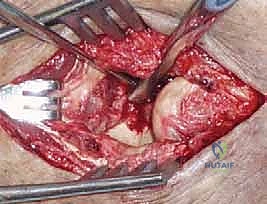
Following coronoid fixation, attention turns to the radial head. If the fracture is a simple, two- or three-part pattern (Mason Type II) without severe comminution, Open Reduction and Internal Fixation (ORIF) with headless compression screws or a low-profile plate in the "safe zone" (the non-articulating arc of the radial head) is preferred. However, in the terrible triad, the radial head is frequently severely comminuted (Mason Type III). In these cases, attempts at heroic ORIF often fail, leading to nonunion or hardware failure. The definitive treatment is excision of the fragments and immediate metallic radial head arthroplasty.
Sizing the radial head prosthesis is a critical, exacting step. The excised fragments should be assembled on the back table to estimate the native diameter and thickness. The implant must sit precisely at the level of the proximal radioulnar joint, articulating smoothly with the lesser sigmoid notch. Overstuffing the joint will cause a loss of flexion, lateral elbow pain, and capitellar wear. The surgeon must confirm under fluoroscopy that the ulnohumeral joint space is symmetric and that the radial head tracks concentrically with the capitellum throughout pronation and supination.

Ligamentous Repair and Stability Assessment
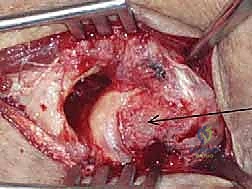
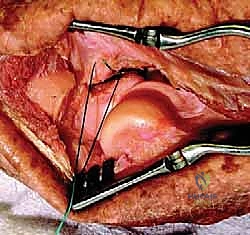
With the anterior bony columns reconstructed, the lateral tension band must be restored. The LCL complex, specifically the lateral ulnar collateral ligament (LUCL), is repaired to its anatomical footprint on the lateral epicondyle. This "bare spot" is located at the isometric center of rotation. Fixation is achieved using robust suture anchors or transosseous tunnels. The critical technical pearl here is to tie these sutures with the elbow in 90 degrees of flexion and the forearm in full pronation. Pronation closes the lateral joint space and removes tension from the LCL
Clinical & Radiographic Imaging Archive




