Lateral Ulnar Collateral Ligament Reconstruction for Posterolateral Rotatory Instability
Key Takeaway
Lateral ulnar collateral ligament (LUCL) reconstruction is the gold-standard surgical intervention for chronic posterolateral rotatory instability (PLRI) of the elbow. This comprehensive guide details the modified Kocher approach, precise isometric tunnel placement at the lateral epicondyle and crista supinatoris, and graft tensioning techniques. Designed for orthopedic surgeons, it provides an evidence-based, step-by-step protocol to restore the lateral collateral ligament complex and ensure optimal postoperative joint stability and kinematics.
Comprehensive Introduction and Patho-Epidemiology
Posterolateral rotatory instability (PLRI) represents the most frequently encountered pattern of chronic elbow instability, manifesting as a complex, three-dimensional kinematic disruption of the ulnohumeral and radiocapitellar joints. First comprehensively elucidated in the seminal works of O’Driscoll, Morrey, and Bell, PLRI is characterized by a specific displacement pattern: as the elbow extends and supinates under an axial load, the ulna supinates and subluxates posterolaterally away from the trochlea, obligatorily carrying the radius with it. This abnormal tracking results in the radial head subluxating posterior to the capitellum, producing the characteristic clinical symptoms of mechanical catching, locking, and a profound sensation of the elbow "giving way." Understanding this triplanar instability is paramount for the orthopedic surgeon, as failure to recognize the rotational component often leads to misdiagnosis and inappropriate management of lateral-sided elbow pain.
The primary pathoanatomic lesion driving PLRI is the incompetence, attenuation, or frank avulsion of the lateral ulnar collateral ligament (LUCL), a critical component of the lateral collateral ligament (LCL) complex. The mechanism of injury is classically described as a fall on an outstretched hand (FOOSH), generating a predictable cascade of forces: axial compression, valgus stress, and external rotation (supination) of the forearm relative to the humerus. This force vector initiates soft tissue disruption on the lateral side of the elbow, which can progressively march medially if the energy is sufficient. This progression is elegantly described by the Horii circle concept, which delineates the stages of elbow instability from Stage 1 (partial or complete disruption of the LCL complex resulting in PLRI) to Stage 3 (complete capsuloligamentous disruption including the medial collateral ligament, resulting in frank dislocation).
Epidemiologically, PLRI can present in both acute and chronic settings, though it is most frequently diagnosed in the chronic phase after conservative management of an ostensibly "simple" elbow sprain or reduced dislocation has failed. Furthermore, PLRI is a hallmark of complex elbow trauma, frequently accompanying the "terrible triad" of the elbow (elbow dislocation, radial head fracture, and coronoid process fracture). In these complex scenarios, the bony stabilizers are compromised, placing an exponentially higher demand on the ligamentous restraints. Iatrogenic PLRI is also a well-documented phenomenon, occasionally occurring following excessive lateral surgical exposures for radial head resections or extensor origin releases for recalcitrant lateral epicondylitis (tennis elbow), where the LUCL is inadvertently transected or compromised.
Clinically, the presentation of chronic PLRI can be subtle, demanding a high index of suspicion. Patients rarely present with a frank dislocation; instead, they report activity-related apprehension and mechanical symptoms. The pain is typically localized to the lateral joint line, often exacerbated by activities requiring terminal extension combined with supination, such as pushing up from a chair or performing a push-up. The insidious nature of these symptoms frequently leads to misdiagnoses, most commonly refractory lateral epicondylitis. Therefore, a meticulous clinical examination, incorporating provocative maneuvers designed to recreate the posterolateral subluxation, is the cornerstone of accurate diagnosis and subsequent surgical planning.
Detailed Surgical Anatomy and Biomechanics
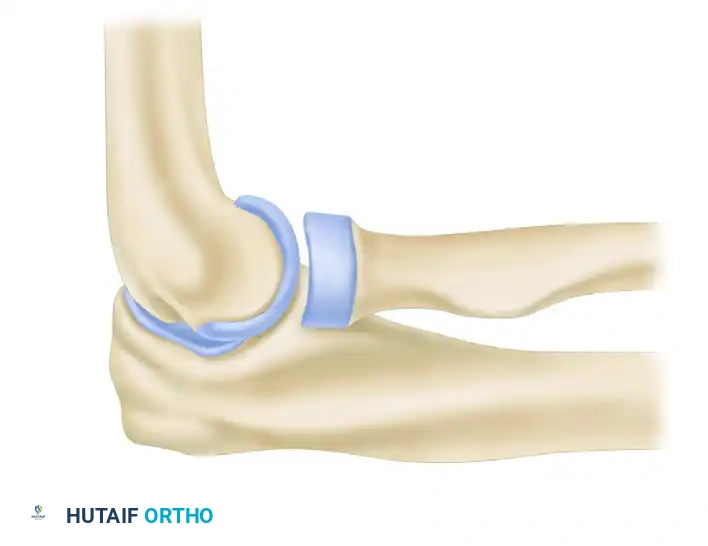
A profound and precise understanding of the lateral ligamentous complex and the osseous architecture of the radiocapitellar and ulnohumeral joints is mandatory for the successful reconstruction of the LUCL. The lateral collateral ligament (LCL) complex is a multifaceted capsuloligamentous structure consisting of four distinct, interconnected components: the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), the annular ligament, and the accessory lateral collateral ligament. The RCL originates from the lateral epicondyle and fans out distally to blend seamlessly into the annular ligament, providing a primary restraint to varus stress while allowing the radius to rotate freely within its fascial sling. The annular ligament itself is a robust, funnel-shaped band that encircles the radial head, anchoring it to the lesser sigmoid notch of the ulna and stabilizing the proximal radioulnar joint during pronation and supination.
The lateral ulnar collateral ligament (LUCL) is the most critical structure in the prevention of PLRI. It functions as the primary restraint to varus and posterolateral rotatory stress. The LUCL originates at the lateral epicondyle, sharing a footprint with the RCL, but courses superficial and posterior to the annular ligament. It traverses the radiocapitellar joint to insert distally on the crista supinatoris (supinator crest) of the proximal ulna. This unique origin-to-insertion pathway—spanning from the humerus to the ulna while bypassing the radius—allows the LUCL to act as a posterior sling for the radial head, preventing its posterior translation during supination and extension. The accessory lateral collateral ligament, a less consistent structure, originates from the annular ligament and inserts on the supinator crest, assisting in stabilizing the annular ligament during varus loading.
Biomechanically, the elbow relies on a highly synchronized interplay between static osseous articulations, static ligamentous restraints, and dynamic muscular forces. The ulnohumeral joint provides primary osseous stability, while the radiocapitellar joint acts as a secondary bony stabilizer, particularly against valgus and longitudinal forces. The LUCL operates as the primary static soft-tissue stabilizer on the lateral side. Crucially, the humeral origin of the LUCL represents the isometric axis of the ulnohumeral joint. This isometric point lies precisely at the intersection of the anterior humeral line and the radiocapitellar axis on a true lateral radiograph. Accurate identification of this point is the single most critical step in LUCL reconstruction; non-isometric graft placement will result in either restricted range of motion (if the graft is too tight in certain arcs) or recurrent instability (if the graft stretches out).
The dynamic stabilizers of the lateral elbow further augment the static restraints. The common extensor origin (CEO), particularly the extensor carpi ulnaris (ECU) and the extensor digitorum communis (EDC), provides a dynamic compressive force across the radiocapitellar joint. The anconeus muscle also plays a vital role in preventing posterolateral subluxation by acting as a dynamic restraint during pronation. In the setting of PLRI, the loss of the LUCL's static sling effect overwhelms these dynamic stabilizers, leading to the characteristic uncoupling of the radiocapitellar joint. Surgical reconstruction must therefore not only recreate the static LUCL but also meticulously repair the dynamic muscular origins to restore the intricate biomechanical balance of the lateral elbow.
Exhaustive Indications and Contraindications
The decision to proceed with operative reconstruction of the lateral ulnar collateral ligament requires a rigorous evaluation of the patient's clinical symptoms, physical examination findings, and advanced imaging, balanced against their functional demands and physiological status. The primary indication for LUCL reconstruction is recurrent, symptomatic posterolateral rotatory instability that has definitively failed a comprehensive, minimum 3 to 6-month trial of conservative therapy. Conservative management typically includes activity modification, hinged elbow bracing with a pronation block, and targeted physical therapy focusing on strengthening the dynamic stabilizers (brachioradialis, common extensors, and anconeus). When these measures fail to alleviate mechanical symptoms—such as clicking, locking, or the sensation of the elbow "giving way" during activities of daily living or athletic endeavors—surgical intervention becomes warranted.
Clinical examination is paramount in establishing surgical indications. A positive lateral pivot-shift test of the elbow, performed with the patient supine and the arm positioned overhead, is the pathognomonic physical finding. As the examiner applies an axial load, valgus stress, and supination while slowly flexing the elbow from full extension, a palpable and visible clunk is appreciated at approximately 40 degrees of flexion as the radiocapitellar joint reduces. Additional provocative maneuvers, such as the posterolateral rotatory drawer test, the chair push-up test, and the tabletop relocation test, further corroborate the diagnosis. In cases where patient guarding precludes an accurate awake examination, a dynamic examination under anesthesia (EUA) utilizing fluoroscopy is highly indicated and often serves as the final confirmatory step immediately prior to surgical incision.
Imaging plays a critical supportive role in confirming the indications for surgery. Standard orthogonal radiographs (AP, lateral, and oblique views) are essential to rule out associated osseous pathology, such as subtle radial head fractures, coronoid tip avulsions, or intra-articular loose bodies that may mimic or exacerbate mechanical symptoms. Magnetic Resonance Imaging (MRI) is considered the gold standard advanced imaging modality for evaluating the soft tissue envelope. High-resolution MRI, particularly with intra-articular contrast (MR arthrography), provides detailed visualization of the LCL complex, allowing the surgeon to identify LUCL attenuation, mid-substance tears, or avulsions from the lateral epicondyle or supinator crest. Furthermore, MRI assesses the integrity of the common extensor origin and the secondary capsular structures, guiding the extent of the necessary surgical repair.
Contraindications to LUCL reconstruction must be carefully weighed to prevent catastrophic outcomes or surgical failures. Absolute contraindications include active local or systemic infection, severe medical comorbidities precluding safe anesthesia, and a non-functional or paralyzed extremity where stability would not improve function. Relative contraindications require nuanced clinical judgment. Severe, advanced ulnohumeral or radiocapitellar osteoarthritis may render a ligament reconstruction futile, as the primary pain generator is degenerative rather than purely instable; in such cases, total elbow arthroplasty or interposition arthroplasty might be considered in the appropriate demographic. Additionally, significant patient non-compliance is a strong relative contraindication, as the post-operative rehabilitation protocol is stringent, and failure to adhere to bracing and motion restrictions will inevitably lead to graft failure and recurrent instability.
| Category | Specific Conditions | Clinical Rationale / Impact on Surgery |
|---|---|---|
| Absolute Indications | Recurrent symptomatic PLRI failing 3-6 months conservative care | Mechanical symptoms (giving way, locking) severely limit ADLs and athletic function. |
| Absolute Indications | Positive Pivot-Shift Test (Awake or EUA) | Confirms the pathoanatomic uncoupling of the radiocapitellar joint requiring structural restoration. |
| Absolute Indications | Acute PLRI in the setting of a "Terrible Triad" injury | Bony instability demands immediate restoration of lateral ligamentous restraints to permit early motion. |
| Relative Indications | Iatrogenic PLRI following lateral epicondylitis release | Attenuated tissues may require reconstruction rather than simple repair due to poor tissue quality. |
| Absolute Contraindications | Active local or systemic infection | High risk of deep joint infection and graft necrosis. |
| Absolute Contraindications | Medically unfit for surgery | Anesthetic risks outweigh the functional benefits of elbow stabilization. |
| Relative Contraindications | Advanced multi-compartment elbow osteoarthritis | Joint stabilization will not resolve degenerative pain; alternative arthroplasty procedures preferred. |
| Relative Contraindications | Documented patient non-compliance | Post-operative protocol requires strict adherence to pronation bracing; failure guarantees graft stretching. |
| Relative Contraindications | Asymptomatic clinical laxity | Laxity without mechanical symptoms or functional deficit does not warrant operative morbidity. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the foundation of a successful LUCL reconstruction, beginning with a comprehensive review of all imaging modalities. The surgeon must carefully evaluate the osseous architecture on plain radiographs to ensure there is adequate bone stock at the lateral epicondyle and the crista supinatoris to accommodate the necessary drill tunnels. If prior trauma or multiple corticosteroid injections have compromised the bone quality, alternative fixation methods, such as cortical buttons or solid suture anchors, must be available in the surgical armamentarium. Templating the anticipated tunnel trajectories and bone bridge dimensions (minimum 1.5 to 2.0 cm at the ulna) helps mitigate the risk of intra-operative cortical blowout. Furthermore, the MRI should be reviewed to assess the quality of the native capsular tissues, which will dictate whether a primary repair with augmentation or a complete autograft reconstruction is required.
Graft selection is a critical component of pre-operative planning and must be discussed extensively with the patient. The ipsilateral palmaris longus tendon is the autograft of choice due to its excellent biomechanical properties, minimal harvest morbidity, and appropriate length and diameter for passing through osseous tunnels. The presence of the palmaris longus must be confirmed pre-operatively using the Schaeffer test (opposition of the thumb and little finger with wrist flexion). In the approximately 15% of patients who are congenitally absent of a palmaris longus, alternative graft sources must be planned. The gracilis tendon autograft is a robust alternative, though it requires prepping a secondary surgical site on the lower extremity. Other options include a strip of triceps fascia or, in revision cases or multi-ligamentous injuries, allograft tissue (e.g., semitendinosus), though allografts carry a slightly higher risk of attenuation over time.
Anesthetic management is tailored to optimize both intra-operative conditions and post-operative pain control. General anesthesia is typically preferred, as it ensures complete muscle relaxation, facilitating the dynamic examination under anesthesia (EUA) and the subsequent joint reduction and graft tensioning. This is routinely supplemented with a regional anesthetic block, such as a supraclavicular or axillary brachial plexus block. The regional block provides profound post-operative analgesia, reducing the need for systemic opioids and allowing for a smoother transition to the immediate post-operative rehabilitation phase. The anesthesia team must be informed of the need for an EUA prior to the administration of long-acting paralytics, ensuring the pivot-shift phenomenon can be accurately assessed.
Patient positioning and operating room setup must be executed with precision to allow unhindered access to the lateral elbow and the graft harvest site. The patient is placed in the supine position on a standard operating table. The operative upper extremity is meticulously prepped and draped free to allow full, unrestricted range of motion (flexion, extension, pronation, supination, and varus/valgus stress). The arm can be brought across the patient's chest for the lateral exposure, or supported on a radiolucent arm board, which is particularly useful when fluoroscopy is required. A sterile pneumatic tourniquet is applied high on the brachium over ample padding. Following exsanguination with an Esmarch bandage, the tourniquet is inflated to 250 mm Hg. If a lower extremity autograft (e.g., gracilis) is planned, the ipsilateral leg is prepped and draped simultaneously. The fluoroscopy unit (C-arm) should be positioned on the contralateral side of the table, ready to be brought in for orthogonal imaging to confirm isometric pin placement and tunnel trajectories.
Step-by-Step Surgical Approach and Fixation Technique
1. The Modified Kocher Approach and Superficial Dissection
The surgical intervention begins with the modified Kocher approach, providing optimal, extensile access to the lateral ligamentous complex. The skin incision is initiated approximately 5 cm proximal to the lateral epicondyle, extending distally directly over the epicondyle, and then curving gently anteriorly toward the radial head, terminating at the level of the annular ligament. This curvilinear incision minimizes the risk of crossing flexion creases at a perpendicular angle, thereby reducing the likelihood of hypertrophic scarring and subsequent soft-tissue contractures. Following the skin incision, hemostasis is meticulously achieved using electrocautery.
The superficial dissection proceeds by incising the deep antebrachial fascia in line with the skin incision. The critical step here is identifying the internervous plane between the anconeus muscle (innervated by the radial nerve) posteriorly and the extensor carpi ulnaris (ECU, innervated by the posterior interosseous nerve) anteriorly. Developing this plane provides a safe corridor to the deep structures. The surgeon must exercise extreme caution as the dissection proceeds distally.
⚠️ Surgical Warning: The Posterior Interosseous Nerve (PIN)
The posterior interosseous nerve (PIN) lies vulnerable within the substance of the supinator muscle belly. When dissecting distally to expose the supinator crest, it is imperative to maintain the forearm in full pronation. Pronation dynamically shifts the PIN anteriorly and medially, safely distancing it from the lateral surgical field. Retractors must be placed with precision; blind or forceful placement of Hohmann retractors around the radial neck is strictly contraindicated to prevent iatrogenic PIN palsy.
2. Deep Dissection and Exposure of the Ligamentous Complex
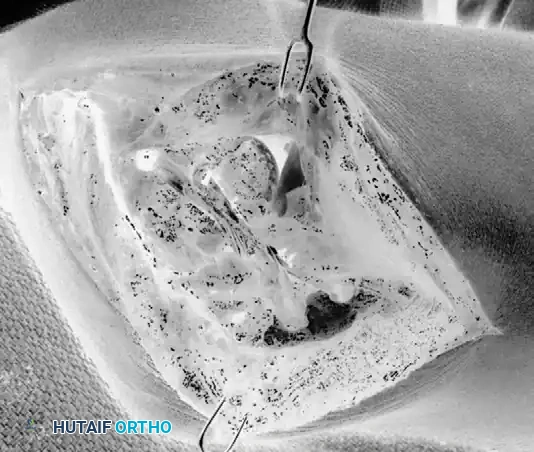
Once the internervous plane is developed, the deep dissection involves elevating the common extensor origin (CEO). By sharp dissection, the CEO, including a portion of the extensor carpi radialis brevis (ECRB), is carefully elevated off the lateral epicondyle to reveal the underlying origin of the radial collateral ligament complex. Distally, the anconeus muscle is reflected posteriorly, and the ECU is reflected anteriorly. The extension of the anconeus origin to the lateral aspect of the triceps fascia is also reflected sufficiently to expose the entire lateral ligamentous footprint.
The primary anatomic landmark on the ulna, the crista supinatoris (supinator crest), must now be definitively identified. This distinct bony ridge serves as the anatomic insertion site of the LUCL. Typically, upon exposing this region in a patient with chronic PLRI, the surgeon will observe a lax, attenuated ulnar band of the radial collateral ligament, or a frank avulsion of the capsuloligamentous tissue from the epicondyle or crest. The abnormal tissue is carefully debrided to healthy margins, ensuring a robust biological bed for the subsequent reconstruction.
3. Ligament Imbrication and Advancement
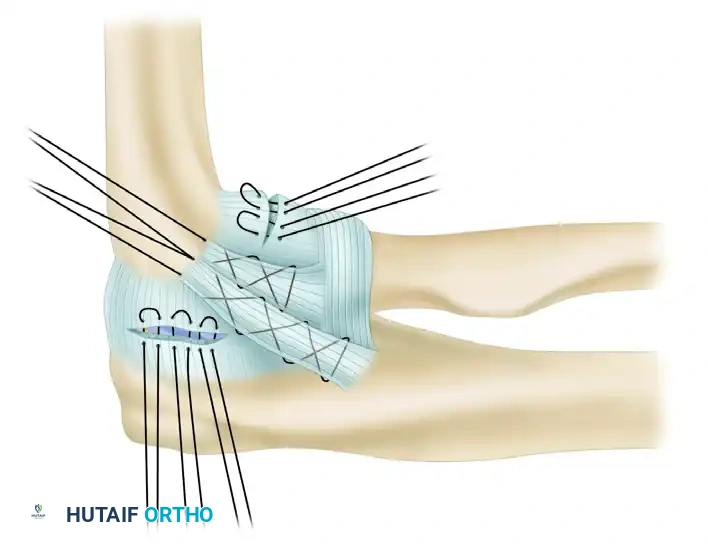
Prior to the introduction of the autograft, the native, attenuated lateral tissues are managed to provide a secondary layer of stability. An imbrication and advancement of the ulnar band of the radial collateral ligament and the anterior capsule are performed. This is achieved utilizing a Bunnell-type running locking suture technique with a high-tensile, non-absorbable suture.
These sutures are then passed through small drill holes created at the anatomical origin of the ligament on the lateral epicondyle. Tying these sutures effectively plicates the redundant posterior and anterior capsule, eliminating pathologic volume within the joint and providing a robust secondary restraint that will protect the primary graft during the early phases of biological incorporation.
4. Ulnar Tunnel Preparation
Attention is then directed to the proximal ulna for the preparation of the osseous tunnels. The ulnar tunnels must be placed with exacting precision at the crista supinatoris to replicate the anatomic insertion of the LUCL. Using a high-speed burr or a 3.2-mm drill bit, two converging drill holes are created at the supinator crest.
It is critical that these holes are separated by a substantial bone bridge, typically measuring 1.5 to 2.0 cm in length. A bone bridge of inadequate width is highly susceptible to cortical blowout during the final graft tensioning phase, which severely compromises fixation. The trajectory of the tunnels should be oriented to align optimally with the isometric point on the lateral epicondyle, ensuring a smooth, linear path for the graft that avoids acute angulations and subsequent abrasive wear.
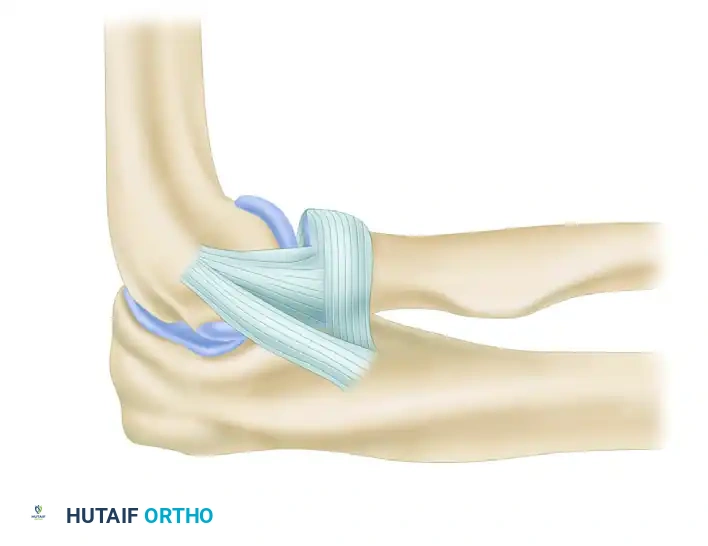
5. Graft Harvest and Passage
Concurrent with or immediately following tunnel preparation, the autograft is harvested. The palmaris longus tendon is harvested utilizing a standard tendon stripper, yielding a graft typically 15 to 20 cm in length. The graft is cleared of adherent muscle belly and paratenon on the back table. Both ends of the graft are then meticulously whip-stitched using a #2 non-absorbable, high-tensile suture (e.g., FiberWire or Ethibond) to facilitate passage and tensioning.
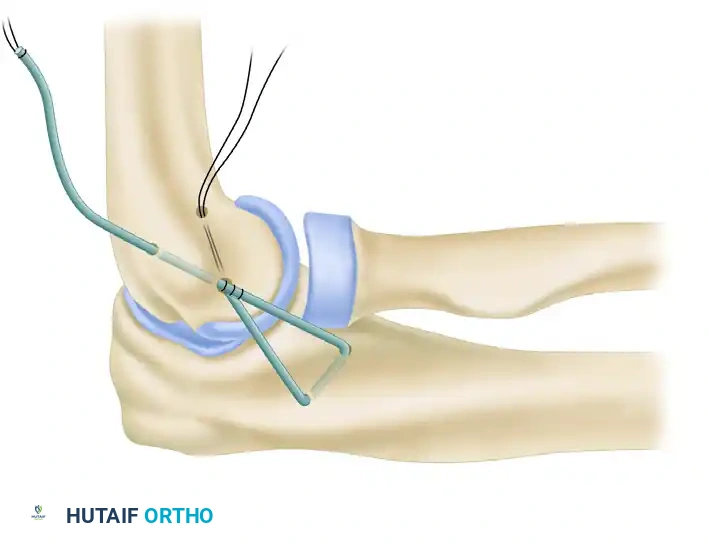
The prepared graft is then passed through the converging ulnar tunnels. To secure the graft at the ulnar insertion and prevent slippage during humeral tensioning, a "yoke stitch" is frequently employed. This technique involves suturing the graft upon itself at the exit of the ulnar tunnels, creating a low-profile, highly secure anchor point at the crista supinatoris before the two free limbs are passed proximally toward the humerus.
6. Humeral Tunnel Preparation and Isometry
The identification and utilization of the isometric point on the lateral epicondyle is the most unforgiving step of the procedure. The isometric point is defined radiographically at the precise intersection of the anterior humeral line and the radiocapitellar axis. Clinically, it lies at the center of the capitellar curvature of the lateral epicondyle.
Before committing to the final large-diameter drill holes, isometry must be dynamically tested. A 2.0-mm K-wire is driven into the presumed isometric point. A heavy suture is looped around the ulnar bone bridge and then passed around the K-wire. The surgeon then takes the elbow through a full, uninhibited range of motion (0 to 140 degrees of flexion). The excursion of the suture is meticulously measured; it should not change length by more than 1 to 2 mm. If the suture stretches significantly in flexion, the K-wire is positioned too anteriorly. Conversely, if it stretches in extension, the K-wire is too posterior.
Once isometry is definitively confirmed, the humeral tunnels are created. A primary entry hole is drilled at the isometric point. This hole is then expanded internally to create a Y-shaped or V-shaped intraosseous pathway. One exit hole is directed posterosuperiorly, and the second is directed posteroinferiorly, exiting the far cortex of the lateral epicondylar ridge. This configuration allows the two limbs of the graft to be drawn into the humerus and tied over a robust cortical bone bridge.
7. Graft Tensioning and Final Fixation
The two free limbs of the palmaris longus graft are drawn proximally from the ulna and introduced into the primary isometric hole on the humerus, utilizing suture passing loops to retrieve them through the superior and inferior exit holes. The critical phase of graft tensioning now commences.
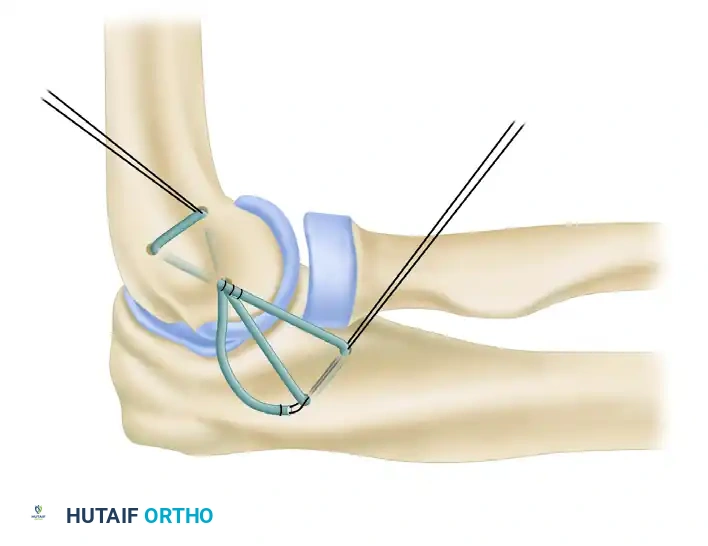
The elbow is positioned in approximately 30 to 40 degrees of flexion, and the forearm is placed in maximal, full pronation. Pronation is an absolute requirement during tensioning, as it dynamically closes the lateral radiocapitellar joint space and perfectly reduces the posterolateral subluxation. Simultaneously, a mild varus stress is applied by the assistant to ensure the ulnohumeral joint is congruently reduced and no lateral gapping exists.
With the joint held in this meticulously reduced position, the graft limbs are pulled taut, drawing the graft deeply into the humeral tunnel. The limbs are then tied securely over the humeral bone bridge. In a docking configuration, the limbs may be sutured directly to each other and to the adjacent periosteum, providing a robust, anatomic, figure-of-eight reconstruction of the LUCL that resists triplanar deforming forces.
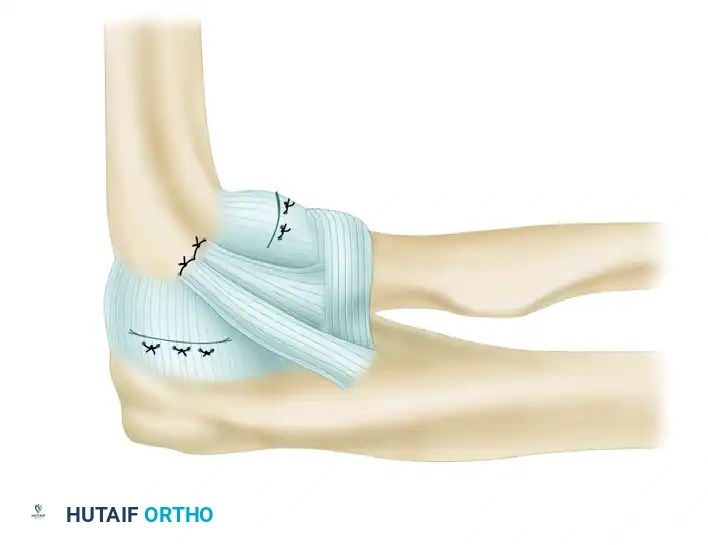
8. Closure
Following final fixation, the joint is taken through a gentle range of motion to confirm stability and the absence of impingement. The native capsular flaps and the common extensor origin, which were previously tagged, are now meticulously repaired over the graft reconstruction.
The CEO is securely reattached to its anatomic footprint on the lateral epicondyle using either transosseous sutures through the epicondylar ridge or small suture anchors. This restores the dynamic stabilizing effect of the extensor musculature. The deep fascial layers are closed with heavy absorbable sutures. The subcutaneous tissue is approximated, and the skin is closed with a subcuticular stitch or surgical staples. A sterile, non-adherent dressing is applied, and the extremity is immediately immobilized in a well-padded posterior splint with the elbow in 70 to 80 degrees of flexion and the forearm in full pronation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, lateral ulnar collateral ligament reconstruction is associated with a specific profile of complications. The most devastating complication is recurrent posterolateral rotatory instability, which occurs in approximately 5% to 8% of cases. The primary technical etiology for recurrent instability is non-isometric tunnel placement, specifically placing the humeral origin too anteriorly, which
