Septic Arthritis of the Hand and Wrist: An Intraoperative Drainage Masterclass

Key Takeaway
This masterclass details the urgent surgical management of septic arthritis in the hand and wrist. Fellows will learn comprehensive anatomy, precise diagnostic techniques, and step-by-step intraoperative drainage procedures. We cover open and arthroscopic approaches, meticulous dissection, instrument use, and critical pearls for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Septic arthritis of the hand and wrist represents a profound orthopedic emergency, demanding immediate recognition and aggressive surgical intervention. Unlike superficial soft tissue infections, a purulent infection within the closed synovial space of a joint initiates a rapid, catastrophic cascade of articular cartilage destruction. The synovial membrane, a highly vascularized tissue lacking a limiting basement membrane, is exceptionally vulnerable to bacterial seeding. Once inoculated, pathogens proliferate exponentially within the synovial fluid, triggering a massive influx of polymorphonuclear leukocytes (PMNs). This host immune response, while intended to eradicate the pathogen, paradoxically becomes the primary driver of joint destruction.
The pathophysiology of cartilage degradation in septic arthritis is both rapid and irreversible if left unchecked. Bacteria, particularly Staphylococcus aureus, release exotoxins, hyaluronidases, and chondrocyte-stimulating factors that directly damage the articular surface. Concurrently, the host's PMNs degranulate, releasing a storm of proteolytic enzymes, including matrix metalloproteinases (MMPs), elastases, and cathepsins. Furthermore, the rapid accumulation of purulent effusion exponentially increases intra-articular pressure, leading to profound synovial ischemia and secondary pressure necrosis of the chondrocytes. Irreversible depletion of the cartilage matrix proteoglycans can occur within 48 hours of symptom onset, underscoring the absolute necessity for emergent decompression and lavage.
Epidemiologically, the etiology of hand and wrist septic arthritis is most frequently attributed to direct inoculation. Penetrating trauma, retained foreign bodies, and animal or human bites are the primary culprits. The classic "clenched fist injury" or "fight bite" frequently results in inoculation of the metacarpophalangeal (MCP) joint with a polymicrobial flora, notably including Eikenella corrodens alongside virulent Staphylococcus and Streptococcus species. Hematogenous seeding, while less common in the small joints of the hand compared to the axial skeleton or large appendicular joints, remains a critical consideration, particularly in immunocompromised hosts, intravenous drug users, or patients with underlying rheumatoid arthritis. In sexually active populations, disseminated gonococcal infection (Neisseria gonorrhoeae) must be considered, often presenting with a migratory polyarthralgia before localizing to the wrist or small joints.
Detailed Surgical Anatomy and Biomechanics
A masterful surgical approach to the infected hand and wrist requires an intimate, three-dimensional understanding of the regional anatomy. The interphalangeal (IP) and metacarpophalangeal (MCP) joints are complex articulations stabilized by a delicate interplay of capsuloligamentous and musculotendinous structures. The MCP joints are condyloid articulations permitting flexion, extension, abduction, and adduction. Their stability is primarily governed by the proper and accessory collateral ligaments and the robust volar plate. Crucially, the proper collateral ligaments are eccentric; they are lax in extension (allowing abduction/adduction) and maximally taut in 70 to 90 degrees of flexion. Conversely, the interphalangeal joints are true hinge joints. Understanding these tensioning patterns is vital during postoperative splinting to prevent debilitating contractures.

The extensor mechanism overlying these joints is highly susceptible to iatrogenic injury during surgical drainage. At the MCP level, the extensor tendon is centralized by the sagittal bands. Dorsal approaches must carefully split or retract these structures without compromising their stabilizing function. At the proximal interphalangeal (PIP) joint, the extensor mechanism divides into the central slip (inserting on the middle phalanx) and the lateral bands (converging to form the terminal tendon at the distal phalanx). Disruption of the central slip during a dorsal approach to the PIP joint will inevitably lead to a boutonniere deformity, while injury to the terminal tendon results in a mallet finger.
The wrist joint is an intricate biomechanical marvel comprising the radiocarpal, midcarpal, and distal radioulnar joints (DRUJ). The radiocarpal joint is entirely separated from the DRUJ by the triangular fibrocartilage complex (TFCC), provided the TFCC is intact. However, in the setting of chronic degenerative tears or acute trauma, these compartments may communicate, allowing purulence to spread from the radiocarpal space into the DRUJ. Dorsally, the wrist capsule is accessible between the extensor tendon compartments. Lister's tubercle serves as the paramount osseous landmark, separating the second dorsal compartment (extensor carpi radialis longus and brevis) from the third compartment (extensor pollicis longus). Surgical approaches, whether open or arthroscopic, heavily rely on these intervals to access the joint safely while avoiding the superficial sensory branches of the radial and ulnar nerves.
Exhaustive Indications and Contraindications
The decision to proceed with operative drainage in suspected septic arthritis is rarely ambiguous. The presence of purulent fluid within a joint space is an absolute indication for emergent surgical intervention. Delaying surgery to await final culture results in the face of strong clinical and preliminary laboratory evidence (e.g., a synovial fluid white blood cell count exceeding 50,000 cells/µL with a neutrophil predominance) constitutes a departure from the standard of care.
While surgical drainage is the definitive treatment, the specific modality—open arthrotomy versus arthroscopic lavage—depends on the joint involved, the chronicity of the infection, and the surgeon's expertise. Arthroscopy has become the gold standard for the wrist due to its superior visualization of loculations and decreased surgical morbidity, though open arthrotomy remains essential for the smaller joints of the digits or when extensive osteomyelitis is present.
| Parameter | Indications for Surgical Drainage | Contraindications (Relative/Absolute) |
|---|---|---|
| Clinical Presentation | Exquisite pain with passive ROM, joint effusion, erythema, fever. | Cellulitis without joint involvement (Absolute: Avoid inoculating a sterile joint). |
| Synovial Fluid Analysis | WBC > 50,000 cells/µL, >75% PMNs, positive Gram stain, low glucose. | Crystalline arthropathy confirmed without concomitant infection (Relative). |
| Imaging Findings | Joint effusion on MRI/Ultrasound, gas in joint space, cortical destruction. | Overlying soft tissue abscess without intra-articular extension (Relative). |
| Patient Factors | Immunocompromised status, failure of medical management (>24 hours). | Patient medically unstable for anesthesia (Relative: May require bedside aspiration/washout). |
| Surgical Modality | Arthroscopy: Native wrist joint, early presentation, minimal soft tissue necrosis. | Arthroscopy: Massive soft tissue necrosis, severe overlying cellulitis, advanced osteomyelitis requiring bone resection. |
Pre-Operative Planning, Templating, and Patient Positioning
Diagnostic Workup and Imaging
The preoperative phase is a race to confirm the diagnosis without delaying surgical decompression. A meticulous history and physical examination are paramount. The hallmark physical finding of septic arthritis is exquisite, intractable pain with any degree of passive motion. This finding is highly sensitive and helps differentiate intra-articular pathology from periarticular cellulitis or tenosynovitis. Laboratory evaluation must include a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). While the peripheral WBC count may be normal, CRP and ESR are almost universally elevated and serve as excellent baselines for monitoring the efficacy of postoperative treatment.
Radiographic evaluation begins with orthogonal plain films. Early in the disease process, radiographs are typically normal or demonstrate only subtle soft tissue swelling and joint space widening secondary to effusion. However, they are crucial for ruling out retained radiopaque foreign bodies, fractures, or underlying chronic arthropathies. The presence of chondrocalcinosis, for instance, may suggest pseudogout, though crystalline arthropathy and septic arthritis can coexist.

When the diagnosis remains equivocal, or to assess the extent of soft tissue and osseous involvement, Magnetic Resonance Imaging (MRI) is the modality of choice. MRI provides unparalleled soft tissue contrast, readily identifying joint effusions, synovial hypertrophy, and early marrow edema indicative of impending osteomyelitis. T2-weighted fluid-sensitive sequences will dramatically highlight the intra-articular purulence and surrounding inflammatory edema.

Synovial Fluid Aspiration: The Definitive Diagnostic Step
Joint aspiration (arthrocentesis) is the absolute gold standard for diagnosing septic arthritis. It must be performed prior to the administration of any antibiotics, if clinically feasible. Crucially, the overlying skin must be meticulously prepped, and the injection of local anesthetic into the skin or subcutaneous tissue should be minimized or avoided entirely, as it can obscure the anatomic landmarks, dilute the synovial sample, and potentially introduce bacteriostatic agents that interfere with cultures.
For the MCP and IP joints, a dorsal approach is utilized, entering the joint space just collateral to the extensor tendon. An 18- or 20-gauge needle attached to a small (3-5 mL) syringe is advanced until a palpable "pop" is felt as the capsule is breached. For the wrist, the aspiration is typically performed dorsally, just distal to Lister's tubercle, angling slightly volar to match the articular inclination of the radius. The aspirate is immediately sent for cell count with differential, Gram stain, aerobic and anaerobic cultures, fungal/AFB cultures, and crystal analysis.
Patient Positioning and Hemostasis
Optimal patient positioning and operating room setup are critical for a seamless procedure. The patient is positioned supine with the affected extremity extended onto a radiolucent hand table. The table must be rigidly secured to prevent any movement during microsurgical dissection. A well-padded pneumatic tourniquet is applied to the proximal arm.
Exsanguination of the limb prior to tourniquet inflation requires special consideration in the setting of infection. The traditional use of an Esmarch bandage to tightly wrap and exsanguinate the limb is strictly contraindicated. The mechanical compression of the Esmarch can force purulent material, bacteria, and inflammatory mediators proximally into the systemic circulation, potentially precipitating bacteremia or sepsis. Instead, the limb is elevated for 3 to 5 minutes to allow for gravity exsanguination before the tourniquet is inflated to 250 mmHg. This provides the necessary bloodless field to identify delicate neurovascular structures without risking systemic dissemination of the pathogen.
Step-by-Step Surgical Approach and Fixation Technique
Open Drainage of the Metacarpophalangeal (MCP) Joint
The MCP joint is most reliably approached via a dorsal longitudinal incision. This approach provides excellent visualization of the joint capsule and allows for extensive irrigation while avoiding the palmar neurovascular bundles.
- Incision and Dissection: A 3-cm dorsal longitudinal incision is made centered over the affected MCP joint. Subcutaneous tissues are bluntly dissected to protect the dorsal sensory venous network.
- Extensor Mechanism Management: The extensor tendon is identified. To access the joint, the sagittal band is incised longitudinally on either the radial or ulnar side of the extensor tendon. The tendon is then gently retracted to the contralateral side using a Ragnell or Senn retractor.
- Capsulotomy and Debridement: A longitudinal capsulotomy is performed. Immediately upon breaching the capsule, purulent fluid will typically egress. Swab cultures should be taken at this precise moment if preoperative aspiration was unsuccessful.
- Irrigation: The joint is aggressively irrigated with a minimum of 1 to 2 liters of sterile normal saline. A small rongeur or curette is used to meticulously debride any fibrinous exudate, necrotic synovium, and debris from the articular gutters.

Open Drainage of the Interphalangeal (PIP and DIP) Joints
Approaching the PIP and DIP joints requires extreme caution to preserve the delicate extensor mechanism.
- The Midaxial Approach: For the PIP joint, a midaxial approach is often preferred over a direct dorsal approach to avoid injuring the central slip. The midaxial line is identified by connecting the apices of the flexion creases. An incision is made along this line.
- Neurovascular Protection: The dissection proceeds volar to the lateral band of the extensor mechanism but dorsal to the neurovascular bundle. Cleland's ligaments may need to be divided to mobilize the neurovascular bundle volarly.
- Capsular Access: The transverse retinacular ligament is incised, and the collateral ligament is identified. The joint capsule is incised dorsal to the collateral ligament, allowing access to the joint space for thorough irrigation and synovectomy.
- DIP Joint: The DIP joint can be approached via a similar midaxial incision or a dorsal H-shaped or Y-shaped incision, taking absolute care not to disrupt the terminal extensor tendon insertion on the distal phalanx.
Arthroscopic Drainage of the Wrist Joint
Wrist arthroscopy has revolutionized the management of radiocarpal and midcarpal septic arthritis. It allows for comprehensive visualization, targeted debridement of loculations, and high-volume irrigation with significantly less surgical trauma than an open dorsal arthrotomy.
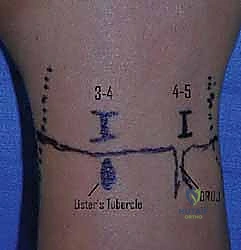
- Setup and Portals: The hand is placed in sterile traction using a specialized wrist tower, with 10-15 lbs of distraction applied via finger traps on the index and middle fingers. Standard radiocarpal portals (3-4 and 6R) are established.
- Initial Evaluation: A 2.7-mm or 1.9-mm arthroscope is introduced through the 3-4 portal. It is critical to perform the initial diagnostic sweep using a "dry" technique or with very low fluid pressure. High-pressure fluid influx can cause massive extravasation of contaminated fluid into the surrounding soft tissues, potentially creating secondary abscesses or compartment syndrome.

- Debridement and Lavage: Once the portals are secure and outflow is established (often through the 6R portal or a dedicated ulnar outflow portal), an arthroscopic shaver is introduced. Fibrinous debris, hyperplastic infected synovium, and loculations are systematically debrided. The radiocarpal space, including the volar recesses and the prestyloid recess, must be visualized and cleared.

- Midcarpal Assessment: Following radiocarpal debridement, the midcarpal joint must be assessed via the midcarpal radial (MCR) and midcarpal ulnar (MCU) portals. Septic arthritis frequently involves both joint spaces, and failure to debride the midcarpal joint is a common cause of treatment failure.
Closure and Drain Placement
Following exhaustive irrigation of any joint (hand or wrist), the management of the surgical wound is critical. The joint capsule is never tightly closed in the setting of acute infection. It is either left entirely open or loosely approximated with a single absorbable suture to prevent tendon subluxation. The skin may be loosely closed over a small Penrose drain or a vessel loop acting as a wick to allow for continuous egress of residual fluid. In cases of severe, established infection with significant soft tissue compromise, the wound is left open, packed with sterile gauze, and managed with delayed primary closure or healing by secondary intention.
Complications, Incidence Rates, and Salvage Management
Despite aggressive and timely surgical intervention, septic arthritis of the hand and wrist carries a high morbidity rate. The unique anatomy of the hand, with its tightly packed gliding structures, means that even a successfully eradicated infection often leaves the patient with significant functional deficits. The surgeon must counsel the patient extensively preoperatively regarding these highly probable outcomes.
Stiffness is the most ubiquitous complication, arising from a combination of intra-articular fibrosis, capsular contracture, and adhesions of the overlying extensor or flexor tendons. Chondrolysis, the rapid and irreversible destruction of the articular cartilage, leads to rapid-onset secondary osteoarthritis. If the infection breaches the subchondral plate, osteomyelitis ensues, which drastically alters the treatment algorithm and often necessitates bone resection.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage Management & Reconstruction |
|---|---|---|---|
| Severe Joint Stiffness / Ankylosis | 40% - 60% | Arthrofibrosis, capsular scarring, tendon adhesions. Risk increases with delayed drainage (>48 hrs). | Aggressive hand therapy, dynamic splinting. Late: Surgical tenolysis, capsulotomy (only after infection is eradicated). |
| Chondrolysis / Secondary Osteoarthritis | 30% - 50% | Proteolytic degradation by bacterial toxins and host MMPs. | Activity modification, NSAIDs. Late: Arthrodesis (fusion) is the gold standard for pain relief. Arthroplasty is generally contraindicated. |
| Osteomyelitis | 10% - 20% | Direct extension of bacteria into subchondral bone due to delayed treatment or highly virulent organisms (MRSA). | Serial surgical debridement, bone resection, prolonged IV antibiotics (6+ weeks). May require eventual bone grafting or ray amputation. |
| Tendon Rupture | 5% - 10% | Enzymatic degradation of the tendon substance, particularly the extensor mechanism over the MCP/PIP joints. | Staged tendon reconstruction or tendon transfer once the soft tissue envelope is sterile and supple. |
| Systemic Sepsis | < 5% | Hematogenous dissemination from the joint space. Higher risk in immunocompromised or elderly patients. | Emergent ICU admission, broad-spectrum IV antibiotics, hemodynamic support. |
Salvage procedures are strictly reserved for the post-infectious phase, defined by normalized inflammatory markers (CRP/ESR) and a quiescent clinical exam for a minimum of 3 to 6 months. For the destroyed IP or MCP joint, arthrodesis in a functional position (e.g., 30 degrees of flexion for the PIP joint) provides a stable, painless digit, albeit at the cost of motion. Silicone arthroplasty, while an option for non-infectious degenerative joint disease, carries an unacceptably high risk of recurrent infection and hardware failure if placed in a previously septic bed, and is generally avoided.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following drainage of a septic joint is a delicate balancing act. The surgeon and hand therapist must navigate the conflicting goals of immobilizing the joint to allow for soft tissue healing and infection control, versus early mobilization to prevent the devastating complication of arthrofibrosis.
Phase I: Infection Control and Protection (Days 0-7)
Immediately postoperatively, the hand or wrist is placed in a bulky, non-compressive soft dressing and supported by a custom orthosis. For digital infections, the MCP joints are splinted in 70-90 degrees of flexion (to maintain collateral ligament length), and the IP joints in full extension. For wrist infections, a volar resting splint in 10-15 degrees of extension is utilized. The primary focus during this phase is edema control, strict elevation, and administration of targeted intravenous antibiotics based on intraoperative culture sensitivities. Range of motion is restricted to adjacent, uninvolved joints.
Phase II: Early Controlled Mobilization (Weeks 1-4)
Once the clinical signs of acute infection (erythema, severe resting pain) begin to subside and the surgical wounds are stabilizing, early active and active-assisted range of motion (ROM) is initiated. This must be closely supervised by a certified hand therapist. The goal is to encourage tendon gliding and nourish the remaining articular cartilage through synovial fluid diffusion. Passive stretching is strictly avoided during this phase, as it can exacerbate inflammation and damage healing capsular structures. If a drain was placed, it is typically removed within the first 48-72 hours once output becomes minimal and serous.
Phase III: Restoration of Function and Strengthening (Weeks 4-12+)
As the infection is definitively cleared (evidenced by normalizing CRP and clinical exam), the rehabilitation protocol transitions to aggressive ROM and functional restoration. Dynamic or static-progressive splinting may be introduced if significant contractures have developed. Strengthening exercises, initially isometric and progressing to isotonic, are incorporated to rebuild the musculature that rapidly atrophies during the immobilization phase. Patients must be educated that maximal medical improvement may take up to a year, and some degree of permanent stiffness is the rule rather than the exception.
Summary of Landmark Literature and Clinical Guidelines
The evolution of treatment for septic arthritis of the hand and wrist is heavily grounded in both classic orthopedic principles and modern minimally invasive advancements. The foundational understanding of joint destruction kinetics stems from early animal models, which definitively proved that irreversible cartilage damage occurs within 48 hours of bacterial inoculation, establishing the modern mandate for emergent surgical decompression.
In the realm of diagnostic criteria, while the Kocher criteria are classically applied to the pediatric hip, their underlying principles regarding the utility of ESR, CRP, and inability to bear weight (analogous to exquisite pain with passive ROM in the hand) remain highly relevant. The definitive guidelines for synovial fluid analysis, establishing the >50,000 WBC/µL threshold with PMN predominance, remain the cornerstone of diagnosis across all orthopedic subspecialties.
For the wrist specifically, the paradigm shift from open arthrotomy to arthroscopic management is supported by numerous contemporary studies. Landmark papers by authors such as Sammer and Shin have demonstrated that arthroscopic drainage of the septic wrist yields equivalent infection eradication rates to open procedures, but with statistically significant improvements in postoperative range of motion, decreased hospital length of stay, and lower rates of postoperative capsular contracture. These studies reinforce that, in the hands of a skilled arthroscopist, minimally invasive lavage should be considered the first-line surgical intervention for native joint radiocarpal and midcarpal sepsis.
