
Definition
Clubfoot, also known as congenital talipes equinovarus , occurs in approximately 1 in 1000 live births. The clubfoot contains four identifiable components that are easily remembered using the acronym CAVE (cavus, adductus, varus, and equinus). Idiopathic clubfoot contains each of the four components to varying degrees.
The so-called postural clubfoot is held by the infant in an equinovarus position, but all components are nearly completely correctable with gentle manipulation and resolve over time without intervention. A small proportion of clubfeet are teratologic, occurring as part of other neuromuscular diseases, such as Larsen syndrome, any of the arthrogryposis syndromes, and spina bifida. The complex clubfoot, a severe type of idiopathic clubfoot, has a tighter hindfoot and plantar structures.
In 1948, Dr. Ignacio Ponseti began manipulating clubfeet through serial casting, completely correcting the clubfoot deformity. The principles of Ponseti casting lay in gently stretching the soft tissue structures and gradually inducing remolding of the primarily cartilaginous bones of the hindfoot during immobilization. For the definitive publication on clubfoot and the Ponseti technique, the reader is referred to Dr. Ponseti's book. 7 The success of the treatment protocol that bears his name has been borne out through over 30 years of follow-up, establishing it as the standard for initial treatment of clubfoot. 1 In 2006, Dr. Ponseti published a modification to his original casting technique that addresses the specific deformities characteristic of the complex clubfoot. 8
Anatomy
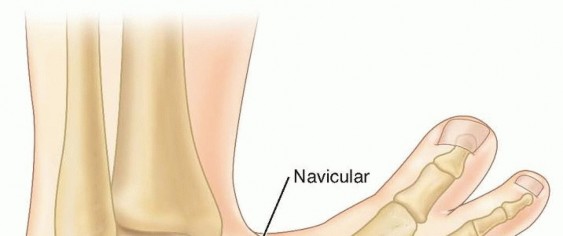
The Achilles and posterior tibialis tendons, as well as the posterior and medial ligaments of the foot between the calcaneus, talus, and navicular, are thickened and fibrotic. 7 The clubfoot contains a number of changes in bony alignment and shape.
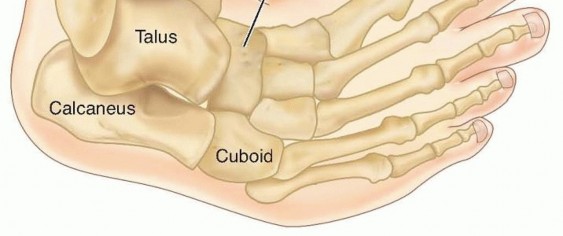
FIG 1: Anatomic alignment in neonatal clubfoot. Note the medial displacement of the navicular and cuboid, the inversion and internal rotation of the calcaneus under the talus, and equinus of the talus and calcaneus.
Relative to normal foot anatomy, the first ray is plantarflexed, generating the cavus deformity. By comparison, all rays are plantarflexed in the complex clubfoot, resulting in full-foot cavus. The navicular is medially displaced on the talus, and the cuboid is medially displaced on the calcaneus as part of the adductus deformity. The medial corners of the head of the talus and the anterior calcaneus are flattened. The calcaneus is inverted under the talus, creating the hindfoot varus, while also being in equinus and elevated in the fat pad of the heel.
In children with unilateral clubfoot, the affected foot usually is smaller, as is the lower leg, relative to the unaffected side. Up to 85% of clubfeet have an insufficient or absent anterior tibial artery. 6
Natural History
The exact cause of the fibrotic changes in clubfoot is unknown. Recently, candidate genes have been identified in familial clubfoot, including Pitx1 and Tbx4 . 3 Left uncorrected, the weight-bearing surface in a clubfoot becomes the dorsolateral surface. Thick callosities develop, and the positioning of the foot creates significant functional disability.
Patient History and Physical Findings
Clubfoot may be identified on prenatal ultrasound as early as 12 to 13 weeks. Half or more of fetuses with clubfeet identified on second-trimester ultrasounds are found to have other anomalies (most commonly cardiac, neurologic, and/or urogenital) or are syndromic/teratologic. 9 The exact sensitivity and specificity of prenatal ultrasound are unknown. False positives are rare on 20-week ultrasounds but may be as high as 40% during the third trimester (when false negatives are rare). 9 Cases not found on prenatal ultrasound are readily identifiable at birth.


FIG 2: Ultrasound at 20 weeks of a child born with clubfoot.
All children with clubfeet should be examined for other findings that may suggest a syndromic or neuromuscular association, such as other contractures or joint dislocations (especially hip dislocation), cutaneous lesions, spinal abnormalities, and abnormal facial features. The clubfoot is easily identified by the combined deformities of cavus, adductus, varus, and equinus.
Consider complex clubfoot if a deep midfoot crease and cavus extend transversely across the entire plantar aspect of the foot, and the foot appears short and broad. The ability to abduct or dorsiflex the foot completely on examination suggests etiologies other than idiopathic clubfoot, such as isolated metatarsus adductus, neuromuscular disease, or focal anatomic abnormalities.
The fat pad of the heel will feel empty upon palpation due to equinus positioning of the calcaneus. This is especially dramatic in the complex clubfoot. The lateral head of the talus is easily palpable over the dorsolateral surface of the foot. More laterally, the anterior calcaneal tuberosity is also palpable. Care must be taken in differentiating these two structures because Ponseti casting necessitates stabilizing the foot over the lateral head of the talus, allowing free motion of the calcaneus under the talus, whereas pressure at the calcaneal tuberosity blocks calcaneal rotation, allowing only forefoot abduction.
The complex clubfoot has a crease that extends transversely across almost the entire plantar aspect of the foot accompanied by full-foot cavus with plantarflexion of all metatarsals. Also, the heel crease is deeper than that of most other clubfeet. During the initial one or two casts, as the adductus is corrected, the first ray in the complex clubfoot becomes retracted, if not noticeably retracted at presentation. The cavus also persists, with all metatarsals remaining plantarflexed.
It is important to examine the clubfoot before each casting to evaluate for the adjustments that must be made during casting to correct residual deformities or to identify and modify casting for a complex clubfoot. A number of classification systems have been introduced as an attempt to predict outcome, but the ability of these systems to evaluate correction, predict recurrence and final function is still unclear. 5 The degree of dorsiflexion and abduction, and the distance of the navicular anterior to the medial malleolus, provide other objective measurements of deformity and correction.
Some children are born with one or both feet held in an equinovarus deformity at birth that is nearly completely correctable on examination. Nearly complete dorsiflexion (more than 20 degrees) is present, although abduction may be slightly limited. The calcaneus is also readily palpable in the fat pad of the heel. These feet may be thought of as "postural" in nature, and most will resolve spontaneously or with parental stretching over 1 to 2 months. If persistent, one or two casts usually correct the deformity, and Achilles tenotomy is rarely required. Feet corrected with casting may require maintenance in a foot abduction orthosis.
Imaging and Other Diagnostic Studies
Clinical examination is sufficient to diagnose the congenital clubfoot. Plain radiographs at birth are not helpful in diagnosing clubfoot because the ossific nuclei of the talus and calcaneus are spherical, so orientation and relationship are not discernible, and the other tarsal bones are unossified.
Once full abduction is obtained by casting, if dorsiflexion of more than 10 degrees is present, forced dorsiflexion lateral films are helpful in differentiating midfoot breach, producing apparent dorsiflexion, from true dorsiflexion occurring at the ankle, obviating the need for a percutaneous Achilles tenotomy.
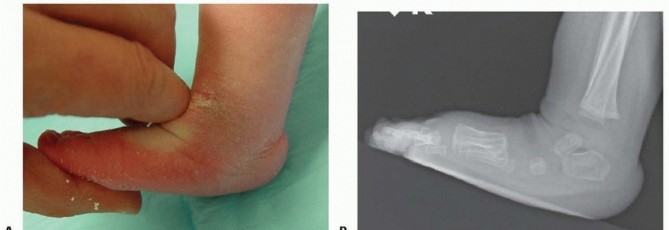
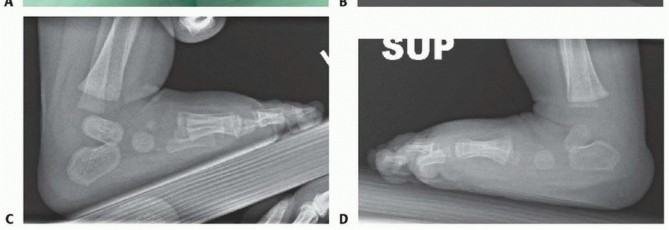
FIG 3: Forced dorsiflexion lateral radiographs to differentiate midfoot breach from true ankle dorsiflexion.
Differential Diagnosis
- Metatarsus adductus
- Neurologic equinovarus or cavovarus deformity: Both deformities may be differentiated from clubfoot by absence of the other components of clubfoot.
- Teratologic or syndromic clubfeet (including neuromuscular disorders): Clubfoot deformity may be more difficult to correct and tends to recur.
- Postural clubfoot
- Complex clubfoot
Nonoperative Management
Ponseti casting of the idiopathic clubfoot involves a specific sequence of corrective maneuvers that correct the deformities of the clubfoot in combination. Each manipulation is maintained with a plaster cast. Ponseti casting ideally begins during infancy, although good results are achievable through toddlerhood. Casting in older children can also produce good results or at least reduce the amount of surgery required for complete correction. An open tendo Achilles lengthening may be more appropriate than a percutaneous tenotomy in children older than 2 years old.
Long-leg casts should always be used to prevent cast slippage and maintain rotational control of the lower leg. Initially, applying a short-leg cast allows focused attention on maintaining foot position and molding before extending the cast above the knee. Padding should be minimal, and plaster is preferable for its ability to be molded precisely to the contours of the foot and ankle.
Four to six casts should correct the cavus, adductus, and varus deformities. If correction is not achieved in eight casts or the child pulls back in the casts, the possibility of an unrecognized complex clubfoot or improper casting technique should be considered. Casting is facilitated by the child being relaxed and calm. Feeding the infant during casting assists in this. For breast-fed infants, it is helpful if the family introduces, and uses once daily, a bottle so the child may feed during casting. If a bottle is not tolerated, other calming measures may be necessary. For older children, music, television, or playing with toys often proves helpful, as does casting with the child sitting upright or on the parent's lap.
**Vascular Check:** Before leaving the clinic, the toes should be checked to make sure they are pink and well perfused. Some toes will become reddish-purple as the casts cool but will become pink if the child is bundled and monitored over 1 hour. Toes that become more purple and dusky indicate that the cast is too tight and should be reapplied.
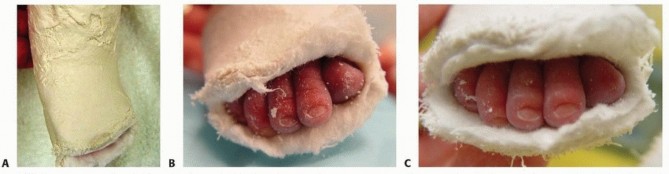
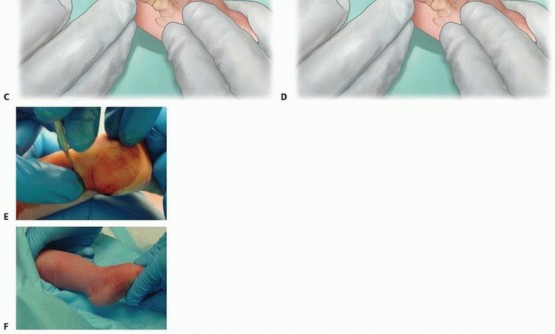
FIG 4: (A) A complex clubfoot that has pulled back in the cast. (B) Purple discoloration of toes after application. (C) Reperfusion and pink toes after the cast temperature stabilizes.
Casts are changed every 5 to 7 days. The final cast, following percutaneous Achilles tenotomy, is left in place for 3 weeks. Almost all clubfeet will require a percutaneous Achilles tenotomy to correct the residual equinus deformity once the other components are corrected. Once complete correction is obtained, correction must be maintained by placing the feet in a foot abduction orthosis. Constructs include straight last shoes, soft ankle-foot orthoses (AFO), or rigid AFOs mounted on rigid or articulating bars.
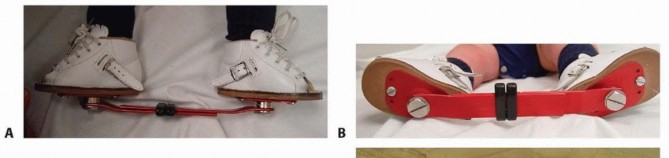
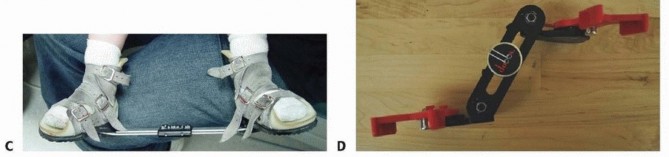
FIG 5: The foot abduction orthosis constructs (straight last shoes attached to a solid bar, and soft AFO options).
Surgical Management
Percutaneous Achilles tenotomy is required in almost all idiopathic clubfeet to correct the residual equinus. About 20% of patients require anterior tibialis tendon transfer at 3 to 4 years old to correct recurrent or persistent dynamic varus deformity.
Preoperative Planning
- Degree of dorsiflexion: If dorsiflexion is less than 10 degrees, a percutaneous Achilles tenotomy is required to correct the residual equinus. If dorsiflexion is more than 10 degrees, forced dorsiflexion lateral foot radiographs help to differentiate midfoot dorsiflexion, with residual calcaneal equinus, from true dorsiflexion occurring at the hindfoot.
- Location & Anesthesia: The risk of anesthesia must be balanced against the perceived pain and duration of the procedure. Approximately half of pediatric orthopedists report performing the percutaneous tenotomy under general anesthesia or conscious sedation. Local analgesia, with 1% lidocaine, affords the opportunity to perform the tenotomy in the clinic setting and avoids any potential risk of general anesthesia.
Positioning
The child should be supine on the table with the contralateral leg held out of the way by the parent or an assistant during tenotomy and casting.
Approach
A medial approach is used to remain posterior to the medial neurovascular bundle.
Techniques
1. Casting
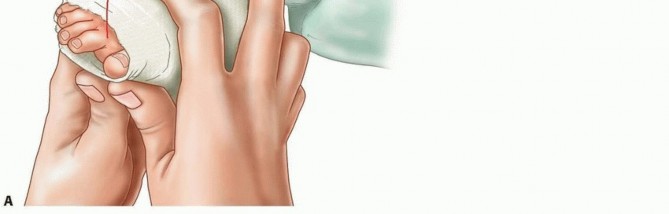
Stretching
Before casting, the foot should be stretched in the same manner as used for immobilization during casting. The thumb of the examiner's contralateral hand should be placed over the head of the talus, and the index finger of the other hand should lie along the medial aspect of the first ray with the second through fourth fingers under the plantar aspects of the forefoot. The calcaneocuboid joint should be avoided, so as not to block subtalar motion. The first casting should focus on elevation of the first ray to correct the cavus deformity. This places the forefoot in supination, locking the midfoot and aligning the forefoot with the hindfoot, allowing for correction of the hindfoot deformities during later abduction maneuvers. Some of the adductus may also be corrected during the first casting.


TECH FIG 1: Proper hand placement during stretching and first cast application for elevation of the first ray.
Lower Leg Cast Application
A thin layer of cotton padding should be applied. The padding is wrapped three times around the toes distally, then extended proximally over the foot and lower leg to pad with no more than two layers of padding. The foot should be held in the position to be casted throughout. The popliteal fossa should be avoided proximally. A thin layer of plaster is applied over the foot and lower leg. The plaster may be applied more loosely over the toes but should be snug over the hindfoot and ankle to immobilize the foot properly and allow for precise molding.
Avoid making the cast too snug so as to impair venous return or apply unnecessary pressure on the fat pad of the heel. The lower leg cast should be precisely molded around the malleoli and above the calcaneus posteriorly. Do not apply pressure over the fat pad of the heel. Throughout, the foot should be held in the position of correction, but the fingers should be in fairly constant motion to prevent pressure spots.


TECH FIG 2: Holding the position of correction while applying thin plaster and molding around the malleoli.
Completing the Cast
Once the lower leg cast has set, padding should be applied over the rest of the leg up to the groin, again in no more than two or three layers. The knee should be held at 90 degrees, and the lower leg should be in slight external rotation. Padding should be minimized in the popliteal fossa to prevent impingement of the neurovascular structures. A plaster splint of three or four layers of plaster roll should be placed over the knee from the proximal thigh to the middle of the shin to strengthen the cast against knee extension while minimizing bulk in the popliteal fossa.
The knee should be molded while held at 90 degrees with the lower leg in slight external rotation until set. Rolling the plaster at the proximal edge of the cast before the plaster sets up completely helps minimize chafing of the thigh.


TECH FIG 3: Extending the cast to a long-leg cast and trimming the distal end to ensure pink, well-perfused digits.
The cast should be trimmed distally to expose the toes. The practitioner should confirm that they are pink and well perfused before the child is sent home. Trimming the plaster over the dorsal aspect too far proximally, beyond the web space, may create a tourniquet effect over the forefoot. Parents should be instructed on signs and symptoms of cast problems before discharge.
Cast Changes and Follow-Up
Casts are typically changed every 7 days, although they may be changed as frequently as every 5 days. Casts should not be removed until just before recasting. Casts can be soaked by the family before coming to the office, then removed with a plaster knife in the clinic. Alternatively, dry casts may be removed with a cast saw, using extreme caution. Having the parents remove the casts the night before results in varied degrees of recurrence overnight and prolongs casting.
After the first casting, the cavus deformity should be nearly, or completely, corrected. If not, adopt complex casting modifications. Stretching is performed with the forefoot in supination, maintaining alignment of all rays, abducting the foot under the talus, again stabilizing the talus laterally. The foot is then casted in the newly maintained position, just to where the foot may be comfortably corrected without significant resistance. Trying to overabduct the foot during a single casting results in intolerance, pressure sores, or vascular compromise.
Each subsequent manipulation results in increased abduction of the forefoot and correction of the hindfoot varus. Throughout, the forefoot should remain in neutral (appearing supinated due to the hindfoot varus) and the hindfoot in equinus. Dorsiflexion of the calcaneus remains blocked under the neck of the talus until approximately 25 degrees of abduction has been obtained. Once abduction of 70 degrees is obtained, correction of the remaining equinus deformity may occur. Overabduction to 70 degrees is necessary to accommodate some of the inevitable recurrence.



TECH FIG 4: Progression of correction through subsequent casts, decreasing varus and equinus and increasing abduction to 70 degrees.
2. Complex Clubfoot Casting
The complex clubfoot may not be immediately recognizable at presentation. Correction usually begins using the standard maneuvers, but within one or two casts, the foot begins to clearly demonstrate a deviation from the expected correction as the cavus persists (involving plantarflexion of all metatarsals) and the first ray becomes retracted. At this point, the technique must be modified.
Lateral counterpressure still occurs at the lateral head and neck of the talus, but stabilization of the fibula should also occur. The index finger of the contralateral hand should be flexed at the proximal interphalangeal joint and placed posterior to the distal fibula. The thumb of the same hand is placed just anterior to the lateral malleolus along the neck of the talus.
After applying cotton padding, a posterior splint of three or four layers of plaster should be applied under the plantar surface of the foot, extending from beyond the tips of the toes proximally over the posterior lower leg. Then, a thin layer of plaster may be wrapped in the usual manner. A minimal amount of plaster should be used because precise molding is even more important for the complex clubfoot.
The pads of the thumbs of both hands are placed under the forefoot, with the pads of the index fingers placed over the dorsal surface of the talar neck. The forefoot is then forcefully dorsiflexed against the counterpressure over the dorsal talar neck, enough to produce blanching of the digits. Upon release of dorsiflexion pressure after setting of the cast, the slight relaxation of the cast should result in revascularization of the digits and pink coloration.
TECH FIG 5: Dorsiflexion force applied to stretch the midfoot in the complex clubfoot, checking for digit blanching and reperfusion.
On extending the cast up over the lower leg, the knee should be flexed to 110 degrees to minimize the ability to pull out of the cast. Tenotomy occurs once the cavus and adductus deformities are corrected and about 40 degrees of abduction is obtained. Attempting to abduct the complex clubfoot beyond 40 degrees results in no further hindfoot correction and only overabducts the forefoot.
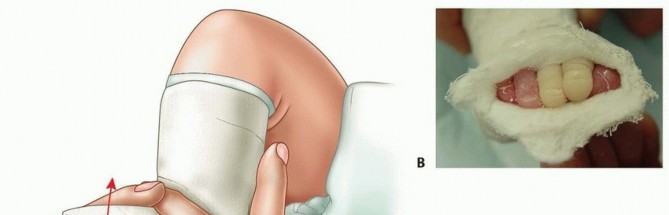
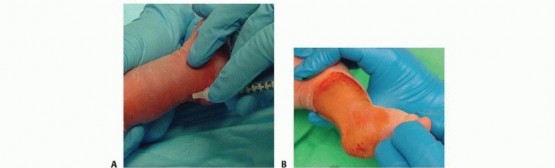
3. Percutaneous Achilles Tenotomy
The tenotomy should occur 1 to 1.5 cm above the insertion of the Achilles on the posterior tuberosity of the calcaneus. Performing the tenotomy too low results in damage to the posterior calcaneal tuberosity. For procedures in the clinic, local anesthesia must be used. A small amount of 1% lidocaine may be injected locally adjacent to the tendon.
An assistant should hold the foot in maximal dorsiflexion to increase tension on the Achilles tendon, making it more easily palpable. A second assistant should hold the contralateral leg and foot out of the field. A thin, sharp scalpel should be used to perform the tenotomy. Cataract surgical blades (5100 or 5400 Beaver blades) are well suited for this procedure, although a no. 11 blade is also acceptable.
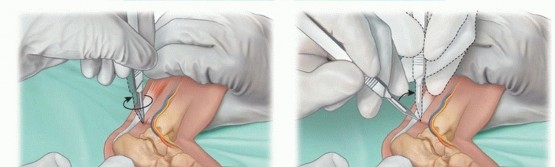


TECH FIG 6: Step-by-step percutaneous Achilles tenotomy under local anesthesia, blade positioning, transection, and post-tenotomy cast molding.
Once the blade is oriented perpendicular to the fibers of the Achilles tendon, the safest maneuver involves pressing the tendon onto the blade using the contralateral thumb. Complete transection often results in a palpable "pop," release of the Achilles tendon, and an immediate increase of 15 to 20 degrees of dorsiflexion. A palpable defect in the tendon confirms complete transection.
Casting After Tenotomy: The lower leg is wrapped with sterile cotton, accommodating the increased dorsiflexion. The plaster is applied in the usual manner and molded well at the anterior ankle to prevent pulling back in the cast. Extension of the cast above the thigh as a long-leg cast should occur with the knee in the usual 90 degrees of flexion (110 degrees for complex clubfoot). The post-tenotomy cast should be left on for 3 weeks before removal to allow tendon healing.


TECH FIG 7: Final long-leg casting and complete correction obtained three weeks post-tenotomy.
Pearls and Pitfalls
- Failure to correct the cavus deformity with initial casting: Failure to elevate the first ray will result in worsening cavus during abduction, and only the forefoot will abduct. The hindfoot varus will fail to correct. The foot will then pull back in the cast.
- Toes turn purple after cast application (see FIG 4): Some neonatal feet have poor vascular control and will turn purple as the cast cools. Do not be too hasty to remove the cast. Bundle the child, elevate the feet, and recheck every 15 minutes. Increasing purplish discoloration indicates a cast that is too tight and should be removed and reapplied.
- An older child who resists casting: A child who fights casting prevents good molding, and too much motion may prevent the cast from setting up in the desired position. A quiet room with music, entertaining the child with a toy, or feeding may relax the child.
- Child pulling out of foot abduction orthosis: Add padding in the heel, above the posterior calcaneal tuberosity, use a shoe with a heel cutout, or both. If the child has a strong propensity for toe curling, try a Plastazote plate under the toes to keep them extended.
- Child cries while in casts or in bar and shoes: Make sure the toes are well perfused. Discomfort for 24 hours after the first casting or tenotomy is common and easily relieved with acetaminophen. If the child is in an orthosis, examine the feet for sores. Feet may be hyperesthetic after casting: massage during diaper changes accelerates desensitization.
- Recurrence: Monitor for decreases in abduction and dorsiflexion. Treating an early identified, minimal recurrence with stretching by the parents with every diaper change may prevent progression. Later or more marked recurrence should be treated with recasting and possibly a second percutaneous tenotomy.
Postoperative Care
After removal of the post-tenotomy cast, the child should immediately be placed in a foot abduction orthosis. Acceptable constructs include straight last shoes or AFOs connected to a solid or articulated bar.
In the case of bilateral corrected clubfeet, both shoes should be placed in abduction/external rotation on the bar to the degree of comfortable correction, typically 60 to 70 degrees. For unilateral clubfoot, only the shoe of the affected foot is placed near the extreme of abduction; the shoe of the normal foot is placed at 30 degrees.
Only a single, thin pair of socks should be worn with the shoes. For the first week, the orthosis and socks should be removed with every diaper change to inspect the feet for evidence of developing pressure sores. Red spots that do not disappear within 5 minutes signal a potential problem spot and require refitting of the shoes with Plastazote or repositioning on the bar.
After the first week, the orthosis should be worn full time, but it may be removed once daily for bathing and a short period of play (1 to 2 hours). Full-time wear continues for 3 to 4 months to maintain correction. After 3 months of full-time wear and maintenance of full correction, children wear the orthosis for 16 hours per day, primarily at nighttime and during naps. Part-time wear continues until the child is 4 years old, when orthosis wear may be discontinued.
Outcomes
A corrected clubfoot tends to recur to its original position, requiring maintenance of correction in the orthosis. Noncompliance with bar-and-shoe wear increases the likelihood of recurrence to more than 80%. Compliance is increased with close follow-up and explicit discussions with the family and all caregivers. 4 Twenty percent to 50% of corrected clubfeet will require anterior tibialis tendon transfer to correct dynamic varus present during ambulation.
Complications
- Cast sores, cast saw burns.
- Prolonged casting or pulling back in the cast due to improper technique, unrecognized clubfoot, or failure to modify casting for complex clubfoot.
- Overabduction from unrecognized complex clubfoot or overabduction in foot abduction orthosis (beyond degree of correction).
- Posterior tibial artery impingement.
- Peroneal artery or lesser saphenous vein laceration during tenotomy. 2
- Recurrence due to incomplete correction or lack of orthosis wear.
Scientific References
- Cooper DM, Dietz FR. Treatment of idiopathic clubfoot. A thirty-year follow-up note. J Bone Joint Surg Am 1995;77(10):1477-1489.
- Dobbs MB, Gordon JE, Walton T, et al. Bleeding complications following percutaneous tendo Achilles tenotomy in the treatment of clubfoot deformity. J Pediatr Orthop 2004;24:353-357.
- Dobbs MB, Gurnett CA. Genetics of clubfoot. J Pediatr Orthop B 2012;21:7-9.
- Dobbs MB, Rudzki JR, Purcell DB, et al. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone Joint Surg Am 2004;86-A(1):22-27.
- Flynn JM, Donohoe M, Mackenzie WG. An independent assessment of two clubfoot-classification systems. J Pediatr Orthop 1998;18: 323-327.
- Greider TD, Siff SJ, Gerson P, et al. Arteriography in club foot. J Bone Joint Surg Am 1982;64(6):837-840.
- Ponseti IV. Congenital Clubfoot: Fundamentals of Treatment. New York: Oxford University Press, 1996.
- Ponseti IV, Zhivkov M, Davis N, et al. Treatment of the complex idiopathic clubfoot. Clin Orthop Relat Res 2006;451:171-176.
- Treadwell MC, Stanitski CL, King M. Prenatal sonographic diagnosis of clubfoot: implications for patient counseling. J Pediatr Orthop 1999;19:8-10.
- Zionts LE, Sangiorgio SN, Ebramzadeh E, et al. The current management of idiopathic clubfoot revisited: results of a survey of the POSNA membership. J Pediatr Orthop 2012;32:515-520. [View Source / PubMed]
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding ponseti-casting