Anterior Tibialis Tendon Transfer to Lateral Cuneiform: A Masterclass in Residual Clubfoot Correction

Key Takeaway
This masterclass details the anterior tibialis tendon transfer to the lateral cuneiform for residual clubfoot. We'll cover comprehensive anatomy, meticulous preoperative planning, precise intraoperative technique for tendon harvest and fixation, and crucial pearls for success. Fellows will learn to address dynamic forefoot supination, understand neurovascular risks, and manage postoperative rehabilitation, ensuring optimal outcomes for challenging clubfoot deformities.
Comprehensive Introduction and Patho-Epidemiology
The management of congenital talipes equinovarus (clubfoot) has undergone a paradigm shift over the last several decades, largely driven by the widespread adoption of the Ponseti method. However, despite meticulous adherence to serial casting and bracing protocols, orthopedic surgeons are frequently confronted with a common, complex, and frustrating sequela: the residual or recurrent clubfoot deformity. The incidence of this residual deformity is not trivial; contemporary epidemiological data suggest it ranges significantly from 26.6% to a highly challenging 50% in certain cohorts. This broad statistical variance reflects the inherent heterogeneity in the initial severity of the clubfoot presentation, the diverse treatment modalities historically employed (ranging from comprehensive posteromedial releases to conservative casting), and the varying clinical definitions of what precisely constitutes a "residual deformity" in the growing child.
When we discuss residual clubfoot deformity, we are not addressing a singular pathological entity, but rather a spectrum of biomechanical deviations. This spectrum encompasses isolated hindfoot equinus, midfoot cavus, persistent metatarsus adductus, and, most pertinent to the surgical masterclass presented in this chapter, dynamic forefoot supination. These deformities can manifest insidiously, often presenting with or without a history of prior extensive soft tissue releases. The primary objective of the anterior tibialis tendon transfer (ATTT) is twofold and must be executed with uncompromising precision. First, the surgeon must meticulously correct any existing fixed bony or soft-tissue deformity—a tendon transfer will inevitably fail if expected to overcome a rigid contracture. Second, we must precisely rebalance the dynamic muscle forces acting across the midfoot and hindfoot, thereby correcting the dynamic supination, neutralizing the deforming vectors, and restoring plantigrade foot alignment and functional gait mechanics.
Understanding the pathogenesis of these residual deformities is paramount. It is rarely a simple case of a "failed initial intervention." Rather, it is a manifestation of dynamic muscle imbalances that may not have been fully apparent during infancy, or a reflection of the unrelenting natural history of an intrinsically resistant or atypical clubfoot. The primary causes of recurrence are either initial undercorrection of the deformity (particularly incomplete reduction of the talonavicular joint) or a true biological recurrence driven by fibrotic soft-tissue remodeling. Electromyographic (EMG) and histological studies consistently demonstrate that the peroneal muscle group (the primary everters) is often relatively weaker or hypoplastic compared to the robust tibialis anterior muscle. This inherent power mismatch exacerbates the supinator action of the tibialis anterior, creating a relentless dynamic deforming force during the swing phase of gait.
Furthermore, medial subluxation of the navicular is a critical pathomechanical factor. This skeletal malalignment influences both the cosmetic appearance of the foot and the functional lateral rotation of the ankle mortise. In approximately 10% of pathological anatomical specimens, the anterior tibialis muscle exhibits an atypical, aberrantly medial insertion into the first metatarsal and medial cuneiform. This anatomic variation inherently optimizes its force vector for supination rather than pure dorsiflexion. We must also maintain a high index of suspicion for underlying neuromuscular syndromes. Patients presenting with myelomeningocele, cerebral palsy, Larsen syndrome, or occult tethered cord syndrome are at a significantly elevated risk for recurrence. The timing of these residual deformities is also predictable; they typically emerge within the first year after the cessation of initial treatment, usually presenting before the age of five, even in feet that were initially judged to be perfectly corrected. If left untreated, these dynamic, flexible deformities will inevitably progress to rigid, arthritic, inverted feet requiring complex osseous salvage procedures.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the surgical anatomy is the absolute foundation for executing a successful anterior tibialis tendon transfer. The intricate relationships between the musculotendinous units, the neurovascular bundles, and the underlying osteology dictate both the efficacy of the transfer and the safety of the surgical approach.
The Anterior Tibialis Muscle-Tendon Unit
The anterior tibialis muscle is a massive, bipennate structure originating from the upper two-thirds of the lateral surface of the tibia, the adjacent interosseous membrane, and the deep fascia of the leg. In a normal physiological state, it functions as the primary, powerful dorsiflexor of the ankle and a secondary invertor of the foot. However, the true biomechanical brilliance of this muscle lies in the microscopic and macroscopic architecture of its tendon. As the anterior tibialis tendon descends toward the ankle, its fibers undergo a remarkable, obligatory 90-degree rotation from the musculotendinous junction all the way to its distal osseous insertion.
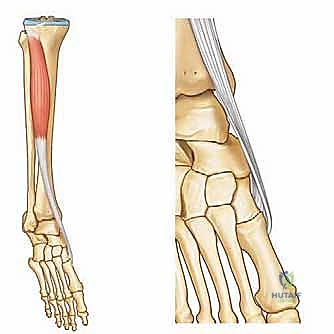
This 90-degree rotation is crucial for understanding its biomechanical action and for properly harvesting the tendon during surgery. The muscle fibers that originate most medially in the proximal leg rotate to form the posterior surface of the tendon near the level of the ankle joint. They continue this spiral rotation distally, ultimately inserting as the distal-lateral fibers on the base of the first metatarsal. Conversely, the muscle fibers originating most laterally in the proximal leg rotate to form the anterior surface of the tendon at its midpoint, continuing distally to insert on the medial cuneiform as the proximal-medial fibers. This complex rotation explains why, in a normal foot, the anterior tibialis acts primarily as a dorsiflexor. It fires concentrically during the initiation of the swing phase to elevate the foot and clear the ground, and then transitions to an eccentric contraction from heel strike to foot flat, smoothly controlling the descent of the forefoot against gravity and the powerful antagonist pull of the gastrocsoleus complex.
The Biomechanics of Residual Supination
In the specific context of residual clubfoot, a critical biomechanical shift occurs that completely alters the function of the anterior tibialis. Dynamic forefoot supination, the primary target of our surgical intervention, is intrinsically linked to the residual medial displacement of the navicular bone on the head of the talus. This persistent medial displacement effectively alters the anatomical line of pull of the anterior tibialis tendon. Because its insertion on the medial cuneiform and first metatarsal is significantly medially displaced relative to the mechanical axis of the ankle and subtalar joints, the anterior tibialis loses its mechanical advantage as a primary dorsiflexor.
Instead, due to this medially shifted vector, the anterior tibialis becomes a potent, unopposed forefoot supinator. Every time the child attempts to dorsiflex the foot during the swing phase of gait, the foot violently supinates. This pathological biomechanical effect is frequently compounded by a relative, sometimes profound, weakness of the peroneal muscles (peroneus longus and brevis), which normally act as the primary antagonists to everte the foot and balance the medial column. By transferring the insertion of the anterior tibialis laterally to the lateral cuneiform, we neutralize this supinating vector and restore the muscle's primary function as a pure, balanced dorsiflexor.
Neurovascular Structures at Risk
During the surgical approach and the subsequent subcutaneous routing of the tendon, the surgeon must maintain acute spatial awareness of the regional neurovascular anatomy to prevent catastrophic iatrogenic injury.
* Deep Peroneal Nerve: This critical nerve courses alongside the anterior tibial artery and veins, deep to the anterior tibialis tendon. It typically lies in the fascial interval between the tibialis anterior and the extensor hallucis longus (EHL). It provides motor innervation to the tibialis anterior, EHL, extensor digitorum longus (EDL), and peroneus tertius, while providing sensory innervation to the first dorsal web space. Aggressive retraction or blind dissection in this interval can lead to permanent foot drop and sensory deficits.
* Anterior Tibial Artery and Veins: These vessels accompany the deep peroneal nerve. Iatrogenic laceration or aggressive traction can lead to significant hemorrhage, compartment syndrome, or compromise of distal pedal perfusion.
* Superficial Peroneal Nerve: This nerve typically pierces the deep fascia in the distal third of the lateral leg to become superficial, providing sensation to the vast majority of the dorsum of the foot. Its medial and lateral dorsal cutaneous branches are at high risk during the lateral incision over the cuneiform and during the blunt subcutaneous tunneling process. Careful, superficial blunt dissection is paramount.
Relevant Osteology and Joint Relationships
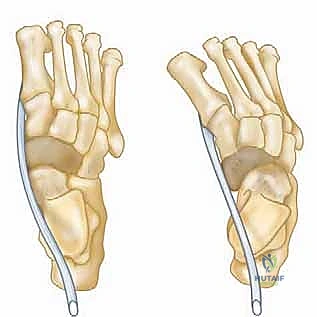
Beyond the soft-tissue dynamics, surgical planning requires a deep appreciation of the bony abnormalities that are pathognomonic of residual clubfoot. The subtalar joint often features an absent anterior facet and severely hypoplastic, narrow medial and posterior facets. This osseous deformity severely restricts subtalar motion, preventing the calcaneus from fully everting and locking the hindfoot in varus, which perpetuates the medial displacement of the navicular.

The navicular itself is frequently wedge-shaped and remains medially subluxated along with the entire distal cuneiform-metatarsal complex. This medial displacement is the structural anchor that profoundly favors the supinator action of the anterior tibialis over its dorsiflexion capabilities. Finally, the lateral cuneiform is our specific anatomical target for the tendon transfer. It is biomechanically superior to the cuboid, as transferring to the cuboid frequently results in severe overcorrection into a pes planovalgus deformity. However, the lateral cuneiform must be adequately ossified to provide a secure, robust anchor site for the tendon. Consequently, we typically delay this procedure until the child's lateral cuneiform ossification center has radiographically appeared and is of sufficient size, which generally occurs between 2.5 to 4 years of age.
Exhaustive Indications and Contraindications
The decision to proceed with an anterior tibialis tendon transfer must be predicated on a rigorous, multifaceted clinical examination. The success of this procedure relies entirely on selecting the correct patient with the correct biomechanical deficit.
Clinical Presentation and Gait Analysis
Gait analysis is the absolute cornerstone of preoperative decision-making. The surgeon must observe the child walking barefoot, ideally in a long hallway where multiple gait cycles can be analyzed unhindered. The pathognomonic finding is dynamic forefoot supination during the swing phase of gait. As the child attempts to clear the foot, the tibialis anterior fires, but instead of pure dorsiflexion, the medial border of the foot elevates violently, and the child lands on the lateral border of the foot. This dynamic observation directly confirms that the anterior tibialis is acting as a deforming supinator and verifies the appropriateness of a lateral transfer.




Upon static physical examination, the surgeon must meticulously evaluate the foot's appearance. Look for persistent forefoot supination, hindfoot equinus, and hindfoot varus. Equinus deformity is often difficult to quantify initially, as a midfoot breech (a "rocker-bottom" deformity) can mask true hindfoot equinus. When equinus is combined with inversion, hindfoot varus will inevitably recur. The navicular-malleolar distance should be palpated; in maximum pronation or supination, this distance is significantly decreased compared to a normal foot. In severe cases, the medial malleolus may even be difficult to delineate due to direct bony contact with the subluxated navicular, indicating profound medial displacement. Additionally, note the calf size and foot morphology. A severely atrophic calf or a short, fat foot with a deep, unyielding plantar crease extending from medial to lateral are indicators of a severe, atypical clubfoot that may be highly resistant to standard interventions.
Specific Clinical Tests
Two specific clinical parameters must be met before considering a transfer. First, the strength of the tibialis anterior must be explicitly tested. For a successful tendon transfer, the donor muscle must possess at least Grade 4 (ideally Grade 5) motor power. Transferring a weak, fibrotic muscle will result in a foot that is neither supinating nor dorsiflexing, leading to a permanent foot drop. Second, and crucially, the surgeon must assess the passive range of motion (ROM) of the ankle and subtalar joints. A tendon transfer is a dynamic balancing procedure; it will never overcome a fixed, rigid bony or soft-tissue contracture. The foot must be passively correctable to a plantigrade position, with full passive dorsiflexion to neutral (0 degrees) or beyond. If fixed equinus or fixed varus is present, these must be addressed concurrently (e.g., via Achilles tendon lengthening or posterior release) or prior to the tendon transfer.
| Category | Specific Clinical Parameters |
|---|---|
| Absolute Indications | Dynamic forefoot supination during swing phase; Passively correctable foot deformity; Tibialis anterior strength ≥ Grade 4; Age > 2.5 years (ossified lateral cuneiform). |
| Relative Indications | Recurrent clubfoot following Ponseti casting; Mild flexible hindfoot varus correctable with forefoot balancing; Failure of conservative bracing protocols. |
| Absolute Contraindications | Fixed, rigid bony deformities (e.g., rigid equinovarus); Weak or paralyzed tibialis anterior (< Grade 4); Unossified lateral cuneiform; Active local soft-tissue infection. |
| Relative Contraindications | Severe, untreated underlying neuromuscular disorders (e.g., un-tethered spinal cord); Severe midfoot cavus requiring primary osseous correction. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential to anticipate intraoperative challenges and ensure optimal biomechanical outcomes. This phase involves a combination of radiographic analysis, clinical templating, and strategic patient positioning.
Radiographic Analysis and Templating
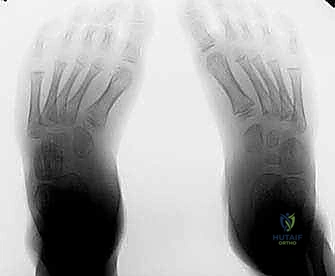
Standard weight-bearing anteroposterior (AP) and lateral radiographs of both feet are mandatory. On the AP view, the surgeon must evaluate the talocalcaneal angle (Kite's angle) and the talonavicular coverage angle to assess the degree of residual hindfoot varus and midfoot adduction. On the lateral view, the talocalcaneal angle and the calcaneal pitch are evaluated to quantify residual equinus or cavus.
Crucially, the radiographs must be scrutinized to confirm the presence and size of the lateral cuneiform ossification center. The lateral cuneiform is the designated target for the transfer because it lies centrally in the midfoot, providing a balanced dorsiflexion vector without inducing excessive valgus. If the ossification center is absent or too small to accept a drill hole and fixation device, the surgery must be postponed. The surgeon must also decide preoperatively on the method of fixation. While traditional techniques utilized a pull-out suture tied over a plantar felt button, modern approaches often employ bioabsorbable interference screws or suture anchors, which eliminate the risk of plantar skin necrosis and reduce postoperative discomfort.
Patient Positioning and Setup
The procedure is performed under general anesthesia. The patient is positioned perfectly supine on the operating table. A small gel bump or folded blanket is placed under the ipsilateral hip to internally rotate the leg slightly; this brings the foot into a neutral, upward-facing position, allowing simultaneous access to both the medial and lateral aspects of the foot without requiring the surgeon to constantly internally rotate the leg against resistance.
A well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, which is critical for identifying the delicate neurovascular structures and the fascial compartments during the tendon harvest and routing. The entire lower extremity is prepped and draped in a standard sterile fashion, ensuring the toes are exposed to assess capillary refill and tensioning during the final fixation steps. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the anterior tibialis tendon transfer requires meticulous soft-tissue handling, precise tendon routing, and rigid osseous fixation. The procedure can be conceptually divided into tendon harvest, subcutaneous routing, and lateral cuneiform fixation.
Incisions and Tendon Harvest
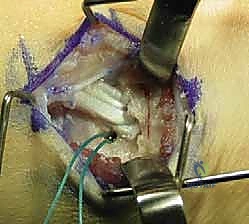
The procedure begins with the identification and release of the distal insertion of the anterior tibialis tendon. A 3 to 4 cm longitudinal incision is made over the medial aspect of the foot, centered over the talonavicular joint and extending distally to the base of the first metatarsal.

Careful blunt dissection is utilized to protect the terminal branches of the saphenous nerve and the medial marginal vein. The sheath of the anterior tibialis tendon is incised longitudinally. The tendon is traced to its broad, bifurcated insertion on the plantar-medial aspect of the medial cuneiform and the base of the first metatarsal.

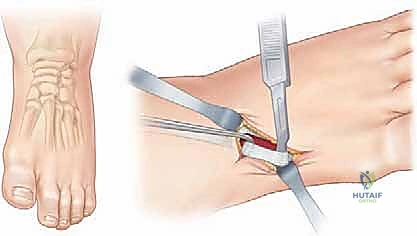
Using a scalpel, the tendon is sharply detached directly off the bone to maximize its length. It is critical to harvest the entire insertion, including the plantar slips, to ensure sufficient length for the transfer. Once detached, the distal end of the tendon is secured with a heavy, non-absorbable locking whipstitch (e.g., #1 or #0 FiberWire or Ethibond).
A second, 3 cm longitudinal incision is then made vertically over the anterior distal third of the leg, just proximal to the superior extensor retinaculum, overlying the anterior tibialis muscle belly. The deep fascia is incised, and the tendon is identified. By placing traction on the whipstitch in the distal wound, the tendon is easily identified in the proximal wound and smoothly pulled proximally out of its sheath, effectively extracting it from the medial foot.
Subcutaneous Tunneling and Routing
The next phase is routing the tendon to its new lateral insertion. A third longitudinal incision (approximately 3 cm) is made over the dorsolateral aspect of the midfoot, centered precisely over the lateral cuneiform. The lateral cuneiform is identified by palpating the base of the third metatarsal and moving proximally. Intraoperative fluoroscopy can be used to confirm the correct bone.

A large Kelly clamp or a specialized tendon passer is introduced into the lateral midfoot incision and directed proximally and medially toward the proximal leg incision. Crucially, the passer must be routed deep to the superior extensor retinaculum but superficial to the periosteum and neurovascular bundle. Routing the tendon deep to the retinaculum is mandatory to prevent anterior bowstringing of the tendon across the ankle joint during dorsiflexion, which would significantly compromise its mechanical advantage and create a cosmetic deformity. The whipstitch sutures are grasped, and the tendon is pulled smoothly from the proximal leg wound, under the retinaculum, and out through the lateral midfoot wound. The tendon should glide freely without any fascial tethering.
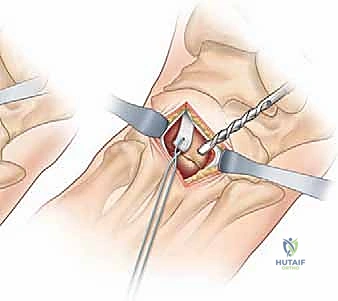
Preparation of the Lateral Cuneiform and Fixation
With the lateral cuneiform exposed, the periosteum is incised and elevated locally. A drill hole is created in the exact center of the lateral cuneiform ossification center. The size of the drill bit (typically 3.5 mm to 4.5 mm) is chosen to precisely match the diameter of the harvested tendon to ensure a tight, biological interference fit. The drill hole is directed from dorsal to plantar, aiming slightly medially to exit through the plantar aspect of the foot.
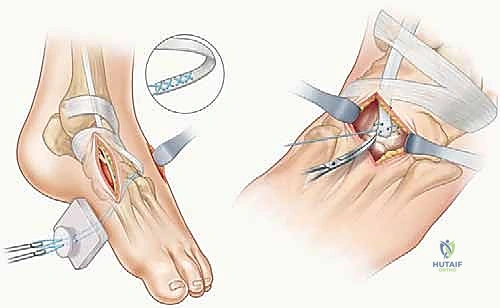
The technique for fixation depends on surgeon preference. If a pull-out button technique is used, straight Keith needles are threaded with the whipstitch sutures, passed through the drill hole, and pushed out through the plantar skin. The foot is then held in maximal dorsiflexion and slight eversion (approximately 5 to 10 degrees of valgus) to neutralize the supinator force. While holding this rigid position, the tendon is pulled taut into the drill hole, and the sutures are tied tightly over a heavily padded felt button on the plantar aspect of the foot.

Alternatively, modern techniques utilize a bioabsorbable interference screw. The tendon is pulled into the drill hole under identical tension, and the interference screw is advanced over a guidewire alongside the tendon, locking it rigidly within the osseous tunnel. This method eliminates the plantar button and allows for earlier weight-bearing in some protocols. Regardless of the fixation method, the foot must rest naturally in a neutral, plantigrade position once the tension is set. The wounds are then copiously irrigated and closed in layers, utilizing absorbable subcutaneous sutures and a running subcuticular closure for the skin.
Complications, Incidence Rates, and Salvage Management
While the anterior tibialis tendon transfer is generally a highly successful and reliable procedure, it is not without potential complications. Meticulous surgical technique and strict adherence to indications are required to minimize these risks. Complications can be broadly categorized into biomechanical failures (undercorrection or overcorrection), technical failures (loss of fixation), and soft-tissue issues.
The most concerning biomechanical complication is over
