David Ring MD: Expert Insights on Clavicle Plate Fixation
Key Takeaway
This topic focuses on David Ring MD: Expert Insights on Clavicle Plate Fixation, Displaced, comminuted clavicle fractures are breaks in the S-shaped collarbone, often from direct shoulder blows. They carry a 10-20% risk of nonunion or malunion, which can lead to shoulder deformity, weakness, or brachial plexus compression. Such fractures may require open reduction and internal fixation, as explained by experts like david ring md.
David Ring MD: Expert Insights on Clavicle Plate Fixation
Introduction and Epidemiology
Clavicle fractures represent a common injury, accounting for approximately 2-5% of all adult fractures and 35-44% of shoulder girdle injuries. These fractures exhibit a bimodal distribution, with peaks in incidence observed in young males engaged in high-energy sports or motor vehicle collisions, and in older females experiencing low-energy falls. While many clavicle fractures can be managed non-operatively with favorable outcomes, a subset, particularly those that are displaced and comminuted, are at significantly elevated risk for complications such as nonunion and symptomatic malunion. These specific fracture patterns warrant careful consideration for open reduction and internal fixation (ORIF) with plate and screw constructs (3, 4, 6, 8, 9, 11). The evolution of surgical techniques and implant design, coupled with a clearer understanding of the biomechanical consequences of displaced fractures, has expanded the indications for operative intervention in appropriate patient populations. This comprehensive review aims to delineate the current understanding and best practices for the surgical management of clavicle fractures.
Surgical Anatomy and Biomechanics
The clavicle is a unique long bone that serves as the sole osseous connection between the axial skeleton and the upper extremity, effectively linking the sternum to the scapula. This connection is reinforced by the strong coracoclavicular and acromioclavicular ligaments, which are crucial for scapular suspension and overall shoulder girdle stability. Phylogenetically, clavicles are present only in brachiating animals, suggesting their primary role in holding the upper limb away from the trunk, thereby enhancing the global positioning and wide range of motion inherent to upper extremity function.
Clavicular Morphology and Key Features
The clavicle is named for its distinctive S-shaped curvature, reminiscent of the musical symbol clavicula. It exhibits an apex anteromedially and an apex posterolaterally. The larger medial curvature is critically important as it widens the space for the passage of vital neurovascular structures, including the brachial plexus, subclavian artery, and subclavian vein, from the neck into the upper extremity through the costoclavicular interval.
In terms of bone composition, the clavicle is characterized by very dense trabecular bone, notably lacking a well-defined medullary canal, which distinguishes it from most other long bones. Its cross-sectional morphology changes gradually along its length: a flat lateral aspect, a tubular midportion, and an expanded prismatic medial end. This anatomical variation dictates specific considerations for plate contouring and screw placement.
The clavicle is subcutaneous throughout its entire length, making it susceptible to direct trauma and contributing significantly to the aesthetic contour of the neck and upper part of the chest. This superficial location also has implications for surgical planning, as hardware prominence can be a significant post-operative concern.
Neurovascular Structures and Ligamentous Attachments
A critical anatomical consideration during surgical exposure is the identification and protection of the supraclavicular nerves. These sensory branches of the cervical plexus run obliquely across the clavicle just superior to the platysma muscle. Meticulous dissection to identify and preserve these nerves is paramount to mitigate the development of post-operative hyperesthesia or dysesthesia over the chest wall, a common and often bothersome complication. Deeper to the clavicle, particularly medially, lie the aforementioned subclavian vessels and brachial plexus. Extreme caution must be exercised when drilling or placing screws, especially on the inferior cortex, to avoid iatrogenic neurovascular injury.
The clavicle's stability is heavily reliant on its ligamentous attachments. Medially, the sternoclavicular joint is stabilized by the anterior and posterior sternoclavicular ligaments and the costoclavicular ligament. Laterally, the acromioclavicular joint is stabilized by the superior and inferior acromioclavicular ligaments, and the trapezius and deltoid muscles. However, the most critical stabilizers for clavicle fracture management are the coracoclavicular ligaments—the conoid and trapezoid ligaments—which originate from the coracoid process of the scapula and insert onto the inferior aspect of the lateral clavicle. These ligaments are crucial for suspending the scapula from the clavicle and are often disrupted in lateral clavicle fractures, or their integrity must be respected during fixation of midshaft fractures.
Pathogenesis and Biomechanical Consequences of Fractures
Clavicle fractures usually result from a direct blow to the point of the shoulder, transmitting force axially through the clavicle. This mechanism typically produces moderate- to high-energy injuries in younger adults. In older individuals, particularly those with osteopenia or osteoporosis, a low-energy fall from a standing height can similarly result in a clavicle fracture.
The biomechanical consequence of a completely displaced midshaft clavicle fracture is significant. The absence of cortical apposition results in a lack of mechanical stability and load transfer. The pulling forces of the sternocleidomastoid muscle medially, and the weight of the upper extremity along with the pull of the pectoralis major and latissimus dorsi muscles laterally, typically result in superior displacement of the medial fragment and inferior, anterior, and medial displacement of the lateral fragment. This displacement often leads to shortening and angulation, which can impair shoulder function by altering the mechanical axis of the shoulder girdle and leading to symptomatic malunion. The overall nonunion rate for diaphyseal clavicle fractures is reported around 4.5% (9). This risk is amplified significantly in cases of complete displacement (no apposition) and comminution, particularly with superior displacement exceeding 20 mm, shortening greater than 15-20 mm, or significant comminution (9). Further risk factors for nonunion include increasing age, female gender, and high-energy trauma.

Indications and Contraindications
The decision to proceed with operative management for clavicle fractures involves a careful assessment of fracture characteristics, patient factors, and potential risks versus benefits. While non-operative treatment remains the standard for many minimally displaced and stable patterns, a growing body of evidence supports operative intervention for specific unstable fracture configurations to improve union rates and functional outcomes.
Indications for Operative Fixation
The primary goal of operative fixation is to restore anatomical alignment, provide stable fixation, and facilitate early rehabilitation, thereby minimizing the risk of nonunion and symptomatic malunion.
- Complete Displacement: Fractures with greater than 100% displacement (no cortical apposition) are at significantly higher risk for nonunion and often develop symptomatic malunion with associated shoulder girdle dysfunction.
- Significant Shortening: Clavicle shortening exceeding 15-20 mm (or 2 cm) can lead to functional deficits, altered scapular kinematics, and nerve impingement symptoms.
- Significant Comminution: Multifragmentary fractures, particularly those with a "Z-fragment," often lack inherent stability and have increased nonunion rates.
- Open Fractures: These require urgent surgical debridement and stabilization to prevent infection and promote healing.
- Neurovascular Compromise: While rare, fractures associated with injury to the brachial plexus or subclavian vessels necessitate immediate surgical exploration and repair, followed by fracture stabilization.
- Polytrauma or Floating Shoulder: In polytrauma patients, stable clavicle fixation can facilitate nursing care and overall rehabilitation. A "floating shoulder" (ipsilateral clavicle and scapular neck fracture) often benefits from clavicle fixation to restore shoulder girdle stability.
- Pathologic Fractures: Fractures through neoplastic lesions, once appropriate oncologic workup is performed, often require stabilization.
- Symptomatic Malunion or Nonunion: Previously missed or failed non-operative treatment resulting in pain, weakness, or functional limitations warrants surgical intervention.
- Skin Tenting or Impending Skin Breakdown: Sharply angulated fragments that compromise skin integrity require reduction and fixation.
- Patient Factors: Professional athletes or highly active individuals may benefit from operative fixation to facilitate a faster and more predictable return to sport, though this remains a relative indication.
Contraindications for Operative Fixation
Absolute contraindications for clavicle ORIF are few but include:
- Active Local or Systemic Infection: Surgical intervention should be deferred until infection is controlled.
- Severe Comorbidities: Patients with medical conditions precluding safe anesthesia or surgery (e.g., severe cardiopulmonary disease).
- Poor Skin Condition: Compromised skin surrounding the fracture site (e.g., severe abrasions, burns) may necessitate delayed surgery or alternative fixation methods.
Relative contraindications include:
- Minimally Displaced or Nondisplaced Fractures: These generally heal well with non-operative management.
- Extremely Comminuted Fractures: In some cases of severe comminution, especially with bone loss, plate fixation may be challenging and alternative strategies (e.g., external fixation or limited internal fixation with bone grafting) might be considered, though this is rare for the clavicle.
- Non-compliant Patient: Patients unable to adhere to post-operative rehabilitation protocols may have poorer outcomes.
Summary of Operative versus Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Displacement | Complete displacement (100%), significant translation | Minimally displaced (<100%), stable |
| Shortening | > 15-20 mm shortening | Minimal shortening (<15 mm) |
| Comminution | Significant comminution (e.g., Z-fragment) | Simple, transverse, or oblique patterns without major comminution |
| Soft Tissue | Open fracture, impending skin tenting, neurovascular compromise | Closed fracture, intact skin, no neurovascular compromise |
| Associated Injuries | Floating shoulder, multiple trauma | Isolated injury |
| Failure of Non-Op Tx | Symptomatic malunion or nonunion | Acute injury with no prior treatment attempt |
| Specific Scenarios | Pathologic fracture, professional athlete considerations (relative) | Low demand patient, good bone quality, minimal deformity |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical to optimize surgical outcomes, minimize complications, and ensure patient safety. This phase encompasses detailed imaging review, implant selection, and meticulous patient positioning.
Preoperative Imaging Assessment
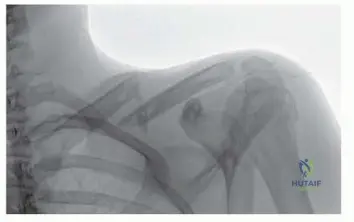
Standard radiographic evaluation typically includes an anterior-posterior (AP) view of the shoulder, a 45-degree cephalic tilt view (often called the Serendipity view or specific clavicle view), and a 45-degree caudal tilt view. These projections help characterize the fracture pattern, displacement, comminution, and any associated injuries to the glenohumeral or acromioclavicular joints.
For complex fracture patterns, significant comminution, or when considering revisions, a computed tomography (CT) scan is invaluable. A CT scan with 3D reconstructions provides superior detail regarding fracture morphology, bone loss, true shortening, and the spatial relationship of fragments, aiding in precise plate contouring and screw trajectory planning. Magnetic resonance imaging (MRI) is rarely indicated unless there is concern for associated soft tissue injury not apparent on radiographs or CT.
Implant Selection
The primary implant for clavicle fixation is a pre-contoured locking compression plate (LCP). These plates are designed to match the S-shape of the clavicle, minimizing the need for intraoperative bending and reducing the risk of plate fatigue. They come in various lengths and configurations (e.g., superior, anteroinferior, hook plates for lateral fractures). The choice between a superior or anteroinferior plating approach is often dictated by fracture location and surgeon preference, with some studies suggesting biomechanical advantages or lower hardware prominence rates with anteroinferior placement. However, superior plating is generally considered more robust biomechanically for midshaft fractures.
Plate length should be sufficient to accommodate at least three bicortical screws on each side of the fracture, ideally involving 6-8 cortices per main fragment, ensuring adequate fixation strength. Locking screws are generally preferred in osteopenic bone or when there is significant comminution, as they provide angular stability independent of plate-to-bone compression. Non-locking screws can be used for compression or in areas of good bone quality.
Patient Counseling and Consent
A detailed discussion with the patient regarding the risks, benefits, and alternatives of operative fixation is essential. Key points to cover include:
* Potential for nonunion or malunion with non-operative treatment.
* Risks of surgery: infection, hardware prominence, nerve injury (supraclavicular), neurovascular injury, nonunion, malunion, refracture, need for hardware removal.
* Expected rehabilitation protocol and recovery timeline.
* Realistic expectations regarding pain relief and functional return.
Preoperative Preparation and Patient Positioning
Antibiotic prophylaxis, typically a first- or second-generation cephalosporin, should be administered within 60 minutes prior to incision.
Patient positioning is critical for optimal surgical exposure and access. The patient is typically positioned in a beach chair position or supine position with a bolster placed longitudinally between the scapulae. This retracts the shoulders posteriorly, allowing the clavicle to fall back into a more anatomical position, elevating the fracture fragments anteriorly and making them more accessible.
- Beach Chair Position: Offers excellent visualization of the superior aspect of the clavicle and facilitates access to the neck and upper extremity. The head should be extended and rotated slightly away from the operative side to improve exposure of the medial clavicle.
- Supine Position: With a bolster, also provides good exposure. The ipsilateral arm should be draped free on an arm board or surgical table, allowing for manipulation of the upper extremity during reduction maneuvers.
Careful padding of all pressure points is essential. The entire ipsilateral upper extremity, shoulder, and neck are prepped and draped in a sterile fashion, ensuring adequate working space for both the surgeon and assistant. Image intensification (fluoroscopy) should be readily available and draped sterilely.
Detailed Surgical Approach and Technique
The surgical approach to the clavicle requires meticulous technique to ensure adequate exposure, anatomical reduction, stable fixation, and minimize iatrogenic injury to critical neurovascular structures.
Incision Design and Initial Dissection
A standard incision for midshaft clavicle fractures is a transverse or slightly oblique incision centered over the fracture site. This incision should ideally follow Langer's lines to optimize aesthetic outcomes. The length of the incision should be sufficient to allow adequate exposure of both fracture fragments for reduction and plate application, typically 6-10 cm. Some surgeons prefer a slightly superior curvilinear incision, particularly for superior plate placement, to avoid scarring directly over the plate.
After the skin incision, dissection proceeds through the subcutaneous tissue. The superficial fascia is carefully incised. At this stage, it is paramount to identify and protect the supraclavicular nerves. These nerves typically cross the clavicle obliquely, often several centimeters lateral to the sternoclavicular joint and superficial to the platysma muscle. They can be found within the superficial fat layer. Gently sweeping these nerves superiorly or inferiorly with blunt dissection, or sharply dissecting them free and tagging them with a vessel loop, is essential to prevent injury, which can lead to persistent dysesthesia or numbness.
Platysma Management and Subperiosteal Exposure
The platysma muscle lies immediately deep to the supraclavicular nerves. It should be sharply incised along the line of the skin incision. Meticulous electrocautery should be used to achieve hemostasis. After the platysma, a thin layer of deep fascia is encountered. Careful, sharp dissection through this fascia directly exposes the superior aspect of the clavicle.
Subperiosteal dissection should be minimized to preserve the blood supply to the fracture fragments. The periosteum is incised longitudinally along the superior cortex of the clavicle over the fracture site. A small periosteal elevator can be used to carefully elevate the periosteum only enough to expose the fracture ends and allow for plate application. Excessive stripping can devitalize fragments, especially in comminuted patterns, and increase the risk of nonunion.
Fracture Reduction
Anatomical reduction is the cornerstone of successful clavicle fixation. The typical displacement pattern involves superior migration of the medial fragment due to sternocleidomastoid pull, and inferior/medial/anterior displacement of the lateral fragment due to the weight of the arm and pull of the deltoid and pectoralis major.
- Reduction Maneuvers:
- Manual Traction: An assistant can apply longitudinal traction to the arm, gently abducting and extending the shoulder to relax surrounding musculature and help align the fragments.
- "Joy Sticks": Small K-wires or bone clamps can be inserted into the main fracture fragments to serve as levers, allowing the surgeon to manipulate them into reduction. This is particularly useful for controlling rotation and correcting superior/inferior displacement.
- Reduction Forceps: Pointed reduction forceps (e.g., Verbrugge, mini-fragment) are used to grasp the main fragments and compress them together, correcting shortening and ensuring cortical apposition. Care must be taken to avoid soft tissue entrapment.
- Temporary K-wires: Once reduced, temporary K-wires can be used to maintain the reduction while the plate is positioned and secured. These should be placed carefully to avoid obstructing future screw paths.
The goal is to restore the original length, angulation, and rotation of the clavicle. Fluoroscopy is helpful to confirm adequate reduction in both AP and cephalic tilt views.

Plate Application and Screw Fixation
Once the fracture is anatomically reduced and held securely, the appropriately sized and contoured plate is selected.
- Plate Placement: For midshaft fractures, superior plating is common due to the broad superior surface providing ample bone stock. Anteroinferior plating is an alternative, potentially reducing hardware prominence and offering a biomechanically favorable tension-band effect, but requires more meticulous dissection and has a higher risk of neurovascular injury. Pre-contoured plates significantly simplify this step. If manual contouring is necessary, it should be performed carefully to match the S-shape of the clavicle, ensuring the plate lies flush with the bone to minimize stress risers and hardware prominence.
- Initial Fixation: The plate is centered over the fracture site, ensuring adequate length for at least three screws (ideally 6 cortices) on each side of the fracture. A clamp can be used to hold the plate securely to the bone.
- Compression (if applicable): If a non-locking plate is used or if a locking plate has a lag screw slot, eccentric drilling of the first screw hole in the "load" position on one side of the fracture can achieve interfragmentary compression. A lag screw can also be placed through the plate or separately to compress oblique fracture patterns.
- Neutralization: The plate then neutralizes the forces acting on the fracture, protecting any lag screws or compression achieved.
- Screw Insertion:
- Drilling: Using appropriate drill guides, bicortical screw holes are drilled. Accurate drill depth measurement is crucial.
- Screw Type: Locking screws provide angular stability and are particularly useful in comminuted fractures or osteoporotic bone. Non-locking cortical screws can be used for compression or in areas of good bone quality.
- Screw Length: Screws should be bicortical, but care must be taken to avoid overt penetration of the inferior cortex, particularly medially and laterally, to prevent iatrogenic injury to the subclavian vessels, brachial plexus, or pleura. Fluoroscopy (lateral view or careful oblique views) can be invaluable to confirm screw length, especially for the medial screws.
- Number of Screws: A minimum of three bicortical screws on each side of the fracture is generally recommended. The goal is to maximize screw purchase without excessively stripping the periosteum.
- Final Assessment: After all screws are inserted, the reduction and fixation stability are reassessed clinically and fluoroscopically. The construct should be rigid, and the fracture should be anatomically aligned.

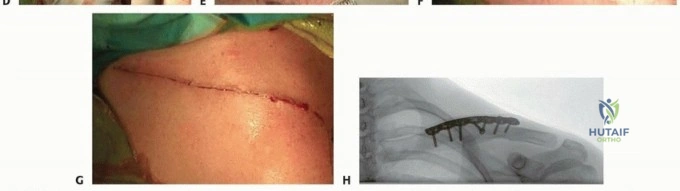
Wound Closure
Meticulous layered wound closure is essential to minimize complications such as infection, hematoma, and hardware prominence, while optimizing aesthetic outcome.
- Periosteum: If a significant periosteal flap was created, it can be loosely reapproximated with absorbable sutures, but direct closure over the plate should be avoided to prevent impingement.
- Platysma: The platysma muscle should be carefully repaired with absorbable sutures to reduce tension on the skin and improve cosmetic results. This also helps bury the hardware.
- Subcutaneous Layer: The subcutaneous tissue is closed with interrupted absorbable sutures to obliterate dead space and provide further skin support.
- Skin: The skin is closed with a subcuticular absorbable suture or staples/non-absorbable sutures, depending on surgeon preference. A sterile dressing is applied.

Complications and Management
Despite advancements in surgical technique and implant design, complications can still arise following clavicle plate fixation. Understanding their incidence and appropriate management strategies is crucial for academic orthopedic surgeons.
Common Complications
- Nonunion: The failure of bone healing within 6-9 months post-fixation, with no signs of progression. While operative fixation generally aims to reduce nonunion rates compared to displaced non-operative fractures, it can still occur (reported incidence 2-6%). Risk factors include severe comminution, infection, poor bone quality, inadequate fixation, and smoking.
- Management: Symptomatic nonunions typically require revision surgery, including hardware removal, debridement of fibrous tissue, refresh of fracture ends, bone grafting (autograft or allograft), and re-fixation with a more stable construct.
- Symptomatic Malunion: Healing of the fracture in an anatomically unacceptable position, leading to pain, functional limitation (e.g., impingement, rotator cuff dysfunction), cosmetic deformity, or neurovascular symptoms (e.g., thoracic outlet syndrome). Incidence varies but is higher with non-operative management of significantly displaced fractures.
- Management: Symptomatic malunions may require corrective osteotomy, wedge resection, and internal fixation to restore length and alignment.
- Hardware Prominence/Irritation: Due to the subcutaneous nature of the clavicle, the plate and screws can be palpable and cause irritation, especially with activities or clothing. This is one of the most common reasons for secondary surgery (up to 30-50% in some series).
- Management: Symptomatic hardware typically necessitates elective hardware removal once the fracture has demonstrably healed, usually 12-18 months post-operatively.
- Infection: Superficial or deep surgical site infection, with reported rates ranging from 1-5%.
- Management: Superficial infections may respond to oral antibiotics. Deep infections require surgical debridement, intravenous antibiotics, and potentially hardware removal if the infection persists or if the fracture is healed.
- Nerve Injury:
- Supraclavicular Nerve Injury: The most common neurological complication (incidence 10-20% or higher). Causes localized numbness, hyperesthesia, or dysesthesia over the anterosuperior chest wall. Often transient but can be persistent.
- Brachial Plexus/Subclavian Neurovascular Injury: Rare but catastrophic, usually due to inadvertent deep drilling or screw penetration.
- Management: Supraclavicular nerve symptoms are often managed conservatively with reassurance. Persistent, severe dysesthesia may warrant pain management consultation, nerve blocks, or rarely, surgical neurolysis or neurectomy. Brachial plexus or vascular injury requires immediate surgical exploration and repair.
- Pneumothorax: Extremely rare, caused by medial screw penetration through the pleura.
- Management: Requires chest tube insertion and monitoring.
- Refracture: Fracture occurring after hardware removal or inadequate healing.
- Management: Usually requires revision surgery with re-fixation and potentially bone grafting.
- Frozen Shoulder/Shoulder Stiffness: Less common than with other shoulder surgeries, but can occur if aggressive early range of motion is not initiated.
- Management: Physical therapy, sometimes manipulation under anesthesia.
Table of Common Complications and Management
| Complication | Incidence (Approximate) | Clinical Presentation | Salvage/Management Strategy |
|---|---|---|---|
| Nonunion | 2-6% | Persistent pain, motion at fracture site, radiographic lucency | Revision ORIF with debridement, decortication, bone grafting (autograft/allograft), re-fixation with more stable construct. Address underlying risk factors (e.g., smoking cessation). |
| Symptomatic Malunion | Variable | Pain, shoulder impingement, functional deficit, cosmetic deformity | Corrective osteotomy (wedge/open), re-fixation, bone grafting if required. |
| Hardware Prominence/Irritation | 30-50% | Palpable hardware, local pain, skin irritation, discomfort with clothing | Elective hardware removal after fracture healing (typically 12-18 months post-op). |
| Surgical Site Infection | 1-5% | Redness, swelling, warmth, pain, purulent discharge, fever | Superficial: Oral antibiotics. Deep: Surgical irrigation and debridement, IV antibiotics; potentially hardware removal if infection persists or fracture is healed. |
| Supraclavicular Nerve Injury | 10-20%+ | Numbness, hyperesthesia, dysesthesia over chest wall | Conservative management (reassurance), pain management, nerve blocks. Rarely, surgical neurolysis/neurectomy for persistent, severe symptoms. |
| Brachial Plexus/Vascular Injury | <0.1% | Neurological deficit, pulselessness, expanding hematoma, hemorrhage | Immediate surgical exploration, neurovascular repair. |
| Pneumothorax | Rare (<0.1%) | Dyspnea, chest pain, diminished breath sounds | Chest tube insertion, close monitoring. |
| Refracture | 1-5% | Recurrence of pain and deformity at fracture site after initial healing/hardware removal | Revision ORIF, often with bone grafting, considering biomechanical factors and bone quality. |
| Shoulder Stiffness/Frozen Shoulder | 1-2% | Restricted active/passive range of motion | Aggressive physical therapy, pain management. May require manipulation under anesthesia or arthroscopic capsular release in refractory cases. |

Post Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is critical for maximizing functional recovery, ensuring union, and preventing complications following clavicle plate fixation. The approach typically emphasizes early protected range of motion, gradual strengthening, and progressive return to activity, tailored to individual patient healing capacity and fracture stability.
Immediate Postoperative Period 0-2 Weeks
- Immobilization: The arm is typically placed in a sling for comfort and to protect the surgical site. The sling is primarily for comfort and proprioceptive feedback rather than rigid immobilization.
- Pain Management: Opioid and non-opioid analgesics, nerve blocks, and ice are used to manage post-operative pain.
- Early Range of Motion (ROM):
- Elbow, Wrist, Hand: Immediate active ROM exercises are encouraged to prevent stiffness and promote circulation.
- Passive Shoulder ROM: Gentle passive shoulder flexion to 90 degrees and external rotation to 30 degrees, often performed with the aid of the uninvolved arm, is initiated within the first few days. Pendulum exercises can also be started to encourage gentle glenohumeral motion.
- Scapular Mobility: Gentle scapular retraction and protraction exercises.
- Wound Care: Daily dressing changes as per protocol. Monitoring for signs of infection.
Early Rehabilitation 2-6 Weeks
- Sling Use: Gradually wean from sling as comfort allows, typically for sleeping and in crowded environments.
- Active-Assisted ROM: Progress to active-assisted ROM for shoulder flexion, abduction, and rotation within pain-free limits. Avoid forced end-range motion.
- Isometrics: Begin gentle isometric exercises for shoulder musculature (deltoid, rotator cuff, scapular stabilizers) without resistance.
- Proprioception: Introduce light proprioceptive exercises.
- Weight Bearing: No weight bearing or lifting objects heavier than a coffee cup with the operative arm.
- Activities of Daily Living (ADLs): Encourage use of the arm for light ADLs, maintaining elbow, wrist, and hand strength.
Intermediate Rehabilitation 6-12 Weeks
- Radiographic Assessment: Obtain follow-up radiographs to assess for signs of union. Clinical union (lack of pain, tenderness, or motion at the fracture site) is often evident before complete radiographic bridging.
- Full Active ROM: Progress to full active, pain-free ROM for the shoulder.
- Light Strengthening: Initiate light progressive resistance exercises for all shoulder girdle muscles using elastic bands or very light weights. Focus on rotator cuff and scapular stabilization.
- Avoidance: Continue to avoid heavy lifting, pushing, pulling, or sudden, uncontrolled movements.
- Cardiovascular Activity: Low-impact cardiovascular activities (e.g., stationary cycling) can be increased.
Advanced Rehabilitation 12 Weeks to 6 Months
- Progressive Strengthening: Advance strengthening exercises with increased resistance and intensity. Incorporate functional exercises relevant to the patient's occupation or sport.
- Plyometrics and Agility: For athletes, introduce sport-specific drills, plyometrics, and agility training as appropriate.
- Impact Activities: Gradual return to activities that involve impact or risk of re-injury.
- Return to Sport/Work: A gradual return to unrestricted activities, including contact sports or heavy labor, is permitted once radiographic union is confirmed, full strength is regained, and the patient is pain-free. This typically occurs at 4-6 months, but can vary. Protection against direct blows to the shoulder should be emphasized for athletes.
Long-Term Considerations
- Hardware Removal: Elective hardware removal may be considered 12-18 months post-operatively if hardware prominence or irritation persists and the fracture is fully healed. This should only be performed once union is robust to minimize the risk of refracture.
- Ongoing Monitoring: Continue to monitor for any signs of residual pain, weakness, or functional limitation.
This protocol serves as a general guideline and should always be individualized based on the patient's specific fracture pattern, bone quality, associated injuries, surgical stability achieved, and rehabilitation progress. Close collaboration between the surgeon and physical therapist is essential.
Summary of Key Literature and Guidelines
The literature surrounding clavicle fracture management has evolved significantly over the past two decades, with a growing consensus favoring operative fixation for certain displaced fracture patterns. This shift is largely driven by high-level evidence demonstrating improved outcomes compared to non-operative treatment in specific cohorts.
Landmark Studies and Evidence Base
The Canadian Orthopaedic Trauma Society (COTS) study (2007) was a pivotal randomized controlled trial that directly compared operative (plate fixation) versus non-operative management for displaced midshaft clavicle fractures. This study demonstrated significantly improved functional outcomes (DASH scores) and lower rates of symptomatic malunion and nonunion in the operatively treated group at 1 year. The COTS study provided robust evidence challenging the long-held dogma of universal non-operative management for these injuries.
Subsequent meta-analyses and systematic reviews have largely corroborated these findings, reinforcing the benefit of operative fixation for significantly displaced midshaft clavicle fractures, defined as >100% displacement, >15-20 mm shortening, or significant comminution. While absolute indications for surgery remain somewhat debated, the trend towards earlier operative intervention for unstable patterns is clear.
Plate Design and Biomechanics
Research into plate design has led to the widespread adoption of pre-contoured locking plates. Biomechanical studies have shown superior stiffness and strength of locking plate constructs compared to conventional non-locking plates, particularly in comminuted fractures or osteoporotic bone. The choice between superior versus anteroinferior plating continues to be an area of discussion. While superior plating offers a wider surface area for screw purchase and is generally considered more straightforward, some biomechanical studies suggest that anteroinferior plating may provide a more favorable tension-band effect. However, the proximity to the neurovascular bundle makes the anteroinferior approach technically more demanding with a potentially higher risk of neurovascular injury if not performed meticulously. Overall, current evidence does not definitively favor one approach over the other in terms of clinical outcome, with surgeon experience and fracture pattern often guiding the choice.
Hardware Removal
The high rate of hardware prominence and subsequent removal is a well-documented concern. Studies suggest that up to 50% of patients may elect for hardware removal. While elective, the need for a second surgical procedure is a significant consideration in patient counseling. Research continues to explore thinner, lower-profile plates or alternative biodegradable fixation options to mitigate this issue, though these are not yet standard of care.
Rehabilitation Paradigms
Contemporary rehabilitation protocols emphasize early, protected range of motion to prevent stiffness and promote early functional recovery. This approach, supported by numerous studies, contrasts with historical prolonged immobilization and is integral to the overall success of operative management. Return to sport or full activity is typically dictated by radiographic union and functional recovery, often between 4-6 months post-surgery.
Future Directions
Ongoing research areas include:
* Optimization of minimally invasive techniques for plate insertion.
* Development of advanced biological augmentation strategies to enhance fracture healing.
* Further refinement of patient-specific indications and outcomes prediction models.
* Long-term functional outcomes comparing operative and non-operative groups, especially concerning rates of post-traumatic arthritis.
In conclusion, the current academic consensus, informed by robust clinical trials and biomechanical studies, supports operative fixation for significantly displaced and comminuted midshaft clavicle fractures to improve union rates, reduce symptomatic malunion, and enhance functional outcomes. Meticulous surgical technique, appropriate implant selection, and a structured rehabilitation protocol are paramount to achieving these favorable results.

Clinical & Radiographic Imaging


