Surgical Management of Midshaft Clavicle Malunions: Osteotomy and Plate Fixation

Key Takeaway
Midshaft clavicular malunions often present with significant shortening, pain, and altered shoulder biomechanics. Surgical correction via corrective osteotomy and rigid plate fixation restores anatomical length and rotation. This comprehensive guide details the preoperative planning, beach-chair positioning, precise osteotomy execution, and dynamic compression plating required to achieve optimal functional outcomes and reliable osseous union in symptomatic patients.
Comprehensive Introduction and Patho-Epidemiology
Historically, fractures of the clavicular midshaft were managed almost exclusively via nonoperative modalities, relying on the robust osteogenic potential of the clavicle and the expectation of high union rates. Early literature, heavily influenced by Neer’s seminal reviews, suggested that nonunion was exceptionally rare and functional outcomes were universally acceptable, regardless of the final anatomical alignment. However, contemporary orthopedic literature, propelled by advanced biomechanical analyses and rigorous patient-reported outcome measures (PROMs), has definitively overturned this historical dogma. It is now well-established that significant displacement and shortening of the clavicle—typically defined as greater than 1.5 to 2.0 centimeters—can lead to a highly symptomatic malunion, profoundly altering the resting position and kinematic function of the entire shoulder girdle.
A malunited clavicle is classically characterized by a complex, multiplanar deformity: absolute shortening of the osseous strut, inferior displacement of the distal fragment due to the weight of the appendicular skeleton, and anterior rotation driven by the unopposed pull of the pectoralis major. This architectural distortion inevitably medializes the center of rotation of the glenohumeral joint and alters the resting tension of the periscapular musculature. Consequently, patients frequently present with a constellation of debilitating symptoms, including chronic periscapular pain, rapid fatigability during sustained activities, objective weakness in overhead elevation, and pronounced scapular dyskinesia. In severe cases, the hypertrophic callus and the depressed orientation of the malunion can encroach upon the costoclavicular space, precipitating secondary thoracic outlet syndrome (TOS) due to dynamic compression of the brachial plexus and subclavian vessels.

Epidemiologically, clavicle fractures account for approximately 2.6% to 4% of all adult fractures, with midshaft diaphyseal lesions representing nearly 80% of these injuries. While the overall nonunion rate remains relatively low, the incidence of symptomatic malunion in displaced, nonoperatively treated midshaft fractures is increasingly recognized as a significant clinical entity. Studies indicate that up to 15% to 20% of patients with initial shortening greater than 2 centimeters will develop a functionally limiting malunion if managed conservatively. The recognition of these poor outcomes has driven a paradigm shift toward early primary osteosynthesis for severely displaced acute fractures; however, the orthopedic surgeon must remain adept at managing the established malunion.
Surgical intervention via corrective osteotomy and rigid plate fixation is definitively indicated for patients with symptomatic malunions who have failed a comprehensive course of conservative management, including targeted periscapular rehabilitation. The primary, non-negotiable goals of operative management are the precise restoration of anatomical length, the meticulous correction of the rotational deformity, and the establishment of absolute mechanical stability to facilitate primary bone healing. By re-establishing the clavicle as a rigid strut, the surgeon restores the anatomical tension of the shoulder girdle, thereby resolving scapular dyskinesia, alleviating neurovascular tethering, and optimizing the biomechanical efficiency of the rotator cuff and deltoid musculature.
Detailed Surgical Anatomy and Biomechanics
Osteology and Muscular Deforming Forces
The clavicle is a unique, S-shaped long bone that serves as the sole osseous link between the axial skeleton and the appendicular upper extremity. Anatomically, it transitions from a robust, tubular cross-section in its medial two-thirds—which is convex anteriorly—to a flattened, broad cross-section in its lateral one-third, which is concave anteriorly. This transitional zone at the midshaft is inherently devoid of robust muscular or ligamentous attachments, making it the biomechanical weak point and the most frequent site of fracture and subsequent malunion. Understanding this complex three-dimensional morphology is critical for the orthopedic surgeon, as any corrective osteotomy must not only restore linear length but also recreate this specific S-shaped contour to avoid iatrogenic neurovascular compression or cosmetically unacceptable hardware prominence.
The displacement patterns observed in midshaft clavicle malunions are dictated entirely by the powerful, unopposed muscular forces acting upon the disjointed fragments. The proximal (medial) fragment is invariably drawn superiorly and posteriorly by the robust insertion of the sternocleidomastoid (SCM) muscle. Conversely, the distal (lateral) fragment is subjected to multiple deforming vectors: the sheer weight of the arm pulls it inferiorly, while the pectoralis major and latissimus dorsi exert a strong medializing and anteriorly rotating force. This combination results in the classic bayonet apposition and overriding of fragments, leading to the pathognomonic shortening and anterior rotational deformity seen in symptomatic malunions.
Neurovascular Proximity and the Costoclavicular Space
The surgical anatomy of the clavicle is inextricably linked to its perilous proximity to the vital neurovascular structures of the superior mediastinum and thoracic outlet. The subclavian artery, subclavian vein, and the trunks and cords of the brachial plexus traverse directly deep to the middle third of the clavicle, separated only by the thin interposition of the subclavius muscle and the clavipectoral fascia. In the setting of a malunion, hypertrophic callus formation and the inferior displacement of the distal fragment can significantly narrow the costoclavicular space. This anatomical distortion places the neurovascular bundle at immense risk during surgical dissection, drilling, and osteotomy, demanding meticulous surgical technique and a profound respect for the subclavicular anatomy.
Biomechanical Sequelae of Clavicular Shortening
Biomechanically, the clavicle functions as a critical strut that lateralizes the glenohumeral joint, optimizing the length-tension relationship of the shoulder musculature. When a malunion results in shortening exceeding 1.5 to 2.0 centimeters, the scapula inevitably protracted and anteriorly tilted. This medialization of the shoulder girdle decreases the resting tension of the trapezius and rhomboids, leading to secondary muscular fatigue and chronic periscapular pain. Furthermore, the altered scapular kinematics dramatically reduce the efficiency of the rotator cuff, manifesting as measurable weakness in abduction and external rotation. Corrective osteotomy directly addresses this biomechanical cascade by restoring the strut length, thereby re-lateralizing the scapula and normalizing the complex force couples required for unimpeded, pain-free overhead function.
Exhaustive Indications and Contraindications
The decision to proceed with a corrective osteotomy for a clavicular malunion requires a nuanced evaluation of the patient's functional deficits, radiographic parameters, and overall physiological status. The presence of a radiographic malunion alone, in the absence of clinical symptoms, is not an indication for surgical intervention.
Indications for Corrective Osteotomy
The primary indication for surgery is debilitating, chronic pain localized to the malunion site or the periscapular musculature that is refractory to a minimum of 3 to 6 months of targeted physical therapy. Objective weakness, particularly rapid fatigability during sustained overhead activities, is a strong indicator of biomechanical compromise due to clavicular shortening. Neurological symptoms, such as paresthesias, radicular pain, or objective motor deficits indicative of secondary thoracic outlet syndrome (TOS), represent a compelling indication for surgical decompression via deformity correction. Additionally, severe cosmetic deformity, while relatively subjective, can be a valid indication in patients experiencing significant psychological distress, provided they understand the risks of the procedure and the inevitability of a surgical scar.
Contraindications to Surgical Intervention
Absolute contraindications include the presence of active, untreated local or systemic infection, which precludes the implantation of internal fixation hardware. A severely compromised soft tissue envelope over the clavicle—whether due to previous radiation therapy, severe burns, or multiple prior surgical incisions—represents a profound risk for wound dehiscence and hardware exposure, rendering the procedure relatively or absolutely contraindicated depending on the reconstructive options available (e.g., rotational flaps). Furthermore, patients who are entirely asymptomatic despite significant radiographic deformity should be counseled against surgery, as the risks of intervention outweigh the nonexistent clinical benefit. High-risk surgical candidates with severe cardiopulmonary comorbidities should also be managed nonoperatively.
| Category | Specific Parameters | Clinical Rationale / Considerations |
|---|---|---|
| Absolute Indications | - Refractory pain with shortening > 2.0 cm - Secondary Thoracic Outlet Syndrome (TOS) - Severe scapular dyskinesia with objective weakness |
Restoration of the osseous strut is required to decompress the neurovascular bundle and normalize shoulder girdle kinematics. |
| Relative Indications | - Shortening between 1.5 cm and 2.0 cm - Cosmetic dissatisfaction - Moderate fatigability during heavy labor |
Requires careful shared decision-making. Symptoms must correlate directly with the biomechanical deficit. |
| Absolute Contraindications | - Active local or systemic infection - Asymptomatic radiographic malunion - Medically unfit for general anesthesia |
High risk of hardware infection or catastrophic perioperative complications without tangible clinical benefit. |
| Relative Contraindications | - Poor soft tissue envelope (e.g., prior radiation) - Active smoking / nicotine dependence - Non-compliant patient |
High risk of wound breakdown, hardware exposure, and nonunion. Nicotine cessation is strongly advised preoperatively. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Radiographic Assessment
Meticulous preoperative planning is the absolute cornerstone of a successful clavicular osteotomy. The surgeon must accurately quantify the degree of deformity to determine the surgical strategy, particularly regarding the necessity of structural bone grafting. Clinically, determine the exact amount of length to be gained by comparing the injured side to the contralateral, uninjured shoulder. This is measured precisely from the center of the sternoclavicular (SC) joint to the anterior edge of the acromioclavicular (AC) joint. Radiographically, a standard shoulder series is insufficient. Standardized bilateral anteroposterior (AP) views on a single cassette, along with 15-degree cephalic tilt and 30-degree caudal tilt views, are required to assess the superior-inferior and anterior-posterior translation.
A computed tomography (CT) scan with high-resolution 3D reconstructions is highly recommended, and arguably mandatory, to fully appreciate the complex, multiplanar nature of the malunion. The 3D reconstructions allow the surgeon to visualize the exact rotational component of the deformity, which is often underappreciated on plain radiographs. Furthermore, the CT scan helps delineate the extent of the medullary canal obliteration and the volume of hypertrophic callus that will need to be resected. If the clinical shortening is substantially greater than the radiographic shortening, it indicates absolute bone loss or severe remodeling. In these instances, a structural intercalary bone graft (typically a tricortical graft harvested from the anterior iliac crest) will be required to compensate for the defect and restore length without placing excessive tension on the neurovascular bundle.
Anesthesia and Patient Positioning
Optimal patient positioning is critical for adequate surgical exposure, intraoperative fluoroscopy, and potential bone graft harvesting. The procedure is performed under general endotracheal anesthesia. A preoperative interscalene regional block is highly recommended and routinely utilized for robust postoperative pain control; however, a meticulous baseline neurological examination must be documented prior to the block to differentiate preoperative TOS symptoms from postoperative complications.
Place the patient in a modified "beach chair" (semisitting) position at approximately 30 to 45 degrees of elevation. The head must be securely secured in a neutral position, avoiding excessive contralateral neck rotation which can place undue tension on the brachial plexus. A critical step in positioning is the placement of a small bump or rolled towel vertically behind the medial border of the involved scapula. This protracts the shoulder girdle, bringing the clavicle forward, opening the operative field, and naturally aiding in the restoration of length during the reduction phase. The involved upper extremity should be draped free to allow for dynamic traction, manipulation, and rotational adjustments during the osteotomy and reduction sequence. Finally, routinely prep and drape the contralateral or ipsilateral anterior iliac crest in the event that an intercalary structural autograft or cancellous bone graft is required.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Soft Tissue Dissection
The surgical approach must balance adequate, extensile exposure of the malunion with the absolute preservation of the soft tissue envelopes necessary for hardware coverage and biological healing. Make an oblique or slightly curvilinear incision along the superior surface of the clavicle, centered directly over the palpable malunion mass. The incision should follow Langer’s lines when possible to optimize cosmetic healing.

Raise the skin and subcutaneous tissue as a single, full-thickness flap. It is imperative to meticulously dissect through the subcutaneous fat to identify and, if possible, protect the intermediate and lateral branches of the supraclavicular nerve. Transection of these nerves can lead to frustrating postoperative numbness over the anterior chest wall or the formation of a painful, hypersensitive neuroma directly over the surgical incision. Identify the underlying myofascial layer, which is comprised of the trapezius fascia superiorly and the deltopectoral fascia inferiorly.
This myofascial layer must be incised directly over the superior aspect of the clavicle and raised as contiguous, robust flaps. Preservation of this tissue is non-negotiable. It is required to achieve a secure, two-layered, watertight closure over the plate at the conclusion of the procedure. Excessive stripping or thermal damage to this layer can lead to catastrophic hardware prominence, wound dehiscence, and deep infection.
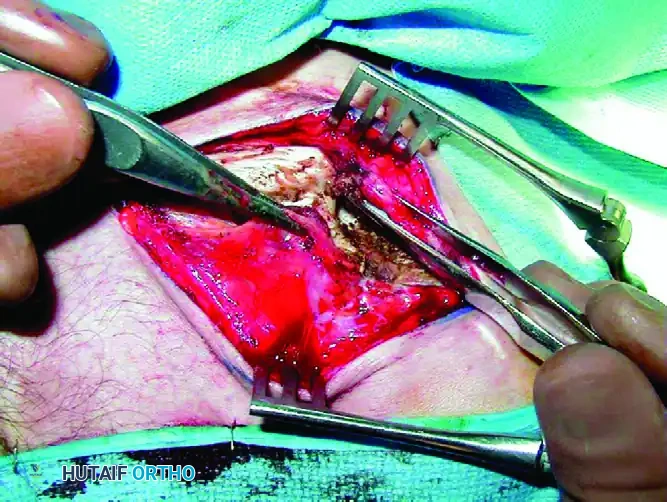
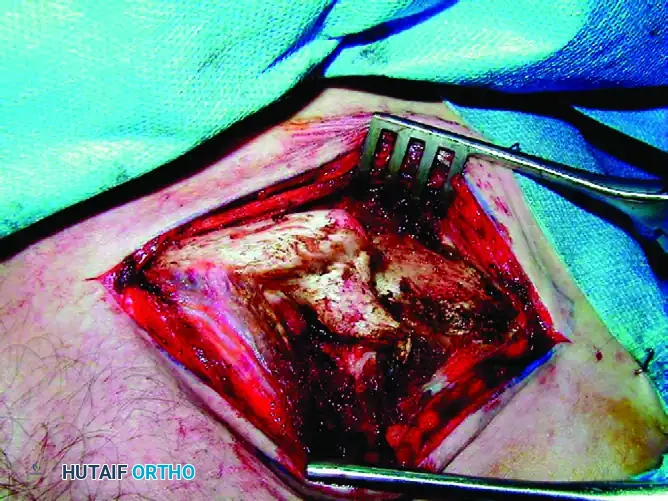
Identifying the Malunion and Executing the Osteotomy
Carefully expose the malunion site using sharp dissection and electrocautery. Maintain subperiosteal dissection strictly to the areas requiring plate application and osteotomy to preserve the periosteal blood supply. In most patients, the original proximal and distal fragments can still be delineated despite exuberant callus formation. The proximal fragment is typically elevated, while the distal fragment is depressed and rotated anteriorly.
Plan the corrective osteotomy carefully. If the malunion is extensively remodeled, an oblique sliding osteotomy may be necessary to maximize the surface area for healing while allowing for length restoration. Before completing the osteotomy, make a small, transverse notch with the saw in both the proximal and distal fragments outside the planned resection zone. This provides a fixed, objective reference point to accurately measure the degree of lengthening achieved after reduction. Utilize a combination of sharp, narrow osteotomes and a microsagittal saw to meticulously re-create the original fracture line or create the planned osteotomy plane.
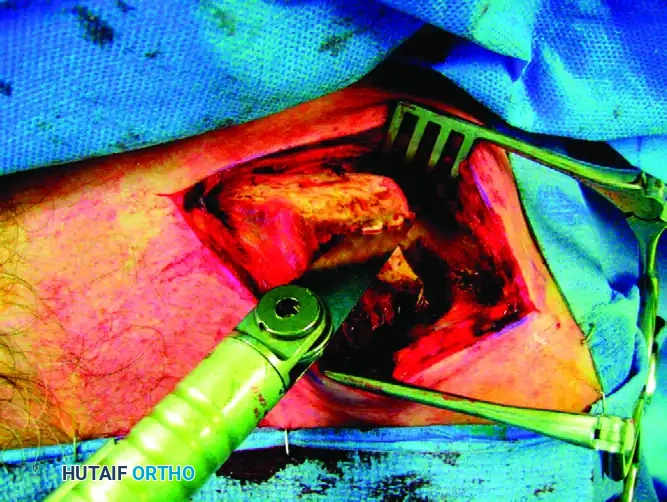
The microsagittal saw must be cooled continually with chilled saline irrigation throughout the cutting process to prevent thermal necrosis of the bone, which is a primary iatrogenic cause of nonunion. Extreme caution must be exercised to avoid plunging the saw blade or osteotomes inferiorly. The subclavian vessels and brachial plexus lie directly deep to the middle third of the clavicle. Place a malleable retractor or a blunt Hohmann retractor carefully beneath the clavicle to protect these structures during the osteotomy. Make no attempt to routinely explore or decompress the brachial plexus unless specifically indicated by preoperative neurological deficits and planned in conjunction with a peripheral nerve specialist.
Deformity Correction and Medullary Preparation
Once the osteotomy is complete and the fragments are fully mobilized, the focus shifts to biological preparation and anatomical reduction. Malunited fragments often have sclerotic, completely obliterated medullary canals due to the chronic remodeling process. Reestablish the medullary canal in both the proximal and distal fragments using a 3.5-mm drill bit or a small curette. This step is vital for restoring endosteal blood flow and providing access for osteoprogenitor cells and marrow elements to reach the osteotomy site.

Hold the proximal and distal fragments with pointed reduction forceps. Apply sustained lateral traction to the arm (utilizing an unscrubbed assistant) to stretch the contracted soft tissues and restore anatomical length.

Correcting the rotational deformity is often the most challenging aspect of the procedure. The distal fragment is typically rotated anteriorly. To correct this malrotation, redirect the flat superior surface of the distal fragment superiorly, rotating it until it perfectly matches the corresponding superior surface of the proximal fragment. Maintain the reduction with minimal soft tissue stripping. Once anatomical length and rotation are achieved, temporarily fix the osteotomy site with a 2.0-mm Kirschner wire (K-wire) or independent lag screws if the osteotomy geometry permits.
Internal Fixation Strategy
Rigid internal fixation is required to counteract the complex, multiplanar deforming forces acting on the clavicle. Select a 3.5-mm Limited Contact Dynamic Compression Plate (LC-DCP) or a pre-contoured anatomical locking plate. The plate must be of sufficient length to allow for a minimum of three bicortical screws (six cortices) on each side of the osteotomy. Typically, a plate with a minimum of six holes (range, 6 to 10 holes) is required depending on the fracture geometry and bone quality.

If using a standard LC-DCP, it must be meticulously contoured using bending presses to match the complex S-shaped anatomy of the superior clavicle. The use of modern, pre-contoured anatomical clavicle plates significantly reduces operative time by eliminating the need for extensive intraoperative bending. Furthermore, their low-profile anatomical shape minimizes hardware prominence, particularly at the medial aspect. Apply the plate to the superior surface of the clavicle. Because the corrective osteotomy is typically transverse or short oblique, the plate should be applied in absolute compression mode.

Utilize eccentric drilling in the holes immediately adjacent to the osteotomy to generate dynamic axial compression across the osteotomy site. Ensure all screws are bicortical to maximize pull-out strength, taking extreme care not to plunge the drill bit dangerously deep into the neurovascular structures beneath the clavicle. Use a depth gauge meticulously, and consider using blunt-tipped screws for the inferior cortex.

Bone Grafting and Biological Augmentation
Even with perfect anatomical reduction and rigid compression, the osteotomy site benefits immensely from biological augmentation, particularly if there is any cortical comminution or minor bone loss following the resection of the sclerotic malunion edges. Smooth the bone ends with a rongeur and collect the resected callus and any local bone debris.
Pack this morselized autograft tightly around the osteotomy site to stimulate osteogenesis and provide an osteoconductive scaffold. If an intercalary gap exists due to absolute bone loss or the need for significant lengthening, the previously harvested iliac crest structural graft should be precisely contoured and slotted into the defect prior to final plate compression. This structural graft acts as a biological strut, preventing excessive tension on the plate while promoting rapid incorporation.
Wound Closure
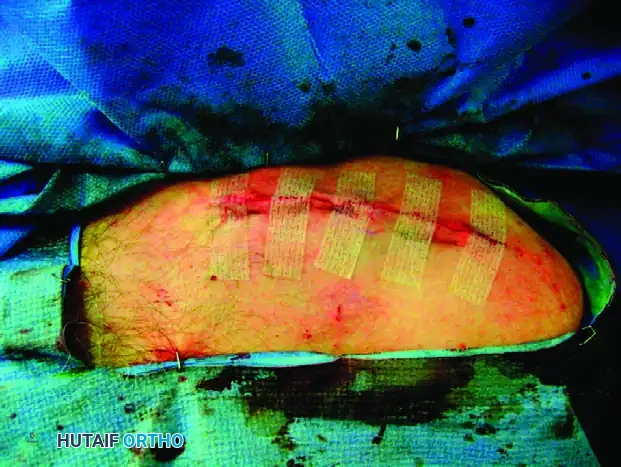
A meticulous, layered closure is critical to prevent hardware exposure and postoperative infection. First, close the contiguous flaps of the trapezius and deltopectoral fascia tightly over the plate using robust, No. 1 or 0 absorbable sutures (e.g., Vicryl). This myofascial layer provides the primary soft tissue coverage and biological barrier for the hardware. Next, approximate the subcutaneous fat and dermal layers using No. 2-0 absorbable sutures to reduce tension on the skin edges and eliminate dead space. Finally, close the skin with surgical clips or a running subcuticular stitch, depending on surgeon preference and skin quality. Apply a sterile, non-adherent dressing and place the patient's arm in a conventional shoulder sling before extubation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, corrective osteotomy of the clavicle carries a distinct complication profile. The surgeon must be prepared to identify and manage these adverse events promptly. The most frequent complication is hardware prominence and irritation, particularly in thin individuals or when standard straight plates are inadequately contoured. This often necessitates hardware removal after definitive osseous union is achieved (typically after 12 to 18 months).
Nonunion is a devastating complication, occurring in approximately 1% to 5% of cases. It is primarily driven by inadequate mechanical stability, excessive periosteal stripping leading to avascularity, or thermal necrosis from the saw blade. Management of a nonunion requires a robust salvage procedure: revision osteosynthesis, typically utilizing dual orthogonal plating (superior and anterior plates), combined with aggressive debridement of the nonunion site and application of a generous autologous iliac crest bone graft.
Neurovascular injuries are rare but catastrophic. Injury to the subclavian vessels can lead to life-threatening hemorrhage, requiring immediate vascular surgery intervention. Injury to the brachial plexus can result in permanent neurological deficits. Prevention through the meticulous use of protective retractors and controlled drilling techniques is paramount. Infection, while uncommon (2% to 4%), requires aggressive management with serial debridements, culture-specific intravenous antibiotics, and potentially hardware removal if the infection cannot be suppressed and the bone is united.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Hardware Irritation | 15% - 30% | Prominent plate profile, inadequate contouring, thin soft tissue envelope. | Hardware removal only after definitive radiographic and clinical union (minimum 12-18 months). |
| Nonunion | 1% - 5% | Thermal necrosis, inadequate compression, smoking, excessive periosteal stripping. | Revision osteosynthesis (dual plating), structural/cancellous autografting, strict smoking cessation. |
| Infection (Deep) | 2% - 4% | Poor soft tissue closure, hematoma formation, prolonged operative time. | Serial I&D, IV antibiotics. Retain hardware if stable until union; remove if loose or union achieved. |
| Neurovascular Injury | < 1% | Plunging drill bit, errant saw blade, aggressive inferior retraction. | Immediate vascular surgery consultation for hemorrhage. Nerve exploration for objective plexus injury. |
| Pneumothorax | < 1% | Errant drilling piercing the apical pleura. | Upright chest radiograph. Observation for small pneumothoraces; chest tube thoracostomy for large or symptomatic ones. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must delicately balance the need for early mobilization to prevent adhesive capsulitis (frozen shoulder) with the absolute necessity of protecting the osteotomy site from excessive torque and shear forces until early osseous union occurs. A standardized, phased approach ensures optimal functional recovery.
Phase I: Immediate Postoperative (0 to 2 Weeks)
During the initial healing phase, the primary goal is pain control and protection of the fixation. The patient's arm is maintained in a conventional sling at all times, except for hygiene and specific exercises. Pendulum exercises are initiated immediately postoperatively to maintain glenohumeral joint mobility and prevent capsular contracture. Active range of motion of the elbow, wrist, and hand is highly encouraged to promote venous return and prevent distal stiffness. The patient is strictly instructed to avoid any active shoulder elevation or lifting.
Phase II: Early Mobilization (2 to 4 Weeks)
At the 2-week postoperative mark, the surgical wound is inspected, and sutures or clips are removed. If the wound is healing well, active-assisted range of motion exercises for the shoulder are initiated. This includes supine wand exercises and pulley systems. Crucially, elevation is typically limited to 90 degrees in both the forward flexion and abduction planes. This limitation is necessary to prevent the powerful rotational forces exerted by the deltoid and trapezius from stressing the osteotomy site before soft callus formation has bridging strength.
Phase III: Active Motion (4 to 6 Weeks)
At 4 weeks postoperatively, standard AP and clavicle-specific radiographs (cephalic and caudal tilts) are obtained to assess the integrity of the hardware and look for early signs of osseous healing.


If the radiographs demonstrate
Clinical & Radiographic Imaging Archive


