Mastering Open Reduction and Internal Fixation of Clavicular Fractures
Key Takeaway
Open reduction and internal fixation (ORIF) of clavicular fractures is indicated for significantly displaced midshaft fractures to restore shoulder biomechanics and prevent nonunion. Surgical options include anteroinferior plating, superior plating, and intramedullary nailing. Successful outcomes depend on meticulous soft-tissue handling, preservation of the supraclavicular nerves, anatomic reduction, and rigid fixation. This guide details the step-by-step operative techniques, biomechanical considerations, and postoperative rehabilitation protocols for optimal patient recovery.
Comprehensive Introduction and Patho-Epidemiology
Clavicular fractures are ubiquitous within orthopedic trauma, representing approximately 5% to 10% of all adult fractures and encompassing nearly 44% of all injuries to the shoulder girdle. Epidemiologically, these fractures exhibit a distinct bimodal distribution. The primary peak occurs in young, active males (typically in the second and third decades of life) as a result of high-energy trauma, contact sports, or motor vehicle collisions. A secondary peak is observed in the elderly population, predominantly females, where low-energy falls onto the lateral aspect of the shoulder result in osteoporotic fractures. The vast majority of these injuries—up to 80%—occur in the middle third of the diaphysis, a region structurally predisposed to failure due to its lack of ligamentous support and its transitional cross-sectional morphology.
Historically, the management of midshaft clavicular fractures was heavily dictated by the conservative dogma established in the mid-20th century by pioneers such as Neer and Rowe. Nonoperative management, utilizing either a simple sling or a figure-of-eight harness, was considered the absolute gold standard for nearly all midshaft fractures, regardless of the degree of displacement. This approach was predicated on early retrospective studies that reported exceptionally low nonunion rates (less than 1%) and purportedly excellent functional outcomes. Consequently, generations of orthopedic surgeons were trained to accept significant clinical deformity and radiographic malunion as benign endpoints.
However, the dawn of evidence-based orthopedic traumatology and rigorous prospective research over the past two decades has precipitated a monumental paradigm shift. Landmark prospective randomized trials, most notably the multicenter studies conducted by the Canadian Orthopaedic Trauma Society (COTS), have unequivocally dismantled the historical consensus. These modern investigations have demonstrated that nonoperative treatment of completely displaced, shortened midshaft clavicle fractures results in nonunion rates approaching 15% to 20%. Furthermore, symptomatic malunion—characterized by chronic pain, rapid fatigability of the shoulder girdle, altered scapulothoracic kinematics (dyskinesia), and even thoracic outlet syndrome—has been recognized as a profound clinical entity in patients left to heal with significant shortening.
Consequently, Open Reduction and Internal Fixation (ORIF) is now firmly established as the standard of care for displaced midshaft clavicular fractures. The primary objectives of operative intervention are to meticulously restore the anatomic length and alignment of the shoulder girdle, provide rigid mechanical stability to facilitate immediate early mobilization, and minimize the risk of neurovascular compromise, nonunion, and long-term functional deficits. By restoring the native strut length of the clavicle, the surgeon re-establishes the optimal resting tension of the rotator cuff and periscapular musculature, thereby optimizing glenohumeral biomechanics.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of clavicular anatomy, its embryological origins, and the formidable deforming forces acting upon it is absolutely essential for successful surgical reconstruction. The clavicle is a complex, S-shaped tubular bone that acts as the sole osseous strut connecting the axial skeleton (via the sternoclavicular joint) to the appendicular skeleton of the upper extremity (via the acromioclavicular joint). Uniquely, it is the first bone in the human body to begin ossification (during the fifth week of fetal development) and the last to complete epiphyseal fusion (often extending into the late twenties). It ossifies primarily via intramembranous ossification, which contributes to its distinct healing characteristics and robust callus formation.
Osseous Morphology and Cross-Sectional Anatomy
The clavicle is not a uniform cylinder; its cross-sectional anatomy changes dramatically along its length, dictating both fracture patterns and implant application. The medial two-thirds of the clavicle are convex anteriorly and possess a robust, tubular cross-section that provides significant resistance to axial loading. In stark contrast, the lateral one-third is concave anteriorly and flattens out superior-inferiorly, becoming broad and relatively thin. The junction between these two distinct morphological zones—the middle third—represents a structural watershed area. It lacks the dense trabecular network of the extremities and is devoid of the muscular and ligamentous reinforcements found medially and laterally, making it highly susceptible to bending and torsional moments.
Muscular Deforming Forces
When a completely displaced midshaft fracture occurs, predictable and powerful deforming forces act upon the fragments, creating the classic radiographic and clinical presentation:
* Medial Fragment: The robust sternocleidomastoid (SCM) muscle inserts on the posterosuperior aspect of the medial clavicle. Upon fracture, the SCM exerts an unopposed, strong superior and posterior pull, elevating the medial fragment toward the base of the neck.
* Lateral Fragment: The weight of the upper extremity, acting through the coracoclavicular ligaments, draws the lateral fragment inferiorly. Concurrently, the powerful pull of the pectoralis major, latissimus dorsi, and subclavius muscles draws the lateral fragment anteriorly and medially. This combined vector results in the characteristic shortening, overlap, and ptosis (drooping) of the injured shoulder.
Neurovascular Proximity and Surgical Danger Zones
The surgical anatomy of the clavicle is defined by its perilous proximity to the vital structures of the thoracic outlet. The subclavian vessels (artery and vein) and the trunks and cords of the brachial plexus lie directly posterior and inferior to the middle third of the clavicle, separated only by the thin subclavius muscle and the clavipectoral fascia.
The distance between the posterior cortex of the clavicle and the subclavian vein can be as little as 10 to 15 millimeters. Furthermore, the dome of the pleura extends above the first rib, placing the patient at risk for iatrogenic pneumothorax. During surgical fixation, particularly when drilling from superior to inferior or placing excessively long screws, the risk of catastrophic neurovascular injury or pleural breach is ever-present. The surgeon must maintain absolute spatial awareness, utilizing drill stops, protective retractors, and precise depth measurement at all times.
Exhaustive Indications and Contraindications
The decision to proceed with operative management of a clavicular fracture requires a nuanced synthesis of radiographic parameters, patient demographics, functional demands, and medical comorbidities. While the indications for ORIF have expanded, careful patient selection remains the cornerstone of successful outcomes.
| Category | Specific Criteria / Conditions | Clinical Rationale |
|---|---|---|
| Absolute Indications | Open fractures | Requires immediate debridement and stabilization to prevent deep osteomyelitis. |
| Neurovascular compromise | Progressive brachial plexopathy or vascular occlusion requires immediate exploration, vessel repair, and rigid skeletal stabilization. | |
| Severe skin tenting | Impending open fracture due to pressure necrosis of the overlying skin from a sharp, displaced spike (typically the medial fragment). | |
| Floating shoulder | Concomitant displaced ipsilateral fracture of the glenoid neck or scapular body. Fixing the clavicle restores the superior suspensory complex. | |
| Relative Indications | Displacement > 100% | Lack of cortical contact significantly increases the risk of atrophic nonunion. |
| Shortening > 1.5 to 2.0 cm | Predictor of symptomatic malunion, altered shoulder kinematics, and decreased peak abduction strength. | |
| Severe comminution (Z-type) | Indicates a high-energy injury with extensive periosteal stripping; prone to shortening and nonunion if treated conservatively. | |
| Polytrauma / Multiple injuries | Facilitates early mobilization, weight-bearing through the upper extremities (e.g., crutch use for lower extremity fractures), and pulmonary toilet. | |
| High-demand patients | Elite athletes or heavy manual laborers requiring rapid, predictable return to baseline functional status. | |
| Absolute Contraindications | Active surgical site infection | High risk of deep hardware infection; requires infection eradication prior to internal fixation. |
| Unacceptable operative risk | Severe cardiopulmonary comorbidities precluding general anesthesia or prolonged surgical positioning. | |
| Relative Contraindications | Undisplaced / Minimally displaced | Excellent prognosis with nonoperative management; surgery introduces unnecessary risks (infection, nerve injury). |
| Poor soft tissue envelope | Severe abrasions, burns, or prior radiation therapy over the surgical site increasing wound breakdown risk. | |
| Non-compliant patient | Severe cognitive impairment or substance abuse precluding adherence to postoperative rehabilitation restrictions. |
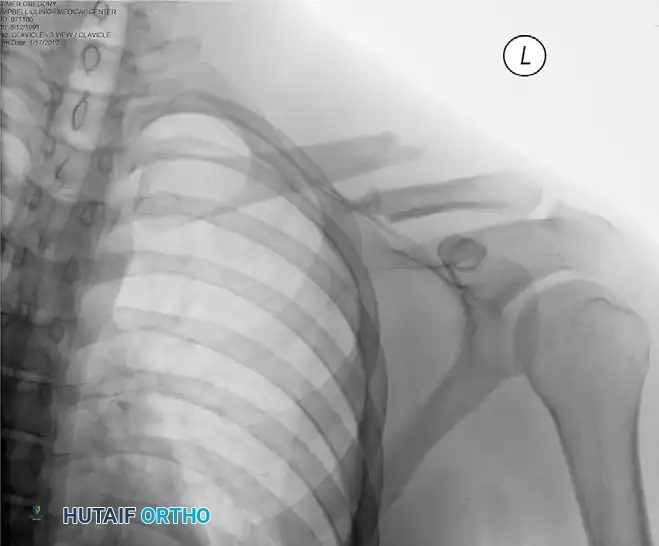
Preoperative radiograph demonstrating a significantly displaced midshaft clavicular fracture, an ideal candidate for surgical intervention due to complete loss of cortical contact and significant shortening.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the vanguard against intraoperative complications. The evaluation begins with obtaining high-quality, orthogonal radiographs. A standard anteroposterior (AP) view is insufficient due to the overlap of the thoracic ribs and the complex curvature of the clavicle. A 15- to 20-degree cephalad tilt view (the Zanca view) is mandatory; this projection projects the clavicle above the rib cage, providing an unobstructed assessment of fracture morphology, comminution, and superior-inferior displacement. In cases of significant comminution, medial intra-articular extension, or suspected nonunion, a 3D reconstructed computed tomography (CT) scan is invaluable for precise spatial mapping and implant templating.
Templating and Implant Selection
Digital templating allows the surgeon to anticipate the required plate length and configuration. The goal is to achieve adequate working length, aiming for a minimum of three (preferably four) bicortical locking or non-locking screws on each side of the fracture. The surgeon must predetermine whether an anteroinferior or superior plating strategy will be employed, as this dictates the type of pre-contoured locking compression plate (LCP) or reconstruction plate to be utilized.
Patient Positioning and Anesthesia
Anesthesia typically consists of a general endotracheal anesthetic supplemented by an ultrasound-guided interscalene regional block. This multimodal approach provides profound intraoperative muscle relaxation (crucial for overcoming the SCM and pectoralis forces during reduction) and excellent postoperative analgesia.
- Table and Posture: The patient is positioned in a modified beach-chair (semi-Fowler) position at approximately 30 to 45 degrees of elevation on a radiolucent operating table. This position decreases venous pressure in the surgical field, reducing bleeding, and provides excellent access to the superior shoulder girdle. Alternatively, a supine position can be used, which simplifies fluoroscopic access.
- Scapular Retraction: A critical maneuver is the placement of a large bump or a vertically rolled towel directly between the scapulae, along the thoracic spine. This allows the bilateral shoulder girdles to fall posteriorly. This passive scapular retraction utilizes gravity to un-shrug the shoulders, passively restoring clavicular length and dramatically improving the anterior exposure of the bone.
- Head Positioning: The patient's head is carefully secured in a neutral or slightly extended position and rotated 30 to 45 degrees away from the operative side. This maximizes the surgical field and shifts the endotracheal tube and anesthesia equipment away from the sterile prep area.
- Draping: The entire forequarter must be prepped and draped free. The drape should extend from the sternal notch to the mid-humerus. Allowing free manipulation of the ipsilateral arm is essential, as the assistant can apply traction, abduction, and external rotation to the arm to dynamically assist with intraoperative fracture reduction.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the clavicle demands a profound respect for the delicate soft tissue envelope and the underlying neurovascular structures. The choice between anteroinferior plating, superior plating, and intramedullary fixation depends on the fracture morphology, the surgeon's expertise, and the patient's anatomy.
Step 1: Incision and Superficial Dissection
The incision should be meticulously planned. A transverse incision directly over the superior aspect of the clavicle is traditional but is associated with broader, hypertrophic scarring due to tension along Langer's lines. A slightly oblique or "bra-strap" incision, placed just inferior to the clavicle, often yields superior cosmesis.
* Sharply incise the skin and subcutaneous fat down to the platysma muscle.
* Hemostasis is achieved using electrocautery.
* The platysma is divided in line with the incision.
* Neurovascular Preservation: As the superficial fascia is breached, the surgeon must actively search for the descending branches of the supraclavicular nerve (C3-C4 roots). These nerves arborize into medial, intermediate, and lateral branches that cross the anterior aspect of the clavicle. Meticulous dissection and vessel loops should be used to mobilize and protect these branches. Transection leads to a numb patch over the anterior chest wall and carries a high risk of painful, debilitating neuroma formation.
Step 2: Deep Dissection and Fascial Release
- Identify the clavipectoral fascia, which envelopes the subclavius muscle and attaches to the anterior-inferior border of the clavicle.
- Incise the fascia sharply. Elevate the soft tissues using a periosteal elevator.
- Direction of Dissection: Always begin deep dissection along the medial fragment. Because the medial fragment is elevated by the SCM, it is physically pulled away from the subclavian vessels and brachial plexus, making it the safer starting point. Once the medial fragment is controlled, dissection proceeds laterally.
- Biological Osteosynthesis: In acute, comminuted fractures, adhere strictly to the principles of biological osteosynthesis. Perform only minimal, targeted periosteal stripping necessary for plate footprint application. Butterfly fragments should not be stripped of their soft tissue attachments; preserving their vascularity is paramount for rapid osteogenesis and preventing atrophic nonunion.
Step 3: Fracture Reduction Techniques
- Utilize the pre-positioned scapular bump and have an assistant apply sustained, inline manual traction to the ipsilateral arm to overcome the shortening forces.
- Reduce the main fracture fragments anatomically. Pointed reduction forceps (Weber clamps) or Farabeuf clamps are applied to secure the reduction provisionally.
- Interfragmentary Compression: If the fracture exhibits a long oblique or spiral morphology, absolute stability should be achieved using a 3.5-mm or 2.7-mm cortical lag screw. The technique involves drilling a near-cortex glide hole, inserting a drill sleeve, drilling the far-cortex thread hole, countersinking the near cortex (to prevent stress risers), measuring, tapping (if non-self-tapping), and inserting the screw to compress the fracture plane. This converts complex shear forces into stabilizing compressive forces.
Step 4: Anteroinferior Plate Application
The anteroinferior plating technique, championed by Collinge and others, offers distinct biomechanical and clinical advantages.
* Biomechanical Advantage: Placing the plate on the anteroinferior surface allows the screws to be directed from anterior to posterior. This trajectory safely parallels the neurovascular bundle rather than aiming directly toward it. Furthermore, the anteroinferior cortex is often thicker, providing superior screw purchase.
* Contouring: Select a 3.5-mm pre-contoured locking plate or a standard reconstruction plate. The plate must be contoured with plate benders to match the complex S-shape of the clavicle perfectly.
* Application: Apply the plate to the bone. Drill the holes directing the bit slightly superiorly and posteriorly. This maximizes bone purchase and ensures that if a screw is slightly long, the sharp tip is directed into the muscular mass of the trapezius rather than down into the subclavian vein. Ensure at least three, but ideally four, bicortical screws are placed on either side of the fracture.
Step 5: Superior Plate Fixation Modifications
While anteroinferior plating is popular for safety and cosmetic reasons (less hardware prominence under the thin superior skin), superior plating remains mechanically robust. The superior aspect of the clavicle represents the tension band side of the bone. According to strict AO principles, a plate placed superiorly is mechanically optimal for resisting the inferior bending forces exerted by the weight of the arm.
* Technique: Pre-contoured superior locking plates are highly recommended to minimize intraoperative bending.
* Extreme Caution: When drilling from superior to inferior, the drill bit is aimed directly at the subclavian vessels, brachial plexus, and pleura. The surgeon must use a drill stop. A malleable ribbon retractor or a blunt Hohmann retractor should be carefully slipped under the clavicle to protect the underlying structures. Depth gauges must be read meticulously to prevent even 1-2 millimeters of over-penetration.
Step 6: Intramedullary Fixation (TENs)
Intramedullary (IM) nailing utilizing Titanium Elastic Nails (TENs) offers a minimally invasive alternative for simple, non-comminuted midshaft fractures (AO/OTA type 32-A or B).
* Rationale: IM nailing provides relative stability, preserving the fracture hematoma and encouraging robust secondary bone healing via endochondral ossification and callus formation.
* Technique: A small 1-2 cm incision is made over the medial end of the clavicle (sternal entry point). The anterior cortex is opened with an awl. A pre-bent titanium elastic nail (typically 2.0 to 3.0 mm in diameter) is manually advanced using a T-handle.
* Reduction: Closed reduction is performed using fluoroscopy and percutaneous reduction clamps. The nail is passed across the fracture site into the lateral fragment.
* Modifications for Safety: To prevent the historically high rates of hardware migration, an end cap must be applied to the medial end of the nail. The nail should never be power-driven, as this eliminates tactile feedback and risks cortical perforation.
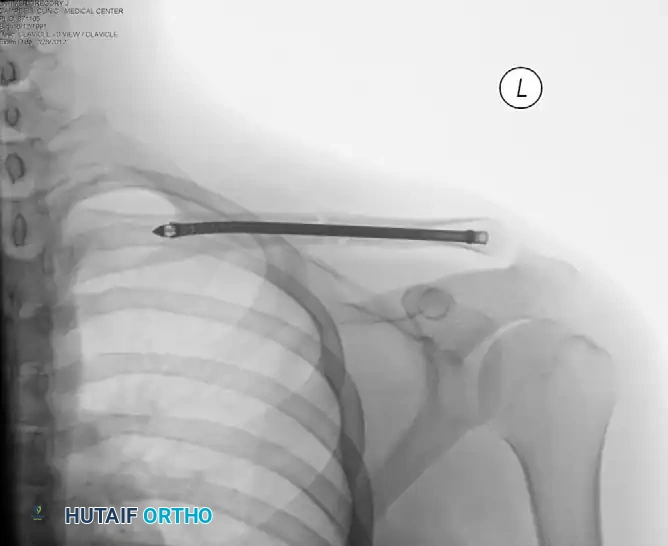
Postoperative radiograph demonstrating successful intramedullary fixation of the clavicle using a Titanium Elastic Nail, restoring anatomic length and alignment with minimal soft tissue disruption.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates of clavicular ORIF, complications do occur. The surgeon must be adept at recognizing and managing these issues promptly to prevent long-term morbidity.
| Complication | Estimated Incidence | Etiology and Pathophysiology | Salvage Management and Treatment |
|---|---|---|---|
| Hardware Prominence / Irritation | 15% - 30% | The superior clavicle has minimal subcutaneous fat. Plates can irritate skin, bra straps, or backpack straps. | Most common reason for reoperation. Hardware removal is performed only after solid radiographic union is confirmed (minimum 12-18 months post-op). |
| Infection (Superficial & Deep) | 2% - 5% | Poor soft tissue envelope, hematoma formation, or prolonged operative time. | Superficial: Oral antibiotics. Deep: Urgent surgical debridement, copious irrigation. If fixation is stable, retain hardware and use IV antibiotics. If loose, remove hardware, place antibiotic spacer, and plan for staged revision. |
| Nonunion | 1% - 3% | Inadequate mechanical stability, excessive periosteal stripping (atrophic), infection, or patient non-compliance (smoking). | Revision ORIF. Requires rigid dual plating or orthogonal plating, excision of the nonunion fibrous tissue, decortication, and application of autologous iliac crest bone graft (ICBG). |
| Supraclavicular Nerve Injury | 10% - 25% | Iatrogenic transection or excessive traction neuropraxia during superficial dissection. | Prevention is key. If transected, bury the proximal stump deep into muscle to prevent painful neuroma formation. Counsel patient on anterior chest numbness. |
| Implant Failure | 1% - 2% | Plate breakage or screw pullout due to early excessive loading prior to bony union, or utilizing an undersized plate. | Revision ORIF with a longer, more robust locking plate construct and potentially bone grafting if delayed union is present. |
| Neurovascular Injury | < 1% | Catastrophic plunge of drill bit or excessively long screws penetrating the subclavian vein/artery or brachial plexus. | Immediate vascular surgery consultation. Pack the wound, do not blindly clamp. May require median sternotomy or clavicle resection for vascular control. |
| Adhesive Capsulitis | 2% - 5% | Prolonged postoperative immobilization and failure to initiate early passive glenohumeral motion. | Aggressive physical therapy, intra-articular corticosteroid injections, or eventual arthroscopic capsular release if refractory. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional outcome following clavicular ORIF relies as much on a structured, phased postoperative rehabilitation program as it does on the surgical execution. The delicate balance involves preventing glenohumeral stiffness (adhesive capsulitis) while strictly protecting the mechanical fixation construct until clinical and radiographic union is achieved.
Phase 1: Immediate Postoperative Period (Weeks 0-2)
- Immobilization: The operated extremity is placed in a standard shoulder sling or a simple swath. This is primarily for comfort, to support the dependent weight of the arm, and to reduce the inferior traction forces on the newly applied hardware.
- Early Motion: Passive range of motion (ROM) is initiated immediately on postoperative day one. The patient is instructed in pendulum exercises (Codman exercises) to prevent capsular adhesions.
- Distal Joints: Active ROM of the elbow, wrist, and hand is highly encouraged and mandated multiple times a day to prevent distal dependent edema, stiffness, and complex regional pain syndrome (CRPS).
- Restrictions: Strict avoidance of any active shoulder elevation, abduction, heavy lifting, pushing, or pulling.
- Intramedullary Nailing Specifics: If the patient was treated with an IM device (TENs), the construct relies on relative stability. Therefore, postoperative range of motion must be strictly limited to a maximum of 90 degrees of forward flexion and abduction for the first 6 weeks to prevent catastrophic hardware back-out or medial migration.
Phase 2: Intermediate Phase (Weeks 2-6)
- Wound Check: Sutures are removed at 10 to 14 days.
- Weaning the Sling: The patient is gradually weaned from the sling. By week 4, the sling should only be utilized in crowded public spaces (for protection) or for comfort during sleep.
- Active-Assisted ROM: The physical therapy protocol advances from passive to active-assisted range of motion. Patients utilize overhead pulleys, wall-crawls, or a wand/cane to assist the operative arm using the contralateral healthy arm.
- Isometric Strengthening: Gentle, sub-maximal isometric strengthening of the deltoid, rotator cuff, and periscapular stabilizers can begin, provided it does not elicit pain at the fracture site.
Phase 3: Advanced Strengthening and Return to Play (Weeks 6-12+)
- Radiographic Check: At the 6- to 8-week mark, orthogonal radiographs must be obtained. The surgeon evaluates for bridging callus (expected in IM nailing) or the progressive obliteration of the fracture lines (expected in rigid plating).
- Active Strengthening: Once clinical signs (absence of point tenderness) and radiographic signs of healing are definitively present, progressive isotonic strengthening of the shoulder girdle is initiated. Resistance bands and light weights are introduced.
- Full Return: Full return to unrestricted activities, including heavy manual labor, overhead athletics, and contact sports, is generally permitted only when solid, mature fracture healing is confirmed both clinically and radiographically. This typically occurs between 10 to 14 weeks postoperatively. Premature return to contact sports is the leading cause of late catastrophic plate bending or refracture.
Summary of Landmark Literature and Clinical Guidelines
The evolution of clavicular fracture management is deeply rooted in high-quality, peer-reviewed literature. A comprehensive understanding of these landmark studies is mandatory for the academic orthopedic surgeon.
- The COTS Trial (Canadian Orthopaedic Trauma Society, 2007): This seminal multicenter prospective randomized controlled trial compared nonoperative management to ORIF with plate fixation for completely displaced midshaft clavicle fractures. The results were paradigm-shifting: the operative group demonstrated significantly lower rates of nonunion (2% vs. 15%), lower rates of symptomatic malunion, faster times to radiographic union, and significantly improved functional outcome scores (DASH and Constant scores) at all time points up to one year.
- Robinson et al. (2004): This expansive prospective cohort study defined the predictive factors for nonunion in conservatively managed fractures. Robinson identified that lack of cortical contact (complete displacement), shortening greater than 2 centimeters, and advanced age were the most significant independent risk factors for failing conservative management, laying the groundwork for modern surgical indications.
- Smekal et al. (2009): A prospective randomized trial comparing Titanium Elastic Nails (TENs) to nonoperative treatment. The study validated IM nailing as a superior alternative to slings for displaced fractures, citing faster functional recovery and lower nonunion rates,
