
Introduction and Epidemiology
Clavicle fractures represent a ubiquitous orthopedic injury, frequently encountered in both high-energy trauma settings and low-energy osteoporotic falls. Epidemiologically, these fractures account for approximately 2.6% to 5% of all adult fractures and encompass 44% to 66% of all fractures involving the shoulder girdle. The incidence demonstrates a classic bimodal distribution. The primary peak occurs in young, active males (typically in their second and third decades of life) secondary to high-energy trauma, sports injuries, or motor vehicle collisions. A secondary peak is observed in elderly females, predominantly associated with low-energy falls from a standing height compounded by decreased bone mineral density.
The mechanism of injury in the vast majority of cases (approximately 87%) involves a direct blow to the lateral aspect of the shoulder. This imparts a massive axial and bending load across the clavicle, leading to failure at its biomechanically weakest point. Less common mechanisms include a direct blow to the clavicle itself (7%) or an indirect force transmitted through a fall onto an outstretched hand (FOOSH) (6%). Furthermore, rare atraumatic etiologies such as violent muscle contractions during seizure activity, pathologic lesions, or stress fractures in overhead athletes must be considered in the absence of a distinct traumatic event.
Fracture location is highly predictable based on the bone's morphology. The middle third (diaphysis) is the site of 80% to 85% of all clavicle fractures. The lateral (distal) third accounts for 10% to 15%, while the medial (proximal) third is involved in fewer than 5% of cases. Classification systems, notably the Allman classification and the more prognostic Edinburgh (Robinson) classification, stratify these injuries based on anatomic location, displacement, and articular extension, directly guiding operative versus non-operative decision-making.
Surgical Anatomy and Biomechanics
A profound understanding of clavicular anatomy and its surrounding neurovascular structures is paramount for safe surgical intervention. The clavicle functions as a critical strut, suspending the upper extremity from the axial skeleton, thereby maximizing the functional range of motion of the glenohumeral joint while protecting the underlying neurovascular bundle.
Osteology and Development
The clavicle is a distinctively S-shaped long bone. Viewed superiorly, the medial two-thirds are convex anteriorly, while the lateral third is concave anteriorly. In cross-section, the medial aspect is robust and tubular, transitioning to a flattened, broad morphology laterally. Developmentally, the clavicle is unique. It is the first bone to initiate ossification in the human fetus (during the fifth week of gestation) via intramembranous ossification, distinct from the endochondral ossification typical of other long bones. Conversely, the medial clavicular epiphysis is the last physical growth plate to fuse, typically closing between 22 and 25 years of age. This delayed fusion is a critical diagnostic consideration, as medial clavicle "dislocations" in young adults are frequently physeal fractures (Salter-Harris types).
Muscular and Ligamentous Attachments
The clavicle serves as an anchor for several major muscle groups. Medially, the sternocleidomastoid originates from the superior surface, while the pectoralis major originates from the anterior surface. Laterally, the deltoid originates from the anterior border, and the trapezius inserts onto the posterior border. The subclavius muscle lies inferiorly, acting as a dynamic depressor and providing a crucial soft-tissue buffer between the clavicle and the underlying neurovascular structures.
Ligamentous stability is highly region-specific. Medially, the robust costoclavicular ligaments provide primary stability against superior displacement. Laterally, the coracoclavicular (CC) ligament complex is the primary suspensory mechanism of the upper extremity. The CC complex consists of the conoid ligament (medial and posterior, resisting superior and anterior translation) and the trapezoid ligament (lateral and anterior, resisting axial compression). Understanding the integrity of these ligaments is essential, particularly in distal third clavicle fractures (Neer Type II), where disruption leads to significant displacement and a high rate of nonunion if treated conservatively.
Neurovascular Proximity
The critical neurovascular bundle, comprising the subclavian artery, subclavian vein, and the cords of the brachial plexus, traverses directly posterior and inferior to the middle third of the clavicle. The distance between the posterior cortex of the clavicle and the subclavian vein can be as little as 10 to 15 millimeters. The clavipectoral fascia and the subclavius muscle afford the only anatomic protection during drilling and screw placement.
Indications and Contraindications
The paradigm for managing clavicle fractures has evolved significantly over the past two decades. Historically treated almost exclusively with non-operative modalities, modern evidence has delineated specific criteria where surgical fixation yields superior functional outcomes and lower nonunion rates.
Operative vs Non Operative Management
| Parameter | Operative Management | Non-Operative Management |
|---|---|---|
| Absolute Indications | Open fractures, skin tenting with impending necrosis, subclavian neurovascular compromise, floating shoulder (ipsilateral displaced scapular neck fracture). | Undisplaced or minimally displaced midshaft fractures, pediatric fractures (prior to physeal closure), high surgical risk patients. |
| Relative Indications | Shortening > 1.5 to 2.0 cm, displacement > 100% (no cortical contact), severe comminution (Z-deformity), polytrauma requiring early mobilization, bilateral clavicle fractures, high-demand athletes. | Displaced fractures in patients with low functional demands, non-ambulatory patients, patients refusing surgery. |
| Expected Nonunion Rate | 1% to 5% | 15% to 20% (in completely displaced midshaft fractures) |
| Primary Complications | Hardware prominence, incisional numbness, infection, adhesive capsulitis. | Malunion (shortening/ptosis), nonunion, prolonged immobilization, cosmetic bump. |
Contraindications to Surgery
Absolute contraindications to operative fixation include active infection over the surgical site, severe medical comorbidities precluding general anesthesia, and an inadequate soft tissue envelope (e.g., severe burns or massive abrasions over the clavicle). Relative contraindications include profound osteopenia or osteoporosis where hardware purchase is questionable, though modern locked plating techniques have mitigated this risk.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the foundation of successful clavicle osteosynthesis. Standard radiographic evaluation must include an anteroposterior (AP) view of the clavicle, a 15 to 20 degree cephalad tilt view (Zanca view) to evaluate superior-inferior displacement without thoracic superimposition, and an apical oblique view. In cases of significant comminution, suspected articular involvement (AC or SC joints), or delayed presentation evaluating for nonunion, a computed tomography (CT) scan with 3D reconstructions is highly recommended to assess fragment morphology and bone stock.
Patient Positioning Setup
The patient is typically positioned in a modified beach chair position or supine with a bump placed between the scapulae to allow the shoulder girdle to fall posteriorly. This maneuver aids in restoring the anatomic length of the clavicle by utilizing gravity to reduce the laterally displaced fragment.
The head is secured in a neutral position, slightly rotated away from the operative side to maximize exposure of the supraclavicular fossa. The entire upper extremity must be prepped and draped free to allow for intraoperative manipulation. The sterile field should extend from the mandible superiorly to the nipple line inferiorly, and across the midline to the contralateral sternal border.
Equipment and Templating
Preoperative templating determines the anticipated plate length and contour. The surgeon must have access to a dedicated clavicle plating system, which typically includes pre-contoured superior and anteroinferior locking plates. Pointed reduction forceps (Weber clamps), a Freer elevator, and provisional Kirschner wires (K-wires) are essential for achieving and maintaining reduction prior to definitive fixation.
Detailed Surgical Approach and Technique
Surgical fixation is predominantly achieved via open reduction and internal fixation (ORIF) utilizing plate osteosynthesis, though intramedullary nailing represents a viable alternative for simple, transverse midshaft fractures.
Incision and Superficial Dissection
A transverse or slightly oblique incision is made centered over the fracture site. The incision can be placed directly over the superior aspect of the clavicle or slightly inferiorly (infraclavicular approach) to keep the resultant scar off the prominent superior ridge, thereby reducing hardware irritation and improving cosmesis.
Subcutaneous dissection proceeds through the adipose tissue to expose the platysma muscle. The platysma is incised in line with the skin incision. Meticulous hemostasis is critical here. The intermediate and medial branches of the supraclavicular nerve (arising from the cervical plexus, C3-C4) cross the clavicle from superior to inferior. Every effort must be made to identify, mobilize, and protect these sensory branches. Iatrogenic transection results in a predictable area of paresthesia over the anterior chest wall, which is a frequent source of postoperative patient dissatisfaction.
Deep Dissection and Fracture Exposure
The investing clavipectoral fascia is incised longitudinally along the anterior-superior border of the clavicle. Subperiosteal dissection is performed using a periosteal elevator to expose the fracture fragments. It is imperative to maintain the soft tissue attachments to comminuted butterfly fragments to preserve their vascular supply. Aggressive circumferential stripping of the periosteum dictates a higher risk of avascularity and subsequent nonunion.
The inferior aspect of the clavicle must be approached with extreme caution. Instruments such as Hohmann retractors should be placed carefully, ensuring they remain subperiosteal and do not plunge inferiorly into the subclavius muscle or the underlying neurovascular bundle.
Fracture Reduction Techniques
Reduction of a displaced midshaft clavicle fracture often requires overcoming the deforming forces: the sternocleidomastoid pulls the medial fragment superiorly and posteriorly, while the weight of the arm and the pectoralis major pull the lateral fragment inferiorly and medially.
Traction is applied to the arm while manipulating the fragments with pointed reduction forceps. In cases of oblique fractures or large butterfly fragments, interfragmentary lag screws (typically 2.7 mm or 3.5 mm cortical screws) are utilized to achieve absolute stability and anatomic reduction of the cortical tube. Once the main fragments are reduced and provisionally held with lag screws or K-wires, the definitive plate is applied.
Plate Application and Biomechanics
The choice between superior and anteroinferior plating depends on fracture morphology and surgeon preference.
1. Superior Plating: Biomechanically advantageous as it places the plate on the tension side of the bone. It allows for longer screw purchase in the broader lateral segment. However, superior plates are more prominent subcutaneously, leading to higher rates of symptomatic hardware requiring removal.
2. Anteroinferior Plating: Offers a safer trajectory for drilling (screws are directed posterosuperiorly, away from the neurovascular bundle). The hardware is better cushioned by the anterior soft tissues, reducing prominence. Biomechanically, it is slightly less optimal for resisting inferior bending forces but provides excellent resistance to the pull of the pectoralis major.
Pre-contoured locking plates (typically 3.5 mm systems) are applied. A minimum of three bicortical screws (six cortices) on each side of the fracture is mandatory for adequate construct stiffness. In osteoporotic bone or comminuted fractures, locking screws are utilized to create a fixed-angle construct.
Distal Clavicle Fracture Nuances
Distal third fractures (Neer Type II) require specialized techniques due to the small lateral segment and the disruption of the CC ligaments. Fixation options include:
* Pre-contoured Distal Clavicle Locking Plates: Featuring a cluster of small (2.4 mm or 2.7 mm) locking screws laterally.
* Coracoclavicular Augmentation: Heavy non-absorbable sutures or cortical button systems passed around or through the coracoid process to neutralize superior deforming forces while the bone heals.
* Hook Plates: Utilized when the lateral fragment is too small for screw purchase. The hook passes under the acromion. This construct requires routine removal at 3 to 6 months postoperatively to prevent acromial osteolysis and rotator cuff impingement.
Closure
The wound is irrigated copiously. The clavipectoral fascia is closed over the plate if possible. The platysma must be meticulously approximated with absorbable sutures to provide a robust soft-tissue envelope over the hardware and minimize scar widening. Subcutaneous and subcuticular closures follow.
Complications and Management
Despite high success rates, operative management of clavicle fractures carries a distinct complication profile. Surgeons must be adept at recognizing and managing these sequelae.
Summary of Surgical Complications
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage and Management Strategy |
|---|---|---|---|
| Hardware Prominence | 10% to 30% | Thin subcutaneous tissue, superior plate placement, use of reconstruction plates. | Hardware removal after clinical and radiographic evidence of solid union (typically > 12 months post-op). |
| Nonunion | 1% to 5% | Infection, inadequate fixation (too few cortices), excessive periosteal stripping, smoking. | Revision ORIF with rigid locking plate, autologous iliac crest bone grafting (ICBG), and optimization of host factors. |
| Incisional Numbness | 10% to 25% | Transection or traction injury to the supraclavicular nerves during superficial dissection. | Usually permanent but becomes less bothersome over time. Gabapentinoids for neuropathic pain. Prevention via meticulous dissection. |
| Infection | 1% to 4% | Poor soft tissue envelope, prolonged operative time, medical comorbidities (diabetes). | Superficial: Oral antibiotics. Deep: Surgical debridement, hardware retention if stable until union, suppressive IV antibiotics. |
| Neurovascular Injury | < 1% | Plunging drill bits, errant screw trajectory, aggressive inferior retractor placement. | Immediate vascular surgery consultation for subclavian vessel injury. Brachial plexus neuropraxia usually resolves with observation. |
| Adhesive Capsulitis | 2% to 5% | Prolonged postoperative immobilization, failure to initiate early glenohumeral ROM. | Aggressive physical therapy, intra-articular corticosteroid injections, rarely manipulation under anesthesia (MUA). |
Management of Nonunion
Aseptic nonunion is defined as a lack of clinical or radiographic progression of healing at 6 months post-injury. Patients typically present with pain, crepitus, and motion at the fracture site. Workup must include inflammatory markers (ESR, CRP) to rule out indolent infection. Revision surgery requires complete resection of the atrophic or hypertrophic nonunion site down to bleeding bone, recanalization of the medullary canal, rigid fixation with a robust locking plate, and biological augmentation, typically utilizing autologous iliac crest bone graft.
Hardware Failure
Catastrophic hardware failure (plate breakage or screw pullout) usually occurs within the first 6 to 8 weeks and is indicative of either an mechanically inadequate construct (e.g., bridging a highly comminuted fracture with a non-locking plate) or patient non-compliance with postoperative weight-bearing restrictions. Immediate revision osteosynthesis is indicated.
Post Operative Rehabilitation Protocols
Rehabilitation following clavicle ORIF must balance the need to protect the surgical construct with the imperative to prevent glenohumeral stiffness. Protocols are generally divided into four distinct phases.
Phase 1 Immediate Postoperative (Weeks 0 to 2)
The upper extremity is placed in a standard sling for comfort. The primary goal is pain control and protection of the soft tissues. Patients are instructed to perform active range of motion (AROM) of the elbow, wrist, and hand immediately to prevent distal stiffness. Pendulum exercises for the shoulder are initiated. Active shoulder elevation and lifting are strictly prohibited.
Phase 2 Early Mobilization (Weeks 2 to 6)
At the two-week mark, the surgical incision is evaluated for healing. The sling is gradually weaned for activities of daily living. Formal physical therapy commences with active-assisted range of motion (AAROM) utilizing pulleys and wand exercises. Forward elevation and abduction are generally limited to 90 degrees to prevent excessive rotational forces on the clavicle construct. Isotonic strengthening remains contraindicated.
Phase 3 Strengthening and Full ROM (Weeks 6 to 12)
Radiographs are obtained at 6 weeks. If early callus formation and maintenance of reduction are confirmed, the patient is cleared to progress to full, unrestricted active range of motion. Isometric strengthening of the rotator cuff and periscapular musculature (rhomboids, trapezius, serratus anterior) is initiated. Scapular dyskinesia is common following clavicle fractures and must be aggressively addressed to restore normal shoulder biomechanics. Light isotonic resistance is introduced late in this phase.
Phase 4 Return to Sport and Heavy Labor (Months 3 to 6)
Advanced strengthening and plyometric exercises are incorporated. Clearance for heavy labor, overhead sports, or contact sports requires definitive clinical union (absence of pain at the fracture site) and radiographic union (bridging trabecular bone across at least three cortices). This typically occurs between 12 and 16 weeks postoperatively.
Summary of Key Literature and Guidelines
The modern approach to clavicle fracture management is heavily influenced by several landmark studies that challenged the historical dogma of universal non-operative treatment.
The Canadian Orthopaedic Trauma Society (COTS) Trial
Published in 2007 in the Journal of Bone and Joint Surgery, the COTS multicenter randomized controlled trial is arguably the most influential paper in modern clavicle trauma literature. The study compared non-operative treatment (sling) versus ORIF with plate fixation for completely displaced midshaft clavicle fractures. The results demonstrated a significantly lower nonunion rate in the operative group (3% vs. 15%), faster time to radiographic union, and superior functional outcome scores (DASH and Constant scores) at one year. This study catalyzed a massive shift toward operative management for displaced fractures.
Predictive Factors for Nonunion
Robinson et al. conducted extensive cohort studies evaluating the natural history of clavicle fractures. They identified lack of cortical contact (100% displacement), comminution, advanced age, and female gender as independent risk factors for nonunion in non-operatively managed midshaft fractures. Furthermore, shortening of greater than 15 to 20 millimeters has been biomechanically and clinically correlated with altered scapular kinematics, decreased rotator cuff strength, and poor functional outcomes, serving as a primary relative indication for surgery.
Recent Trends and the Pendulum Swing
While the COTS trial led to a surge in surgical fixation, recent literature over the past five years has prompted a more nuanced approach. Long-term follow-up studies have highlighted the substantial burden of hardware-related complications and the high rate of secondary operations for plate removal. Furthermore, some recent randomized trials have shown that while early functional scores favor surgery, the long-term (2 to 5 year) functional differences between operatively and non-operatively managed patients may equalize, provided the non-operatively managed patients go on to osseous union.
Consequently, current academic guidelines emphasize a highly individualized, shared decision-making model. Surgeons must weigh the biomechanical severity of the fracture against the patient's physiologic age, functional demands, medical comorbidities, and tolerance for potential secondary surgeries. The contemporary orthopedic surgeon does not operate on every displaced clavicle but rather selectively intervenes to restore anatomy in patients who will definitively benefit from rigid stabilization and early mobilization.
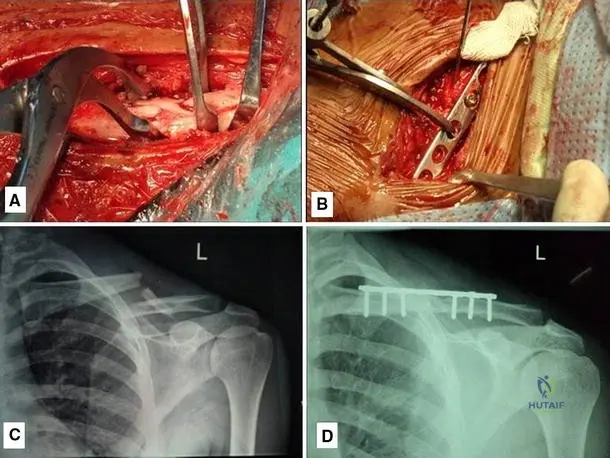
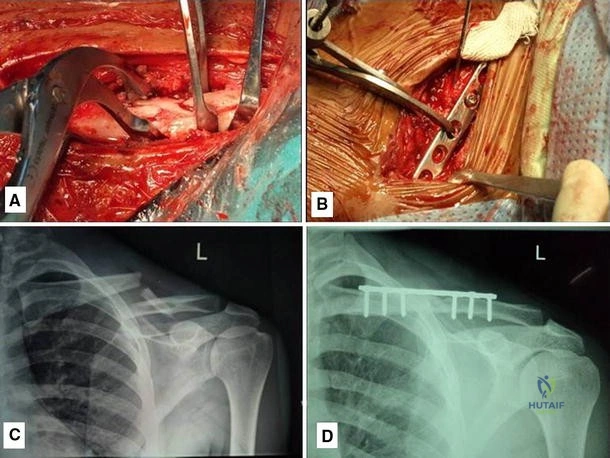
Clinical & Radiographic Imaging
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding clavicle-fractures-epidemiology-anatomy-and-treatment-options