Medial Clavicular Fragment Fractures: Risks, Symptoms, & Recovery

Key Takeaway
For anyone wondering about Medial Clavicular Fragment Fractures: Risks, Symptoms, & Recovery, Clavicle fractures comprise 2.6% of all fractures, typically resulting from falls onto the shoulder. Middle third fractures are most common (80%), with medial third fractures accounting for 5%. Patients often present with a prominent proximal fracture end, which for a medial clavicular fragment may tent the skin. A thorough neurovascular evaluation is crucial.
Comprehensive Introduction and Patho-Epidemiology
Clavicle fractures represent a highly prevalent orthopedic injury, accounting for approximately 2.6% of all fractures presenting to emergency departments and comprising an overwhelming 44% to 66% of all fractures involving the shoulder girdle. The anatomic distribution of these fractures is heavily skewed toward the diaphyseal region, with middle-third fractures accounting for roughly 80% of all clavicular injuries. Fractures of the lateral (distal) third account for approximately 15%, while medial (proximal) third fractures are the least common, representing roughly 5% of cases. Despite their relative infrequency, medial clavicular fragment fractures present unique diagnostic and therapeutic challenges due to their proximity to vital mediastinal and neurovascular structures, as well as the dense ligamentous constraints of the sternoclavicular joint.

The pathogenesis of clavicle fractures is intrinsically linked to the biomechanical forces exerted on the shoulder girdle. The vast majority of these injuries—approximately 87%—occur secondary to a direct lateral impact or fall onto the affected shoulder. This mechanism generates a complex bending and shear force that is transmitted axially along the clavicle, typically exceeding the critical buckling load at the transition zone of the midshaft. Direct traumatic impact to the anterior chest or clavicle accounts for only 7% of cases, while falls onto an outstretched hand (FOOSH), historically thought to be a primary driver of these injuries, account for a mere 6%. In rare clinical scenarios, clavicle fractures may manifest secondary to violent muscle contractions during grand mal seizures, as pathologic fractures in the setting of metabolic or neoplastic bone disease, or as insidious stress fractures in elite overhead athletes.
Historically, the natural history of clavicle fractures was viewed through a lens of benign neglect. Landmark epidemiological studies published in the 1960s by Neer and Rowe established a long-standing orthopedic dogma that nonoperative management of midshaft clavicle fractures yielded universally excellent results, with nonunion rates cited at a remarkably low 0.1% to 0.8%. Furthermore, these early series suggested that operative intervention inherently increased the risk of nonunion (up to 4.6%) and infection. However, modern prospective multicenter trials have fundamentally dismantled this paradigm. Contemporary data demonstrate that significantly displaced midshaft and medial fragment fractures treated nonoperatively are associated with nonunion rates approaching 15%, alongside substantial risks of symptomatic malunion, persistent shoulder dyskinesia, and inferior functional outcomes.
Consequently, the epidemiology of surgical intervention for clavicle fractures has shifted dramatically over the past two decades. As our understanding of shoulder kinematics and the deleterious effects of clavicular shortening has evolved, so too have our indications for osteosynthesis. The modern orthopedic surgeon must possess a nuanced understanding of the epidemiological risk factors that portend poor outcomes—such as advanced age, female sex, smoking status, and severe initial fracture displacement—to appropriately stratify patients for either conservative immobilization or surgical fixation. This chapter will provide an exhaustive, evidence-based review of medial, midshaft, and lateral clavicle fractures, detailing the surgical anatomy, clinical evaluation, and advanced operative techniques required to optimize patient recovery.
Detailed Surgical Anatomy and Biomechanics
The clavicle is an anatomically unique osteological structure, serving as the sole rigid osseous link between the axial skeleton and the upper appendicular skeleton. Embryologically, it is the first bone in the human body to begin ossification, initiating via a combination of intramembranous and endochondral ossification during the fifth week of gestation. Conversely, the medial epiphyseal ossification center is the last in the body to fuse, typically closing between 22 and 25 years of age. This delayed fusion is of paramount clinical importance, as trauma to the medial clavicle in young adults frequently results in a physeal separation (Salter-Harris equivalent injury) rather than a true sternoclavicular dislocation.
Morphologically, the clavicle exhibits a complex, S-shaped double curve when viewed in the axial plane. The medial two-thirds are convex anteriorly, providing a critical protective vault for the underlying neurovascular bundle, while the lateral one-third is concave anteriorly. The cross-sectional anatomy of the bone is highly variable; the medial end is expanded, prismatic, and robust, gradually transitioning into a narrow, tubular midshaft, and finally flattening out into a broad, flat expanse at the lateral acromial end. Unlike typical long bones, the clavicle lacks a well-defined medullary canal, consisting instead of dense, highly vascular trabecular bone encased in a thick cortical shell. The transition zone between the tubular midshaft and the flat lateral segment represents a biomechanical stress riser, explaining the overwhelming preponderance of diaphyseal fractures under axial loading conditions.
The biomechanical stability and functional capacity of the clavicle are dictated by its robust muscular and ligamentous attachments. Proximally and medially, the strong costoclavicular (rhomboid) ligaments anchor the clavicle to the first rib, while the sternocleidomastoid muscle exerts a profound superior and posterior deforming force on medial fracture fragments. Inferiorly, the pectoralis major and subclavius muscles depress the medial and midshaft segments. Distally, the coracoclavicular (CC) ligament complex—comprising the conoid and trapezoid ligaments—provides paramount vertical stability to the acromioclavicular (AC) joint. The conoid ligament is situated more posteromedially, while the trapezoid is anterolateral. These ligaments are inherently stronger than the AC joint capsule itself. In the setting of a fracture, the interplay of these muscular forces predictably dictates fragment displacement: the proximal fragment is typically elevated by the sternocleidomastoid, while the distal fragment is depressed and translated medially by the weight of the arm and the pull of the pectoralis major and latissimus dorsi.
From a surgical perspective, the neurovascular relations of the clavicle are unforgiving. The medial one-third of the clavicle acts as a direct protective strut over the brachial plexus, the subclavian artery and vein, and the superior apical pleura of the lung. The subclavian vein lies intimately posterior and inferior to the medial clavicle, separated only by the thin subclavius muscle. Furthermore, the clavicle is entirely subcutaneous, covered only by the platysma muscle and the superficial fascia. The supraclavicular nerves, originating from the cervical plexus (C3-C4), branch out deep to the platysma and cross anterior to the clavicle to provide sensation to the anterior chest wall. Iatrogenic injury to these nerve branches during surgical exposure is exceedingly common and results in predictable paresthesias or painful neuromas, underscoring the need for meticulous superficial dissection.
Clinical and Radiographic Evaluation
The clinical evaluation of a patient with a suspected clavicle fracture begins with a thorough trauma assessment, as these injuries frequently occur in the setting of high-energy mechanisms such as motor vehicle collisions or high-velocity sports trauma. Patients classically present with localized pain, swelling, and an obvious clinical deformity over the clavicle. The patient typically exhibits antalgic posturing, splinting the affected extremity by adducting the arm across the chest and supporting the elbow with the contralateral hand to unload the weight of the shoulder girdle. The proximal fracture fragment is usually prominent beneath the skin, driven superiorly by the sternocleidomastoid muscle.
A rigorous physical examination is mandatory, with specific attention directed toward the integrity of the overlying soft tissue envelope and the distal neurovascular status. Severe skin tenting, characterized by blanching and ischemia of the overlying dermis, represents an impending open fracture and necessitates urgent surgical intervention. A meticulous neurovascular examination must be documented, assessing the sensory and motor distribution of all terminal branches of the brachial plexus, alongside palpable distal pulses and capillary refill. The anterior chest wall must be auscultated to ensure symmetric breath sounds; diminished breath sounds may indicate an ipsilateral pneumothorax or hemothorax secondary to an apical lung injury or associated rib fractures. Up to 9% of patients with clavicle fractures present with concomitant rib fractures, and high-energy medial third fractures carry a distinct risk of traction injuries to the brachial plexus.
Radiographic evaluation of the clavicle requires specific, targeted orthogonal views to accurately assess fracture morphology, comminution, and the degree of displacement. A standard anteroposterior (AP) radiograph of the clavicle is the initial screening tool, but it is often insufficient for operative planning due to the superimposition of the thoracic cage and the clavicle's inherent curvature. Therefore, a 30-degree cephalad tilt view (often referred to as a serendipity view) is highly recommended. This projection projects the clavicle above the thoracic anatomy, allowing for a clear assessment of superior-inferior translation and true shortening. In pediatric populations, an apical oblique view—taken with the shoulder angled 45 degrees toward the X-ray source and the beam angled 20 degrees cephalad—can be particularly useful for identifying minimally displaced greenstick fractures.
Advanced cross-sectional imaging with Computed Tomography (CT) is increasingly utilized, particularly for complex fracture patterns involving the medial and lateral articular extremities. For medial clavicular fragment fractures (Group III), a CT scan with 3D reconstructions is considered the gold standard. It is indispensable for differentiating a true intra-articular sternoclavicular fracture-dislocation from a medial epiphyseal physeal separation in young adults. Furthermore, CT imaging is highly valuable in assessing distal third (Group II) fractures to precisely identify the fracture's relationship to the coracoclavicular ligaments and to rule out occult intra-articular extension into the acromioclavicular joint, which may dictate the need for specific joint-spanning or ligament-reconstruction surgical techniques.
Classification Systems
The classification of clavicle fractures is essential for standardizing communication, guiding therapeutic decision-making, and predicting clinical outcomes. The most universally recognized system is the Allman Classification, which categorizes fractures based on their anatomical location along the bone. Group I fractures involve the middle third of the clavicle and are the most common, comprising 80% of all cases. In these injuries, the proximal and distal segments remain relatively secured by their respective ligamentous and muscular attachments, though significant displacement can occur if the periosteal sleeve is entirely disrupted. Group II fractures involve the distal third (15%), and Group III fractures involve the proximal or medial third (5%).
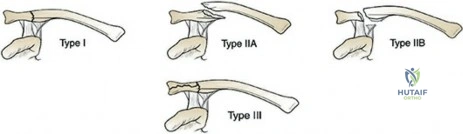
Group II (distal third) fractures are further subclassified by Neer based on the relationship of the fracture line to the coracoclavicular (CC) ligaments, which carries profound implications for fracture stability and the risk of nonunion. Type I fractures are minimally displaced, with the fracture line occurring interligamentously between the conoid and trapezoid, or laterally with intact CC ligaments. Type II fractures are displaced secondary to a fracture medial to the CC ligaments, resulting in a loss of vertical stability and a notoriously high incidence of nonunion (up to 30% if treated nonoperatively). Type II is subdivided into Type IIA (conoid and trapezoid attached to the distal segment) and Type IIB (conoid torn, trapezoid attached to the distal segment). Type III fractures involve the articular surface of the AC joint without ligamentous injury, often leading to late post-traumatic arthrosis.
Group III (medial third) fractures, the primary focus of highly specialized reconstructive efforts, are subdivided into five distinct types based on morphology and articular involvement. Type I represents minimally displaced fractures where the costoclavicular ligaments remain intact, providing inherent stability. Type II indicates a displaced fracture, often requiring surgical reduction due to the deforming forces of the sternocleidomastoid. Type III denotes an intra-articular fracture extending into the sternoclavicular joint. Type IV represents an epiphyseal separation, predominantly seen in patients under 25 years of age, which can easily be misdiagnosed as an SC joint dislocation. Finally, Type V describes a severely comminuted medial fracture, often resulting from massive direct axial trauma.
In addition to the Allman and Neer systems, the Orthopaedic Trauma Association (OTA) / AO Foundation Fracture and Dislocation Classification Compendium provides a highly rigorous, alphanumeric system for clavicle fractures (designated as bone 15). This system classifies the bone into proximal, diaphyseal, and distal segments (15.1, 15.2, 15.3) and further stratifies based on fracture pattern (simple, wedge, multifragmentary). While the OTA classification is unparalleled for research purposes and large database registries, the Allman and Neer classifications remain the most clinically utilized frameworks for daily orthopedic practice and surgical planning.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative versus nonoperative management of clavicle fractures has undergone a massive paradigm shift. While historical algorithms heavily favored conservative management, modern evidence-based medicine dictates a much more aggressive surgical approach for specific fracture morphologies. The overarching goals of treatment are to achieve pain relief, restore normal shoulder girdle anatomy, maximize functional range of motion, and prevent the sequelae of malunion and nonunion. Nonoperative management—typically consisting of a simple sling for 4 to 6 weeks—remains the gold standard for minimally displaced fractures, pediatric fractures, and patients with prohibitive medical comorbidities. Notably, studies have shown that a simple sling provides equivalent clinical outcomes to a figure-of-eight bandage, while offering superior patient comfort and drastically fewer skin complications.
Absolute indications for the operative management of acute clavicle fractures are universally agreed upon and represent orthopedic emergencies or urgencies. These include open fractures, fractures associated with progressive neurovascular compromise (such as a brachial plexus palsy or subclavian artery occlusion), and severe skin tenting where the ischemic dermis has the potential to progress to a secondary open fracture. In these scenarios, immediate surgical exploration, decompression of the neurovascular elements, and rigid internal fixation are mandatory to prevent catastrophic limb-threatening or life-threatening complications.
Relative indications for surgery are more nuanced and require a shared decision-making process between the surgeon and the patient. Current literature strongly supports operative intervention for midshaft fractures demonstrating substantial displacement (defined as >100% translation with no cortical contact), severe comminution (the classic "Z-deformity"), and absolute shortening of greater than 1.5 to 2.0 centimeters. Patients with these radiographic parameters who are treated conservatively face a significantly higher risk of nonunion, persistent shoulder dysfunction, decreased endurance, and dissatisfaction with the cosmetic deformity. Additional relative indications include polytrauma patients requiring early mobilization, "floating shoulder" variants (ipsilateral clavicle and scapular neck fractures), and high-demand overhead athletes or manual laborers.
| Category | Operative Indications | Contraindications to Surgery |
|---|---|---|
| Absolute | Open fracture, Acute neurovascular compromise, Impending open fracture (severe skin blanching/tenting) | Active surgical site infection, Medically unfit for anesthesia (severe cardiopulmonary disease) |
| Relative | >100% displacement, >1.5-2.0 cm shortening, Z-deformity/comminution, Polytrauma, Floating shoulder, Symptomatic nonunion | Minimally displaced fractures, Poor soft tissue envelope (severe abrasions/burns), Non-ambulatory/low-demand patient |
| Distal (Group II) | Type IIA and IIB displaced fractures (due to high nonunion risk) | Type I and Type III non-displaced/articular fractures |
| Medial (Group III) | Posterior displacement compressing mediastinal structures, Severe symptomatic displacement | Minimally displaced Type I, Type IV physeal injuries (often remodel well) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful clavicular osteosynthesis. The surgeon must carefully evaluate orthogonal radiographs and CT scans to determine the fracture morphology, the degree of comminution, and the exact location of the fracture lines relative to the ligamentous insertions. Digital templating is highly recommended to select the appropriate implant type, length, and screw trajectory. For plate fixation, the surgeon must decide between a superiorly placed plate or an anteroinferiorly placed plate. Superior plating provides optimal biomechanical resistance to the tensile forces exerted on the convex surface of the clavicle but carries a higher risk of symptomatic hardware prominence. Anteroinferior plating utilizes longer, safer screw trajectories directed away from the subclavian vessels and is associated with less hardware irritation, though it may be technically more demanding to contour.
Patient positioning in the operating room is critical for optimizing surgical exposure and facilitating intraoperative fluoroscopy. The patient is typically placed in a modified beach-chair position or supine with a bump placed vertically between the scapulae. The beach-chair position utilizes gravity to assist in reducing the distal fragment, which is naturally pulled inferiorly by the weight of the arm. The head and neck must be carefully positioned and stabilized, often utilizing a Mayfield headrest or a foam donut, ensuring the cervical spine remains neutral. Anesthesia typically involves a combination of general endotracheal anesthesia and a regional interscalene nerve block, which provides excellent intraoperative muscle relaxation and profound post-operative analgesia.
Intraoperative fluoroscopy must be seamlessly integrated into the surgical setup. The C-arm is usually brought in from the contralateral side of the table or positioned directly at the head of the bed if space permits. It is imperative to confirm that clear, orthogonal views of the entire clavicle—from the sternoclavicular joint to the acromioclavicular joint—can be obtained before the patient is prepped and draped. The surgical prep should extend from the mandible superiorly to the nipple line inferiorly, and from the contralateral sternal border to the ipsilateral posterior axillary line. The affected arm should be draped free to allow for dynamic intraoperative manipulation, which is often essential for achieving indirect reduction of complex fracture patterns.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the clavicle requires a meticulous dissection strategy to preserve the fragile soft tissue envelope and avoid iatrogenic nerve injury. A transverse or slightly oblique incision is typically utilized, centered directly over the fracture site. Some surgeons prefer an infraclavicular incision, placed slightly inferior to the clavicular ridge, to ensure the surgical scar does not lie directly over the hardware, thereby reducing post-operative skin irritation. As the dissection proceeds through the subcutaneous tissue and the platysma muscle, extreme care must be taken to identify, mobilize, and protect the descending branches of the supraclavicular nerves. Transection of these nerves results in a predictable area of numbness over the anterior chest and carries a risk of painful neuroma formation.
Once the clavipectoral fascia is incised, the fracture site is exposed. A fundamental principle of modern fracture surgery is the preservation of the periosteal blood supply. Therefore, soft tissue stripping should be strictly limited to the fracture margins necessary for reduction. Large, comminuted butterfly fragments should not be devitalized; instead, they should be incorporated into the construct using indirect reduction techniques or lag screws if their size permits. The fracture is reduced using a combination of manual traction on the arm, pointed reduction forceps, and elevators. In cases of chronic nonunion or severe shortening, a laminar spreader or a specialized distractor may be required to restore the anatomical length of the clavicle.
Open Reduction and Internal Fixation (ORIF) with plate osteosynthesis remains the gold standard for diaphyseal and medial fractures. Pre-contoured, anatomically specific locking plates have largely replaced traditional reconstruction plates, offering superior biomechanical stability, especially in osteoporotic bone. If a superior plating technique is chosen, the plate acts as a tension band. Cortical screws are typically sufficient for diaphyseal bone, while locking screws are reserved for short peri-articular segments or comminuted zones. When drilling
