Beyond Plates: Intramedullary Fixation for Displaced Midshaft Clavicle
Key Takeaway
Learn more about Beyond Plates: Intramedullary Fixation for Displaced Midshaft Clavicle and how to manage it. A displaced midshaft clavicle refers to a fracture in the middle third of the S-shaped collarbone, the bone's thinnest and most vulnerable part. This region, unsupported by ligaments or muscles, often breaks due to a direct impact on the shoulder, such as falling. Displacement means the fractured bone segments are out of normal alignment.
Comprehensive Introduction and Patho-Epidemiology
The clavicle is universally recognized as one of the most frequently fractured bones in the human body, accounting for approximately 2.6% to 4% of all adult fractures and up to 44% of all shoulder girdle injuries. Within the clavicle itself, the diaphysis or middle third is the site most susceptible to structural failure, representing nearly 80% of all clavicular fractures. This distinct vulnerability is anatomically dictated; the midclavicular region constitutes the thinnest and narrowest segment of the bone and remains the only substantial area entirely devoid of muscular or ligamentous reinforcement. Furthermore, the midshaft serves as a critical transitional zone, both in terms of cross-sectional morphology and multiplanar curvature. It represents the precise inflection point where the flattened, horizontally oriented lateral segment transitions into the more robust, tubular, and prismatic medial portion. Because of the clavicle’s unique S-shaped biomechanical architecture, an axial load applied to the shoulder girdle generates an exponentially amplified tensile force concentrated along the anterior midcortex, effectively creating a virtual right angle of force vectors at the midclavicle.

The pathogenesis of these fractures is overwhelmingly linked to direct mechanical trauma applied to the lateral aspect of the shoulder, rather than the classically taught mechanism of a fall onto an outstretched hand (FOOSH). In a landmark biomechanical and epidemiological analysis, Stanley and associates meticulously evaluated 106 patients with acute clavicle fractures. Their compelling data revealed that 87% of these injuries were the direct result of a fall onto the lateral point of the shoulder, 7% were caused by a direct blow to the clavicle itself, and a mere 6% were associated with a FOOSH mechanism. Stanley astutely postulated that in patients who initially reported hitting the ground with an outstretched hand, the kinetic energy transfer inevitably caused the shoulder to become the secondary and primary load-bearing contact point with the ground. Biomechanical modeling demonstrates that a compressive force merely equivalent to the patient's body weight routinely exceeds the critical buckling load of the clavicular diaphysis, resulting in catastrophic structural failure and displacement.
Historically, the natural history of displaced midshaft clavicle fractures was viewed through a lens of benign neglect, heavily influenced by seminal studies from the 1960s. Both Neer and Rowe published massive retrospective series advocating for closed functional treatment, citing astonishingly low nonunion rates of 0.1% and 0.8%, respectively, while paradoxically reporting higher nonunion rates (4.6% and 3.7%) following the rudimentary operative interventions of their era. However, modern prospective, randomized, and rigorously controlled outcome studies have fundamentally dismantled this historical dogma. Contemporary literature unequivocally demonstrates that nonunion following conservative management is vastly more common than previously recognized, approaching 15% to 20% in completely displaced fractures. Furthermore, a significant percentage of patients who achieve radiographic union do so with symptomatic malunion. Malunion characterized by shortening greater than 15 to 20 mm fundamentally alters the resting kinematics of the shoulder girdle, leading to profound alterations in scapulothoracic rhythm, chronic pain, and objective weakness in overhead function.
Pioneering work by McKee and colleagues prospectively identified patients with symptomatic malunion of the midclavicle following standard closed treatment. In their cohort, every patient exhibited clavicular shortening exceeding 15 mm, uniformly reported profound dissatisfaction with their functional outcome, and ultimately required complex corrective osteotomy. Postoperatively, following restoration of anatomic length and rigid fixation, all patients demonstrated statistically significant improvements in standardized functional scoring and subjective satisfaction. Similarly, Hill and associates reviewed 52 completely displaced midshaft clavicle fractures, establishing a definitive correlation between initial shortening greater than 20 mm and a high incidence of nonunion, intractable pain, and abysmal functional results. Eskola and coworkers further corroborated these findings in a robust review of 89 malunions, cementing the modern orthopedic consensus that shortening beyond 15 mm is an independent predictor of significant shoulder discomfort and kinetic chain dysfunction. This paradigm shift has paved the way for advanced operative strategies, specifically highlighting the biologic and biomechanical advantages of intramedullary fixation over traditional plate osteosynthesis.
Detailed Surgical Anatomy and Biomechanics
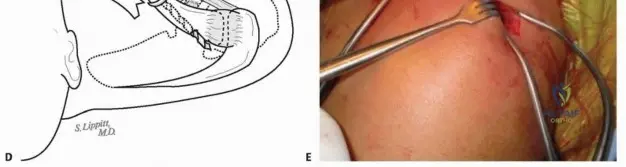
The clavicle is an embryological anomaly and a biomechanical marvel, distinguished as the only long bone in the human skeleton to undergo ossification through a complex combination of both intramembranous and endochondral pathways. This dual ossification process contributes to its unique dense trabecular internal architecture and the distinct lack of a uniform, well-defined medullary canal—a factor that historically complicated intramedullary fixation efforts. Morphologically, the clavicle is configured in a pronounced S-shape, featuring a double curve that is critical for its function as a dynamic strut. The larger medial curve presents with an anterior apex, while the lateral curve features a posterior apex. This specific geometric configuration is not merely structural; the pronounced medial curvature actively expands the retroclavicular space, providing a critical bony shield for the underlying, highly vulnerable neurovascular structures, including the brachial plexus and the subclavian vessels.
As one traverses the clavicle from lateral to medial, the cross-sectional anatomy undergoes a dramatic and continuous transformation. The lateral third is distinctly flattened in the superoinferior plane, optimizing the surface area for the robust coracoclavicular ligamentous complex. Moving medially, the midportion rapidly transitions into a tubular, diaphyseal structure, which then progressively expands into a bulky, prismatic morphology at the medial sternal articulation. Throughout its entire length, the clavicle remains intimately subcutaneous, covered superiorly only by the thin, diaphanous fibers of the platysma muscle and the dermal layers. The supraclavicular nerves, which originate from the cervical plexus (C3-C4) and provide essential sensory innervation to the skin overlying the clavicle and anterior chest, arborize precisely deep to the platysma. Iatrogenic injury to these delicate nerves during surgical exposure is a notorious cause of postoperative chest wall numbness and painful neuroma formation, demanding meticulous blunt dissection techniques.

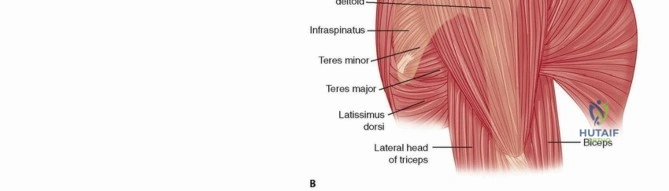
The clavicle is anchored at both extremities by some of the most formidable ligamentous complexes in the human body. Strong capsular and extracapsular ligaments securely tether the medial end to the sternum and the first rib (costoclavicular ligaments), while the lateral end is rigidly bound to the acromion and the coracoid process (conoid and trapezoid ligaments). The muscular attachments are similarly robust and distinctly polarized. Proximal muscular forces are driven by the sternocleidomastoid, the clavicular head of the pectoralis major, and the subclavius, which collectively exert massive superior and medial deforming forces on the proximal fracture fragment. Conversely, the distal fragment is subjected to the inferior gravitational pull of the upper extremity and the medializing forces of the deltoid and trapezius. When structural continuity is disrupted at the midshaft, these unopposed muscular forces invariably lead to the classic clinical deformity: a superiorly displaced medial fragment and an inferiorly, medially translated lateral fragment.

Biomechanically, the intact clavicle functions as a rigid, fixed-length strut that projects the upper extremity laterally, away from the thorax. This vital lateralization optimizes the resting length-tension relationship of the massive musculature spanning the shoulder girdle, enabling the generation and seamless transmission of tremendous kinetic forces from the axial skeleton to the appendicular skeleton. When this strut is compromised and allowed to heal in a shortened position, the entire shoulder girdle protracts, the scapula anteriorly tilts, and the glenoid version is altered. This cascade of biomechanical derangements reduces the efficiency of the rotator cuff, impinges the subacromial space, and accelerates fatigue in the periscapular stabilizers. Therefore, the primary goal of modern operative intervention, particularly via intramedullary fixation, is not merely achieving bony union, but the precise restoration of this critical anatomical strut to its native, pre-injury length and alignment.
Exhaustive Indications and Contraindications
The decision-making algorithm for the operative management of acute midshaft clavicle fractures has evolved significantly, transitioning from a stance of universal nonoperative care to a highly nuanced, patient-specific approach. Absolute indications for immediate surgical intervention are universally recognized and include open fractures, fractures associated with acute neurovascular compromise (such as subclavian artery intimal tearing or brachial plexus compression), and scenarios involving impending skin necrosis where severe displacement causes ischemic tenting of the overlying dermis. Additionally, the presence of a "floating shoulder"—defined as a displaced midshaft clavicle fracture with a concomitant unstable fracture of the scapular neck—mandates stabilization of the clavicular strut to restore the suspensory complex of the upper extremity. Polytrauma patients with severe associated chest injuries, such as flail chest or bilateral pulmonary contusions, also represent absolute indications, as rigid fixation of the clavicle facilitates aggressive pulmonary toilet, early mobilization, and the use of the upper extremities for bed transfers and ambulation.

Relative indications, which now encompass the vast majority of operative cases, center heavily on the degree of initial fracture displacement and the precise measurement of bony shortening. High-level evidence strongly supports operative fixation for fractures demonstrating greater than 15 to 20 mm of absolute shortening, especially when accompanied by significant shoulder girdle protraction, complete lack of cortical contact (100% displacement), or severe comminution (such as a vertical Z-type fracture pattern). In a definitive multicenter, randomized, prospective clinical trial, Altamimi and McKee demonstrated that operative fixation of these specific displaced patterns not only drastically reduced the rates of both malunion and nonunion but also provided significantly superior functional outcomes across all validated scoring metrics when compared to matched nonoperative cohorts. For the high-demand athlete or heavy manual laborer, these relative indications are frequently upgraded to operative mandates to ensure a rapid, predictable return to pre-injury performance levels.
When operative intervention is elected, the surgeon must carefully weigh the distinct advantages and limitations of intramedullary (IM) fixation versus traditional superior or anteroinferior plate osteosynthesis. The potential advantages of IM fixation are profoundly biological; the technique requires minimal to no soft tissue stripping, thereby preserving the critical periosteal blood supply and the enveloping fracture hematoma, which theoretically accelerates the formation of a robust fibrocartilaginous callus. Furthermore, IM nailing requires a substantially smaller incision, resulting in superior cosmesis—a non-trivial consideration for many patients. The centrally placed load-sharing device also mitigates the stress-shielding effects commonly seen with rigid locking plates, and subsequent hardware removal, if necessary, is vastly less morbid and does not leave the bone riddled with stress-concentrating screw holes. However, IM fixation is not without its disadvantages. Historically, smooth pins suffered from catastrophic migration and an inability to resist torsional forces. While modern locked IM devices have largely mitigated migration through medial and lateral locking mechanisms, IM nails inherently provide less absolute rotational stability compared to dual-plate constructs and remain susceptible to fatigue breakage in cases of delayed union.
| Parameter | Intramedullary Fixation | Plate Osteosynthesis |
|---|---|---|
| Primary Indications | Simple midshaft fractures (2B1, 2B2), moderate comminution with cortical contact, high cosmetic concern. | Severe comminution lacking cortical contact, distal/proximal third fractures, revision for nonunion. |
| Absolute Contraindications | Active local infection, obliterated medullary canal, extreme segmental comminution. | Active local infection, critically poor soft tissue envelope (relative). |
| Biomechanical Profile | Load-sharing, relative stability, promotes secondary bone healing (callus). | Load-bearing, absolute stability (if compressed), promotes primary bone healing. |
| Soft Tissue Impact | Minimal periosteal stripping, preservation of fracture hematoma. | Extensive periosteal stripping, high risk of supraclavicular nerve injury. |
| Hardware Removal | Minimally invasive, low risk of subsequent refracture. | Requires extensive re-exposure, significant risk of refracture through screw holes. |
Contraindications specific to intramedullary fixation must be rigorously respected to prevent intraoperative disasters. The most critical anatomical contraindication is an excessively narrow or obliterated medullary canal that physically precludes the passage of the implant, a scenario occasionally encountered in pediatric patients, small-statured females, or patients with sclerotic bone dysplasias. Extreme segmental comminution, where the medial and distal main fragments lack any potential for direct cortical contact after reduction, represents another strong contraindication, as the IM nail cannot adequately maintain length against massive compressive muscular forces without bony apposition. Active infection, whether local or systemic, remains an absolute contraindication for any internal fixation device. Preoperative templating and meticulous evaluation of orthogonal radiographs are paramount in identifying these anatomical constraints before the patient enters the operating theater.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful intramedullary clavicle fixation, beginning with the acquisition of high-quality, orthogonal radiographic projections. Standard anteroposterior (AP) views of the shoulder are notoriously inadequate for assessing the true multiplanar displacement of a clavicular diaphysis. Therefore, it is absolutely essential to obtain dedicated 45-degree cephalic tilt and 45-degree caudal tilt views. In practical clinical application, a 20- to 60-degree cephalic tilt view is often optimal for throwing the clavicle clear of the dense, overlapping thoracic structures and ribs. These specialized projections allow the surgeon to accurately determine the fracture pattern, the presence and orientation of butterfly fragments, and the true degree of superior/inferior and anterior/posterior translation. The radiographic film must be sufficiently large to encompass the entire clavicle, including the acromioclavicular (AC) and sternoclavicular (SC) joints, as well as the scapulothoracic articulation and upper lung fields, to comprehensively rule out associated injuries such as scapular neck fractures or subtle pneumothoraces.

Once the imaging is secured, digital or analog templating is performed to confirm the feasibility of intramedullary fixation. The surgeon must scrutinize the middle third of the bone to ensure the medullary canal is of sufficient diameter to accommodate the selected implant. While modern flexible-to-rigid IM devices are highly adaptable, a canal diameter of less than 3.0 mm may require aggressive reaming or necessitate an intraoperative pivot to plate osteosynthesis. The surgeon must also evaluate the curvature of the medial segment to anticipate the trajectory of the guiding instruments and the final resting position of the implant's medial locking mechanism. If significant comminution is present, the surgeon must mentally map the reduction sequence, ensuring that the primary medial and lateral fragments can be brought into intimate cortical contact over the nail to prevent postoperative shortening and implant fatigue.

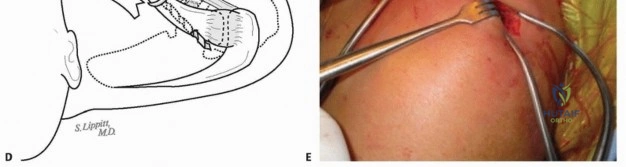
Patient positioning in the operating room is a critical phase that demands careful coordination between the orthopedic surgeon and the anesthesia team. There are two highly effective options for patient positioning, both designed to facilitate unhindered use of a C-arm fluoroscopy unit while providing excellent access to the shoulder girdle. The preferred method for many academic surgeons is the modified beach-chair position. The patient is placed on a specialized radiolucent OR table equipped with a shoulder-positioning device that allows the posterior shoulder area to remain completely exposed and unsupported. The C-arm is brought in from the head of the bed, with the gantry rotated upside down and angled slightly away from the operative shoulder, oriented with a cephalic tilt. This configuration allows for rapid, seamless acquisition of orthogonal views without moving the patient or compromising the sterile field. The operative arm is prepped entirely free and placed in a sterile articulated arm holder, which serves as an invaluable assistant for manipulating the upper extremity to aid in indirect fracture reduction.
Alternatively, the patient can be positioned perfectly supine on a completely radiolucent Jackson surgical table. In this configuration, a 1-liter intravenous fluid bag is placed longitudinally under the affected shoulder, specifically medial to the scapular border. This bump forces the shoulder girdle into relative retraction, aiding significantly in overcoming the typical anterior protraction deformity associated with displaced clavicle fractures. The C-arm is brought in perpendicular to the patient from the non-operative side of the table, remaining entirely out of the primary surgeon's working space. As with the beach-chair setup, the arm is prepped free and secured in an arm holder. Both positioning strategies require meticulous attention to pressure point padding and secure head positioning to prevent cervical spine hyperextension or iatrogenic brachial plexus traction injuries during the often forceful reduction maneuvers.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Dissection, and Nerve Protection
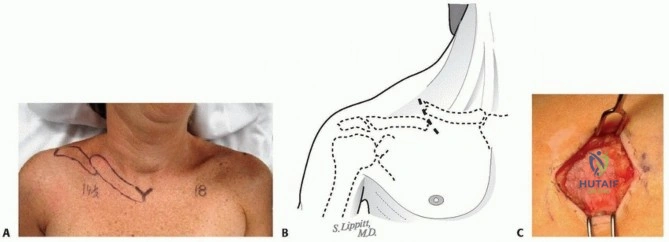
The surgical field is prepped and draped with wide margins, exposing the entire clavicle from the sternal notch to the lateral edge of the acromion, allowing for unhindered palpation of anatomical landmarks. Prior to incision, the clavicle, the exact fracture site (confirmed via fluoroscopy), and the surrounding critical anatomy are marked with a sterile pen. Utilizing the C-arm, the precise location for the incision is identified; optimally, this should be centered over the distal end of the medial fracture fragment, meticulously aligned with the anatomic Langer skin lines of the neck to ensure superior cosmetic healing. A remarkably small 2- to 3-cm skin incision is sharply made through the epidermis and dermis. The dissection proceeds through the minimal subcutaneous fat down to the glistening fascia of the platysma muscle. Although the subcutaneous layer is thin, it is imperative to gently elevate full-thickness flaps—incorporating both skin and subcutaneous tissue—around the entire circumference of the incision. This maneuver creates a mobile window that can be shifted medially and laterally, vastly expanding the effective exposure without extending the skin incision.
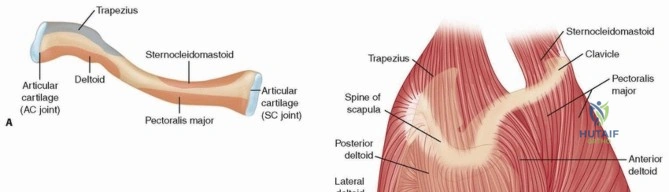
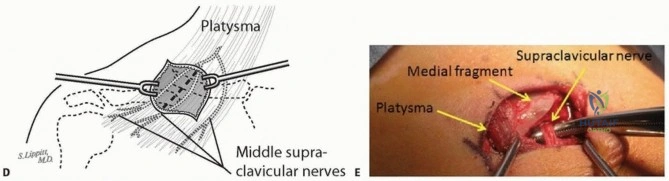
Once the platysma is exposed, it must be bluntly split in line with its vertically oriented fibers. Sharp division of the platysma is strongly discouraged, as the delicate supraclavicular nerves course unpredictably just deep to this muscle layer. The middle branches of the supraclavicular nerve are frequently encountered directly overlying the midclavicular fracture site. These nerves must be meticulously identified, gently mobilized using vessel loops or blunt retractors, and rigorously protected throughout the procedure. Following nerve protection, the fracture hematoma is encountered. The hematoma is carefully evacuated, and the fracture ends are identified. A cardinal rule of intramedullary clavicle fixation is the absolute preservation of the periosteal sleeve. The surgeon may only minimally elevate the periosteum at the immediate fracture edges (1-2 mm) to facilitate visualization of the medullary canal. There is zero tolerance for the extensive periosteal stripping routinely required for plate fixation. Debris, interposed muscle, and organized clot are removed from the fracture site using a curette, while any attached butterfly fragments are left meticulously attached to their soft tissue hinges to preserve their precarious blood supply.
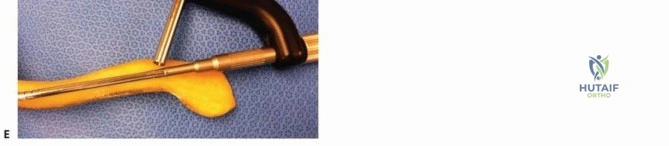
Canal Preparation and Device Insertion
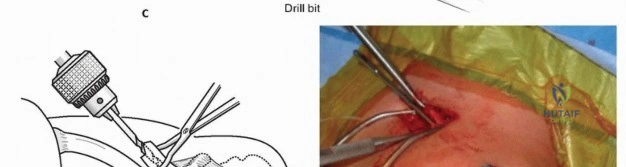
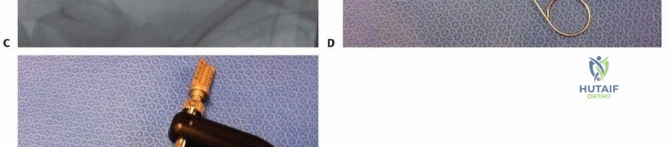
With the fracture ends cleanly exposed, attention turns to the preparation of the intramedullary canal. Using a specialized awl or a small drill bit, the medullary canal of the medial fragment is carefully opened. The trajectory must respect the anterior bow of the medial clavicle to avoid cortical perforation. A flexible guidewire or a dedicated hand reamer is then gently advanced into the medial canal to verify patency and determine the appropriate implant diameter. This process is subsequently repeated for the lateral fragment. The lateral canal is often narrower and flatter, requiring precise, controlled reaming to accommodate the distal aspect of the implant without compromising the thin superior or inferior cortices. Fluoroscopy is utilized extensively during this phase to ensure the instruments remain strictly within the medullary confines and do not breach the posterior cortex, which lies in dangerous proximity to the subclavian vessels.
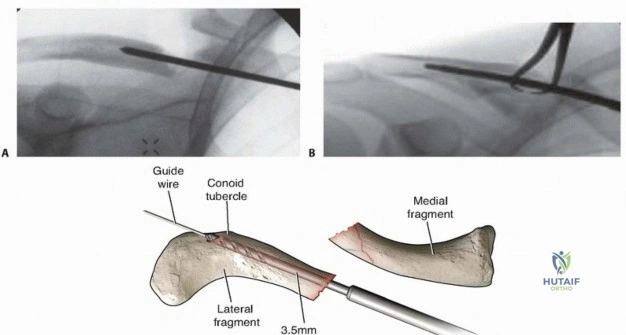
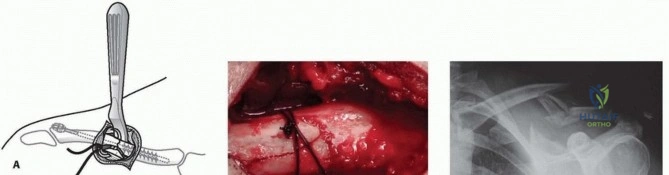
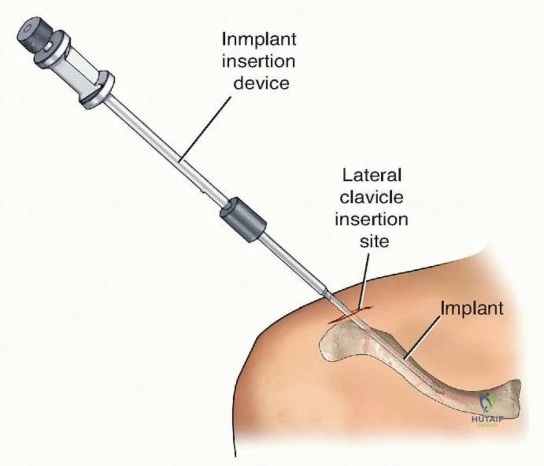
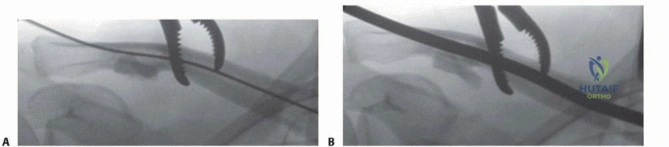
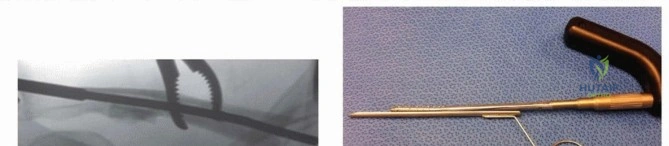
Once both canals are adequately prepared and sized, the definitive intramedullary device is introduced. Modern systems often utilize a device that is inserted into the medial fragment first. The implant is advanced until its medial locking mechanism (often an expandable gripper or a pre-contoured curve) is optimally positioned within the dense trabecular bone of the medial clavicle. The fracture is then anatomically reduced. This is achieved by applying lateral traction and extension to the operative arm (utilizing the sterile arm holder) while simultaneously manipulating the lateral fragment with a pointed reduction forceps to align it with the protruding implant. Once perfect cortical alignment is achieved, the lateral fragment is railroaded over the implant. The fracture is then dynamically compressed. Finally, the lateral aspect of the implant is rigidly secured, typically via a lateral locking screw inserted through a small percutaneous stab incision, passing through the lateral cortex and into the implant. This crucial lateral locking step completely neutralizes rotational instability and definitively prevents the catastrophic pin migration that plagued historical smooth intramedullary pins.
Complications, Incidence Rates, and Salvage Management
Despite the refined techniques and advanced biomechanical designs of modern intramedullary devices, operative fixation of the midshaft clavicle is not devoid of complications. Historically, the most feared and devastating complication of IM fixation was the unconstrained migration of smooth pins (such as Hagie or Knowles pins) into the thoracic cavity, potentially causing fatal cardiac or pulmonary puncture. However, with the advent of contemporary locked intramedullary nails featuring expandable medial grippers and lateral interlocking screws, the incidence of catastrophic implant migration has been reduced to near zero. Today, the most frequently encountered complications are implant prominence, hardware failure (breakage), and nonunion. Because the lateral clavicle is exceptionally subcutaneous, the lateral locking screw or
Clinical & Radiographic Imaging Archive