Pediatric Hip Fractures: An Intraoperative Masterclass in Reduction and Fixation
Key Takeaway
Join us in the operating theater for an immersive masterclass on pediatric hip fractures. We'll meticulously cover surgical anatomy, preoperative planning, and step-by-step intraoperative execution for both closed and open reduction with various fixation methods. Learn to navigate complex cases, manage potential pitfalls, and optimize postoperative care for these challenging injuries, ensuring the best outcomes for our young patients.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a masterclass on one of the most critical, unforgiving, and technically demanding injuries in the pediatric population: the pediatric hip fracture. Representing less than 1% of all pediatric fractures, these injuries are exceedingly rare, yet they command our utmost respect due to their profound potential for devastating long-term morbidity. Unlike the geriatric hip fractures we encounter daily—which are typically fragility fractures resulting from low-energy ground-level falls—pediatric hip fractures are almost exclusively the result of massive, high-energy trauma. Motor vehicle collisions, pedestrian-struck incidents, and falls from significant heights impart tremendous axial and shear forces across the immature proximal femur, necessitating a rigorous and urgent orthopedic response.
The fundamental challenge in managing pediatric hip fractures lies in the unique, evolving anatomy of the immature hip and its notoriously precarious blood supply. The presence of open physes complicates both the injury pattern and our fixation strategies. Our overarching goal is uncompromising: achieve an anatomic reduction, provide absolute stable fixation, decompress the hip capsule, and meticulously preserve the capital femoral epiphysis to ensure optimal healing and continued longitudinal growth. Failure to achieve these tenets dramatically increases the risk of avascular necrosis (AVN), coxa vara, premature physeal closure, and nonunion, ultimately condemning a child to a lifetime of hip dysfunction, early-onset osteoarthritis, and the potential need for multiple reconstructive surgeries or early arthroplasty.

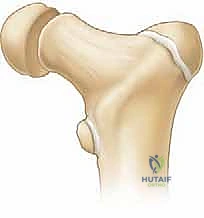
Understanding the patho-epidemiology requires an appreciation of the Delbet classification system, which remains the universally accepted framework for categorizing these injuries and predicting their prognosis. The classification is strictly anatomical, dividing fractures into Type I (transepiphyseal separations), Type II (transcervical fractures), Type III (cervicotrochanteric fractures), and Type IV (intertrochanteric fractures). The risk of AVN is directly proportional to the proximity of the fracture to the femoral head, with Type I and Type II fractures carrying the highest rates of ischemic complications. As orthopedic surgeons, we must approach these fractures not merely as broken bones, but as acute vascular emergencies of the proximal femur.
Detailed Surgical Anatomy and Biomechanics
To master the surgical management of pediatric hip fractures, one must possess an intimate, three-dimensional understanding of the proximal femoral osteology, its capsular attachments, and, most importantly, its evolving vascular network. The pediatric hip is a marvel of developmental biology, but its growth plates and vascularity render it uniquely vulnerable to trauma and iatrogenic injury.
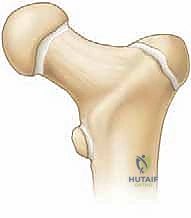
Proximal Femur Osteology and the Physis
The proximal femur in a child is characterized by the presence of the capital femoral epiphysis, the subcapital physis (proximal femoral physis), and the apophyses of the greater and lesser trochanters. The femoral neck typically forms a neck-shaft angle of approximately 135 degrees, an angle that is crucial for normal hip biomechanics, abductor lever arm function, and load transmission. Crucially, the medial two-thirds of the femoral neck are entirely intracapsular, while the lateral one-third is extracapsular. This anatomical distinction dictates the healing potential of the fracture; intracapsular fractures lack a robust periosteal envelope, relying almost entirely on endosteal healing, which is frequently compromised by the fracture itself.
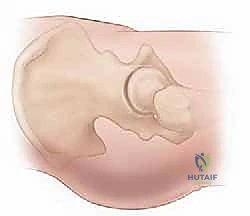
The capital femoral physis is not merely a growth plate; it is a mechanical weak point and a barrier to vascular anastomosis. As the child ages, the contour of the physis changes from relatively flat to mammillary, increasing its resistance to shear forces. However, under the massive loads of a high-energy impact, this physis can separate (Delbet Type I), often accompanied by a dislocation of the epiphysis from the acetabulum, representing the most severe form of this injury.
Vascular Supply: The Lifeline of the Femoral Head
The blood supply to the pediatric femoral head is the single most critical anatomical consideration in these fractures. Unlike adults, where intraosseous cervical vessels contribute significantly, the pediatric femoral head relies almost exclusively on the extraosseous retinacular vessels. These vessels, primarily the posterosuperior and posteroinferior retinacular arteries, are terminal branches of the medial circumflex femoral artery (MCFA). They ascend along the femoral neck within the synovial folds (retinacula) and pierce the epiphysis at the capsular reflection.

During childhood, the physis acts as an impenetrable barrier to blood vessels; therefore, the metaphyseal blood supply cannot cross into the epiphysis. Furthermore, the contribution of the artery of the ligamentum teres is negligible until the child is around 8 to 10 years old. Consequently, any fracture that displaces the femoral neck (Delbet Types I, II, and III) will stretch, kink, or tear these delicate retinacular vessels. Additionally, an intracapsular hematoma can create a tamponade effect, raising intracapsular pressure above the capillary perfusion pressure of the retinacular vessels, further exacerbating ischemia. This is the physiological rationale for emergent capsulotomy.
Muscular Intervals and Biomechanical Forces
Surgically, we must navigate the muscular intervals carefully. Anteriorly, the femoral triangle houses the femoral neurovascular bundle, dictating caution during the Smith-Petersen approach. Laterally, the interval between the tensor fasciae latae (TFL) and the gluteus medius (Watson-Jones approach) provides excellent access to the femoral neck while respecting the neurovascular planes. Biomechanically, the proximal femur is subjected to massive deforming forces. The abductors (gluteus medius and minimus) pull the greater trochanter proximally, while the iliopsoas pulls the lesser trochanter proximally and anteriorly. These forces inevitably lead to varus collapse, shortening, and external rotation of the distal fragment, necessitating forceful but controlled reduction maneuvers and rigid internal fixation to counteract these vectors during healing.
Exhaustive Indications and Contraindications
The threshold for operative intervention in pediatric hip fractures is exceedingly low. Given the catastrophic consequences of displacement, malunion, and AVN, almost all pediatric hip fractures warrant surgical stabilization. Non-operative management is historically fraught with unacceptable rates of coxa vara and nonunion, largely due to the inability of a spica cast to counteract the powerful deforming muscle forces across the hip joint.
Operative Indications
Operative fixation is absolutely indicated for all displaced Delbet Type I, II, III, and IV fractures. The primary objective is to achieve an anatomic, non-traumatic reduction to restore the continuity of any remaining retinacular vessels and to provide rigid stability to facilitate revascularization and bone healing. Furthermore, even undisplaced Delbet Type I, II, and III fractures are generally treated with prophylactic in-situ fixation. The rationale is simple: the risk of secondary displacement in a cast is significant, and the penalty for that displacement—namely, vascular disruption and subsequent AVN—is too high to accept.

Urgent decompression of the hip joint via capsulotomy or arthrocentesis is a critical adjunct indication for all intracapsular fractures. While debate exists regarding the exact timing, the prevailing consensus in academic pediatric orthopedics is that these injuries should be treated as surgical emergencies, ideally addressed within 24 hours of injury, to minimize the duration of vascular compromise.
Contraindications
Absolute contraindications to surgical fixation are exceedingly rare and are generally limited to patients who are medically unstable and unable to tolerate anesthesia due to concomitant life-threatening injuries (e.g., severe traumatic brain injury or massive solid organ hemorrhage). In such extremis, temporary skeletal traction may be employed until the patient is physiologically optimized. Relative contraindications may include severe, pre-existing neuromuscular disease where the functional baseline is non-ambulatory, though even in these cases, fixation is often pursued for pain control and nursing care.
| Delbet Classification | Anatomical Description | Operative Indication | Preferred Fixation Strategy |
|---|---|---|---|
| Type I | Transepiphyseal separation (with or without dislocation) | Absolute (Emergent) | Open reduction, capsulotomy, smooth K-wires or partially threaded screws (physeal-sparing if possible, transphyseal if necessary for stability). |
| Type II | Transcervical fracture (most common) | Absolute | Closed vs. Open reduction, capsulotomy, cannulated screws or pediatric hip plate. Avoid physis if space permits. |
| Type III | Cervicotrochanteric fracture | Absolute | Closed reduction, cannulated screws or pediatric dynamic hip screw (DHS) / locking plate. |
| Type IV | Intertrochanteric fracture | Absolute | Closed reduction, pediatric DHS, locking proximal femoral plate, or flexible intramedullary nails (depending on age). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a successful outcome in pediatric hip trauma. The margin for error is razor-thin; misplaced hardware can cause iatrogenic physeal arrest, while inadequate reduction guarantees biomechanical failure.
Advanced Imaging and Templating
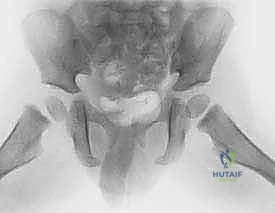
Initial evaluation mandates high-quality, orthogonal plain radiographs: an anteroposterior (AP) view of the pelvis and a cross-table lateral view of the affected hip. Frog-leg lateral views should be avoided in displaced fractures as the maneuver can exacerbate vascular injury. While plain films are diagnostic, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is invaluable, particularly for Delbet Type II and III fractures, to assess the degree of comminution, the exact plane of the fracture, and the available bone stock in the femoral neck for screw purchase.
Magnetic Resonance Imaging (MRI) has a limited role in the acute setting. While it can theoretically assess epiphyseal perfusion, obtaining an MRI delays definitive surgical reduction and capsulotomy, which is counterproductive. Preoperative digital templating is mandatory. The surgeon must measure the width of the femoral neck and the distance from the fracture line to the physis to select the appropriate screw diameter (typically 4.0mm to 6.5mm depending on the child's age) and to determine if physeal-sparing fixation is anatomically feasible.
Operating Room Setup and Patient Positioning
The patient is brought to the operating room and placed supine on a fully radiolucent carbon-fiber Jackson table or a standard flat table. The use of a specialized fracture table with boots is highly controversial in pediatric patients. While it aids in traction, it can easily apply excessive, uncontrolled force across open physes (knee and ankle), risking iatrogenic injury. Furthermore, the perineal post can act as a fulcrum, causing pudendal nerve palsy or soft tissue necrosis in a small child. Therefore, manual traction on a flat radiolucent table is the preferred method for most academic pediatric orthopedic surgeons.


The C-arm fluoroscopy unit is positioned on the contralateral side of the injury, draped sterilely. The monitor must be in direct line of sight for the primary surgeon. The patient's affected limb is prepped and draped free to allow for dynamic manipulation. For fluoroscopic imaging, the AP view is obtained by positioning the C-arm over the hip with the leg in neutral to slight internal rotation (to profile the femoral neck). For the lateral view, because the leg is draped free, the surgeon can gently elevate the leg and roll the C-arm under the table to obtain a true cross-table lateral, or carefully position the limb into a modified frog-lateral if the fracture is already provisionally stabilized.


Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be precise, deliberate, and respectful of the fragile biology. We will detail the approach for a displaced Delbet Type II transcervical fracture, the most common and arguably the most technically demanding pattern.
Reduction Maneuvers
The procedure begins with an attempt at gentle, closed reduction under live fluoroscopy. The classic Leadbetter maneuver is often employed: the hip is flexed to 90 degrees with slight adduction to disimpact the fragments, followed by longitudinal traction. While maintaining traction, the hip is slowly internally rotated, abducted, and extended. This maneuver utilizes the intact anterior capsule to pull the distal fragment into alignment with the proximal fragment.

If anatomic reduction cannot be achieved after one or two gentle attempts, closed reduction must be abandoned immediately. Repeated, forceful manipulation will invariably destroy any remaining intact retinacular vessels. We then proceed directly to an open reduction.
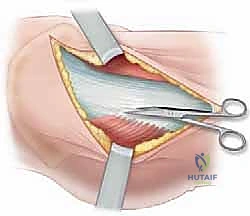
The Open Approach and Capsulotomy
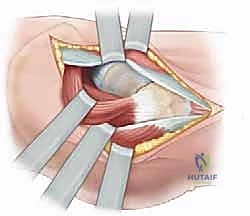
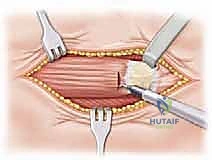
An anterolateral Watson-Jones approach is the workhorse for this procedure. A longitudinal incision is made over the lateral aspect of the greater trochanter, curving slightly anteriorly. The fascia lata is incised in line with the skin incision. The interval between the tensor fasciae latae (anteriorly) and the gluteus medius (posteriorly) is identified and bluntly developed.
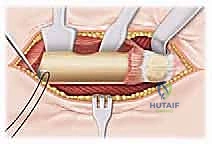

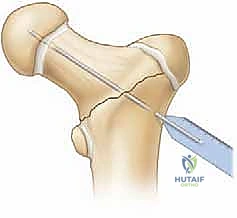
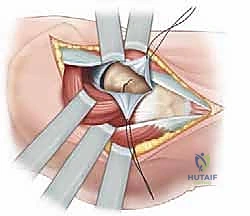
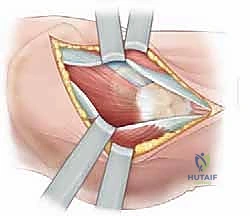
Deep to this interval, the anterior capsule of the hip joint is exposed. A T-shaped or I-shaped capsulotomy is performed. This is a critical step: upon incising the capsule, a significant hematoma is almost always evacuated, immediately decompressing the joint and theoretically restoring perfusion pressure to the retinacular vessels. The capsulotomy also allows direct visualization of the fracture site. Using a periosteal elevator or a small bone hook, the fracture fragments are gently manipulated into an anatomic reduction. Provisional fixation is achieved using multiple smooth Kirschner wires (K-wires) passed from the lateral cortex, across the fracture site, and into the femoral head.

Definitive Fixation Strategies
The choice of definitive implant depends heavily on the child's age and the amount of available bone in the proximal fragment.
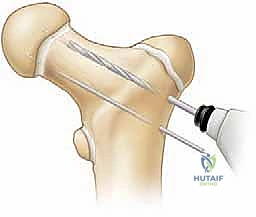
For children under 3 to 4 years of age, the femoral neck is largely cartilaginous. In these toddlers, fixation is best achieved using multiple smooth K-wires or partially threaded 4.0mm cancellous screws. The hardware must cross the physis to achieve adequate purchase in the epiphysis, as the neck is too small. While transphyseal fixation risks premature closure, the risk of nonunion or displacement without it is far greater.

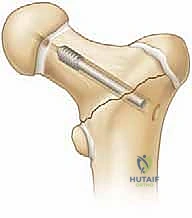
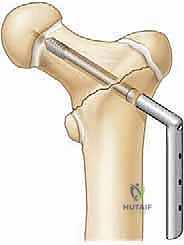
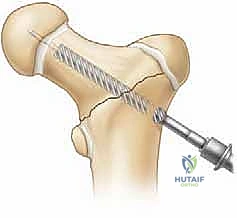
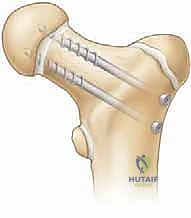
For older children and adolescents, cannulated screws (typically 4.5mm, 6.5mm, or 7.3mm depending on size) are the gold standard. The guide pins are placed over the provisional K-wires. Ideally, we aim for a three-screw construct in an inverted triangle configuration to maximize biomechanical stability against torsional and shear forces.


The crucial intraoperative decision is whether to cross the physis. If the fracture is a low transcervical or basicervical pattern, and there is sufficient room to place at least two (preferably three) screws short of the physis while still obtaining solid compression, physeal-sparing fixation is mandated. However, if the fracture is high (subcapital) and physeal-sparing screws would only engage a few millimeters of bone, the surgeon must cross the physis into the center of the epiphysis to prevent catastrophic fixation failure. Stability trumps physeal preservation in these high-energy injuries.
For Delbet Type III and IV fractures, a pediatric dynamic hip screw (DHS) or a proximal femoral locking plate provides superior biomechanical control of the cervicotrochanteric region, preventing the varus collapse that is common with isolated screw fixation in this area.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, complications in pediatric hip fractures are distressingly common, primarily dictated by the initial energy of the injury and the resulting vascular insult. The surgeon must counsel the family extensively regarding these risks prior to surgery.
Avascular Necrosis (AVN)
AVN is the most dreaded complication, occurring in up to 40-50% of Delbet Type I fractures, 25-30% of Type II, and 10-15% of Type III. It is classified using the Ratliff system: Type 1 involves the entire femoral head (worst prognosis), Type 2 involves only the anterolateral portion, and Type 3 involves the femoral neck leaving the head viable. AVN typically presents radiographically 6 to 12 months post-injury with sclerosis, fragmentation, and eventual collapse of the femoral head.
Management of AVN is complex and often salvage in nature. Early stages may be treated with prolonged non-weight bearing or articulated hinged braces, though efficacy is debated. Once collapse occurs, containment osteotomies (proximal femoral varus osteotomy or pelvic osteotomies) may be required to maintain sphericity. In severe cases with complete head destruction, arthrodesis or early total hip arthroplasty (THA) becomes inevitable.
Coxa Vara and Premature Physeal Closure
Coxa vara (a neck-shaft angle of less than 120 degrees) occurs due to loss of reduction, inadequate fixation, or asymmetric physeal arrest. It leads to a Trendelenburg gait, limb length discrepancy, and abductor weakness. It is most commonly seen in Delbet Type III and IV fractures treated without a fixed-angle device. Treatment requires a subtrochanteric valgus-producing osteotomy to restore normal biomechanics.
Premature physeal closure occurs in up to 30% of cases, either secondary to the trauma itself, ischemic insult, or iatrogenic hardware placement across the physis. This results in limb length discrepancy and potential articular incongruity. If the discrepancy is projected to be greater than 2-3 cm at maturity, contralateral epiphysiodesis or ipsilateral limb lengthening procedures are indicated.
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Options |
|---|---|---|---|
| Avascular Necrosis (AVN) | 10% - 50% (Type dependent) | Vascular disruption at injury, capsular tamponade | Containment osteotomies, core decompression, eventual THA. |
| **Coxa Vara |
Clinical & Radiographic Imaging Archive