Pediatric Tibial Fractures: An Operative Masterclass for Fellows
Key Takeaway
Welcome, fellows, to an immersive operative masterclass on pediatric tibial fractures. Today, we'll delve into the nuances of managing these common injuries, from comprehensive anatomical review and meticulous preoperative planning to the precise intraoperative execution of external fixation, plate fixation, and elastic intramedullary nailing. We'll navigate critical steps, highlight potential pitfalls, and discuss optimal postoperative care to ensure the best outcomes for our young patients.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are tackling a topic that is fundamental to the practice of pediatric orthopaedic surgery: the management of pediatric tibial fractures. While a significant proportion of these injuries can be managed non-operatively with excellent outcomes, it is absolutely critical for the orthopaedic surgeon to master the indications, preoperative planning, and precise techniques for surgical intervention. Our goal in the operative management of these injuries is not merely the restoration of radiographic alignment; it is the restoration of function, the prevention of devastating long-term sequelae, and the absolute protection of growth potential in these young, dynamically developing limbs. You must approach each of these cases with a profound respect for the biology of the pediatric skeleton.
Pediatric tibial fractures are remarkably common, representing a significant portion of long bone fractures evaluated in pediatric trauma centers. The epidemiology of these fractures is distinctly bimodal. In the toddler and early childhood demographic, we frequently encounter low-energy, twisting mechanisms resulting in the classic, often non-displaced spiral or oblique "toddler's fracture" of the distal tibial diaphysis. Conversely, in the older child and adolescent population, we see a surge in high-energy trauma—motor vehicle collisions, sports injuries, and falls from height—resulting in complex, comminuted, and frequently open fracture patterns that demand sophisticated surgical stabilization. Understanding this epidemiologic distribution is the first step in anticipating the fracture pattern and formulating an appropriate treatment algorithm.
When evaluating any pediatric tibial fracture, several paramount patho-epidemiological considerations must immediately come to mind. First and foremost is the vigilance required to identify pathologic fractures. Always maintain a high index of suspicion for an underlying benign or malignant bone lesion. Fractures occurring through nonossifying fibromas, aneurysmal bone cysts, unicameral bone cysts, osteomyelitis, or osteosarcomas require a completely different diagnostic and therapeutic paradigm. A thorough radiographic evaluation for any atypical features—such as cortical thinning, periosteal reaction inconsistent with acute trauma, or a permeative lytic appearance—is non-negotiable. Furthermore, in any young child presenting with an unclear or inconsistent history of trauma, or if you encounter multiple fractures in varying stages of healing, non-accidental trauma (child abuse) must be suspected, documented, and thoroughly investigated according to strict institutional protocols.
Finally, the unique pathophysiology of the pediatric bone dictates our management strategies. The presence of open physes (growth plates) at the proximal and distal ends of the tibia fundamentally precludes standard adult treatment options, such as solid, reamed interlocked intramedullary nails, which would obliterate the physis and guarantee growth arrest or severe angular deformity. However, this same immature skeleton possesses remarkable remodeling potential. Young children can remodel significant degrees of angulation in the plane of joint motion (sagittal plane) and, to a lesser extent, in the coronal plane. Rotational deformities, however, remodel poorly at any age. This remodeling potential predictably diminishes as the child approaches skeletal maturity, making precise, anatomic reduction increasingly critical in the adolescent population.
Detailed Surgical Anatomy and Biomechanics
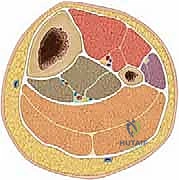
Before we ever lift a scalpel or position a fluoroscopy unit, we must refresh our exhaustive understanding of the tibial anatomy, focusing intensely on structures at risk, biomechanical properties, and key surgical landmarks. The pediatric tibia is not merely a smaller version of the adult tibia; it is a biomechanically distinct structure enveloped by a robust, osteogenic periosteum and capped by highly active growth centers. The cross-sectional anatomy of the tibial diaphysis is roughly triangular, a critical geometric fact when planning external fixator pin placement or plate application. A laterally aimed half-pin may only engage the vertically oriented lateral cortex, leading to unicortical fixation, catastrophic construct instability, and eventual pin pull-out.
The lower extremity is rigidly divided into four distinct fascial compartments, each bound by inelastic fascial septa and containing specific muscles, nerves, and vessels. An intimate knowledge of these compartments is your primary defense against the devastating consequences of missed compartment syndrome. The Anterior Compartment houses the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius, supplied by the anterior tibial artery and innervated by the deep peroneal nerve. The Lateral Compartment contains the peroneus longus and brevis, with the superficial peroneal nerve coursing through it before piercing the fascia distally. The Superficial Posterior Compartment holds the powerful gastrocnemius, soleus, and plantaris muscles. Crucially, the Deep Posterior Compartment contains the tibialis posterior, flexor digitorum longus, and flexor hallucis longus, along with the posterior tibial artery, peroneal artery, and the tibial nerve.
Beyond compartment-specific risks, the overall vascular tree presents unique hazards during tibial trauma and its subsequent surgical management. The popliteal artery bifurcates at the proximal border of the interosseous membrane. The anterior tibial artery abruptly penetrates this membrane to enter the anterior compartment. This specific anatomical tethering point makes the anterior tibial artery exquisitely vulnerable to traction, intimal tearing, or complete transection in high-energy proximal third tibial fractures. Similarly, the posterior tibial artery and tibial nerve are at risk during deep posterior compartment swelling or aggressive surgical retraction. You must respect these neurovascular bundles during every step of your dissection and hardware placement.
Understanding the osteology and the behavior of the physes is paramount for avoiding iatrogenic growth disturbance. The proximal tibial physis is a massive, undulating growth plate responsible for a significant portion of lower extremity longitudinal growth. Crucially, the anterior aspect of this physis extends distally to incorporate the tibial tubercle. Iatrogenic injury to the tibial tubercle physis—often via misplaced proximal pins or aggressive dissection—can lead to a premature anterior growth arrest, resulting in a devastating recurvatum deformity (hyperextension of the knee) as the posterior physis continues to grow. The perichondral ring of LaCroix and the groove of Ranvier, which provide structural support and latitudinal growth to the physis, must also be meticulously protected during any metaphyseal or epiphyseal instrumentation.
Exhaustive Indications and Contraindications
The decision to transition from non-operative casting to surgical intervention in a pediatric tibial fracture requires a nuanced understanding of acceptable alignment parameters, fracture personality, and patient-specific factors. While closed reduction and long-leg casting remains the gold standard for the vast majority of isolated, closed, low-energy pediatric tibial shaft fractures, there are strict thresholds where surgical stabilization becomes mandatory to prevent malunion and functional deficit.
Table 1: Acceptable Deformity for Pediatric Tibial Fractures by Age
| Radiographic Parameter | Under 8 Years Old | 8 Years to Skeletal Maturity |
|---|---|---|
| Coronal Plane (Varus/Valgus) | Up to 10 degrees | Up to 5 degrees |
| Sagittal Plane (Procurvatum/Recurvatum) | Up to 10 degrees | Up to 5 degrees |
| Shortening | Up to 10 mm | Up to 5 mm |
| Malrotation | Up to 5 degrees | Up to 5 degrees |
| Translation | Up to 50% | Up to 25% |
Note: These are guidelines; clinical judgment, fracture location (proximal vs. distal), and the trajectory of healing must always supersede rigid numerical cutoffs.
Absolute and Relative Indications
Absolute indications for surgical intervention include open fractures requiring thorough irrigation and debridement, fractures associated with an impending or established compartment syndrome requiring fasciotomy, and fractures with an associated vascular injury necessitating repair. The "floating knee" scenario—an ipsilateral fracture of the femur and tibia—is a strong indication for surgical stabilization of at least one, and typically both, fractures to allow for mobilization and prevent severe joint stiffness. Polytraumatized children also benefit immensely from early surgical stabilization of tibial fractures to facilitate nursing care, upright positioning, and pulmonary toilet.
Relative indications revolve around the inability to achieve or maintain acceptable radiographic alignment as outlined in Table 1. If a fracture falls outside these parameters after a high-quality closed reduction, or if it loses reduction during the first two to three weeks of cast immobilization, surgical fixation is warranted. Furthermore, as children approach skeletal maturity (typically girls >12 years, boys >14 years), their remodeling potential drops precipitously. In these older adolescents, the indications for surgery closely mirror adult parameters, and we have a much lower threshold to intervene for any significant displacement or shortening.
Contraindications to Surgery
Contraindications to operative intervention are relatively few but critical to recognize. Absolute contraindications include active, untreated deep infection at the planned surgical site (unless the surgery is for debridement and external fixation) and severe medical comorbidities that render the patient unfit for general anesthesia, such as profound cardiopulmonary instability in the acute polytrauma setting. In such extreme cases, rapid application of a splint or a simple spanning external fixator under local anesthesia may be the only viable, life-saving option until the patient is resuscitated. Relative contraindications include massive soft tissue compromise (e.g., severe degloving or blistering) that would make internal fixation unacceptably risky for wound breakdown and deep infection; in these scenarios, external fixation is the treatment of choice.
Pre-Operative Planning, Templating, and Patient Positioning
Every successful surgical case is won or lost long before the patient is wheeled into the operating room. For pediatric tibial fractures, meticulous preoperative assessment, precise templating, and flawless patient positioning are non-negotiable prerequisites. The process begins with a comprehensive history and physical examination, strictly adhering to Advanced Trauma Life Support (ATLS) protocols for high-energy mechanisms.
Clinical Evaluation and Compartment Syndrome Vigilance
The physical examination must focus heavily on the soft tissue envelope and a rigorous neurologic and vascular assessment. Compartment syndrome vigilance is arguably the most critical aspect of your preoperative evaluation. You must actively seek out the early signs: increasing pain, or pain entirely out of proportion to the apparent injury, is the earliest and most reliable warning. Tense, woody swelling of the compartments, extreme pain with gentle squeezing of the muscle bellies, and excruciating pain with passive stretch of the toes (e.g., passive toe flexion stressing the anterior compartment) are highly indicative. Do not wait for late signs like paresthesias, pallor, or pulselessness; loss of a pulse is an ominous, late finding indicating that irreversible ischemic necrosis may have already occurred. If there is any clinical suspicion, immediately split all casting and padding down to the skin. Have a low threshold for utilizing a solid-state transducer to measure compartment pressures; a delta pressure (diastolic blood pressure minus compartment pressure) of less than 30 mmHg is a definitive indication for emergent four-compartment fasciotomy.
Radiographic Templating
Standard radiographic evaluation mandates high-quality, orthogonal anteroposterior (AP) and lateral views of the entire tibia and fibula, including the knee and ankle joints. In cases of severe comminution or bone loss, full-length radiographs of the contralateral, uninjured limb are invaluable for templating. This allows you to accurately determine the native length of the tibia and select the appropriate size for implants, particularly when planning for flexible intramedullary nails or submuscular plates. If standard radiographs leave any ambiguity regarding physeal extension or intra-articular involvement (especially in transitional fractures like the Tillaux or Triplane variants), a computed tomography (CT) scan with sagittal and coronal reconstructions is mandatory to map the fracture lines and plan screw trajectories.
Operating Room Setup and Patient Positioning
Proper positioning is the foundation of a smooth procedure. The patient is placed supine on a radiolucent operating table. A critical maneuver is placing a small towel roll or bump underneath the ipsilateral hip. The pediatric femur naturally rests in external rotation; the hip bump counters this, allowing the patella to point directly anteriorly (straight vertically towards the ceiling). This ensures the entire limb is in a neutral rotational alignment, which is absolutely crucial for judging clinical alignment during reduction and hardware placement.

The fluoroscopy machine (C-arm) must be positioned optimally. Bring the C-arm in from the contralateral side of the operating table, opposite the surgeon. This keeps the bulky base of the machine out of your surgical field and allows unimpeded access to the injured limb for reduction maneuvers and instrument manipulation. Ensure the monitor is placed in your direct line of sight.

A tourniquet should be applied high on the thigh over adequate padding. However, we do not routinely inflate it at the start of the case. We reserve tourniquet inflation for situations where excessive, uncontrollable bleeding obscures the surgical field during an open approach, or if we anticipate massive blood loss. Routine inflation can mask the assessment of tissue viability and distal perfusion during the procedure.

Step-by-Step Surgical Approach and Fixation Technique
We have several operative techniques at our disposal, each tailored to the specific fracture personality, the age of the patient, and the status of the soft tissue envelope. We will comprehensively cover External Fixation, Elastic Stable Intramedullary Nailing (ESIN), and Submuscular Plating.
A. External Fixation Technique
External fixation is the workhorse for open fractures with severe soft tissue compromise, highly comminuted diaphyseal fractures, and damage control orthopaedics in the unstable polytrauma patient. It is also an excellent tool for managing late loss of reduction where an open approach is required to take down early callus.

1. Pin Placement and Safe Zones:
Following initial closed reduction via longitudinal traction, pin placement begins. All pins must be placed through small, sharp stab incisions, followed by blunt dissection down to the bone using a hemostat to spread the soft tissues. This protects cutaneous nerves and prevents soft tissue necrosis around the pin. Every single pin must be placed under continuous fluoroscopic guidance.

The proximal pins are the most critical. The starting point should be on the anteromedial face of the tibia. You must stay strictly distal to the proximal tibial physis and the distal extent of the tibial tubercle apophysis. Use a drill sleeve to protect the soft tissues. Pre-drill both cortices with the appropriate sized bit, and insert the half-pins manually to ensure excellent cortical purchase and "feel."

2. Distal Pin Placement and Frame Assembly:
Distal pins are typically placed from an anteromedial to posterolateral trajectory, again staying well proximal to the distal tibial physis. Once two pins are securely placed in both the proximal and distal fragments, the frame is assembled.
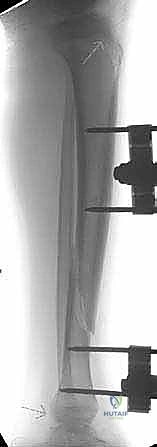
Carbon fiber rods and multi-pin clamps are utilized to build a rigid construct. We typically prefer a unilateral, uniplanar or biplanar frame for diaphyseal fractures. Final reduction is achieved by manipulating the pins and locking the clamps under live fluoroscopy, ensuring restoration of length, alignment, and rotation.

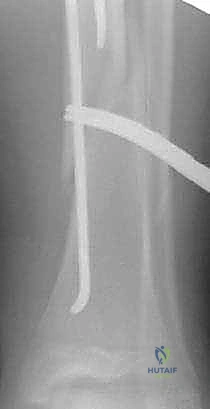
B. Elastic Stable Intramedullary Nailing (ESIN)
ESIN, or flexible nailing, is the absolute gold standard for the operative treatment of transverse, short oblique, or short spiral diaphyseal tibial fractures in children aged 5 to 12 years. It relies on the principle of three-point symmetric fixation within the medullary canal to provide relative stability, promoting rapid, robust secondary bone healing (callus formation).

1. Nail Selection and Contouring:
Preoperative measurement of the narrowest diameter of the medullary canal (the isthmus) is essential. The diameter of each of the two titanium nails should be approximately 40% of the narrowest canal diameter, ensuring they fill about 80% of the canal when inserted together. The nails must be pre-contoured into a gentle "C" shape. The apex of the curve should correspond to the fracture site to maximize the three-point bending forces against the inner cortices.

2. Entry Points and Insertion:
For the tibia, we utilize a proximal medial and proximal lateral entry point. Make small 2cm incisions over the medial and lateral metaphysis, approximately 2cm distal to the proximal tibial physis. Use an awl or drill to breach the near cortex, aiming distally at a 45-degree angle.

Insert the pre-contoured nails, one medial and one lateral. Advance them sequentially down the canal to the fracture site.

3. Fracture Negotiation and Final Seating:
Reduce the fracture closed. Using the T-handle, carefully rotate and advance the nails across the fracture site into the distal fragment.

The nails should be driven down to the distal metaphysis, stopping just short of the distal physis. Ensure the tips of the nails diverge (one medial, one lateral) to lock the distal fragment.

Finally, cut the proximal ends of the nails, leaving 1-2 cm protruding from the cortex to facilitate future removal, and gently bend them away from the bone to prevent skin irritation.
C. Submuscular Plating
When a fracture is too proximal or too distal for flexible nails to achieve adequate purchase, or if the fracture is highly comminuted and length unstable in an older child, submuscular plating is an elegant and highly effective solution.

This technique respects the biology of the fracture by avoiding a massive open exposure. A small incision is made proximally or distally, and an extra-periosteal, submuscular tunnel is created along the medial face of the tibia using a Cobb elevator. A pre-contoured locking compression plate (LCP) is slid down the tunnel across the fracture site. Reduction is achieved indirectly using traction and percutaneous clamps. The plate is then secured with locking screws proximally and distally, completely bypassing the fracture zone to act as an internal fixator. This preserves the fracture hematoma and the vital periosteal blood supply, leading to high rates of union.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, complications can and do occur in the operative management of pediatric tibial fractures. The surgeon must be prepared to recognize these early and execute appropriate salvage strategies.
Table 2: Common Complications, Incidence, and Management Strategies
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Compartment Syndrome | 3 - 9% | High-energy crush, severe swelling, tight casting. | Emergent 4-compartment fasciotomy. Do not delay. |
| Leg Length Discrepancy (Overgrowth) | 10 - 20% | Hyperemia stimulating the physes, common in ages 3-10. | Usually <1cm and clinically insignificant. If >2cm at maturity, epiphysiodesis of the contralateral limb. |
| Angular Deformity (Valgus/Recurvatum) | 5 - 15% | Asymmetric growth, premature tubercle arrest, poor initial reduction. | Observation if remodeling expected. Corrective osteotomy (e.g., opening wedge) for severe, symptomatic deformity near maturity. |
| Delayed Union / Nonunion | < 2% | Infection, severe soft tissue stripping, inadequate stability. | Rule out infection. Optimize biology (bone graft) and mechanics (exchange nailing, compression plating). |
| Pin Tract Infection (Ex-Fix) | 15 - 30% | Poor pin care, thermal necrosis during insertion. | Oral antibiotics, aggressive local pin care. Rarely requires pin removal or IV antibiotics unless deep osteomyelitis develops. |
Compartment syndrome remains the most feared acute complication. Its incidence is highest in proximal third fractures and those caused by high-energy crush mechanisms. If diagnosed, an emergent dual-incision, four-compartment fasciotomy is required. Delaying surgery to obtain formal compartment pressures when clinical signs are glaringly obvious is a medicolegal and clinical pitfall.
Leg length discrepancy is a unique pediatric complication. Unlike adults who typically shorten, children often experience a transient overgrowth of the fractured tibia due to fracture hyperemia stimulating the adjacent physes. This overgrowth averages 5-10mm and usually resolves or becomes clinically insignificant over time. However, true physeal arrest from iatrogenic injury (e.g., placing a screw across the physis) will lead to progressive shortening and angular deformity, requiring complex reconstruction with osteotomies or spatial frame lengthening.
Angular deformities, particularly valgus angulation, can occur as the fracture heals or as a result of asymmetric physeal stimulation. Recurvatum is specifically linked to damage to the proximal tibial tubercle apophysis. While some coronal plane deformities remodel, sagittal plane deformities (procurvatum/recurvatum) remodel poorly and may necessitate a corrective closing or opening wedge osteotomy once the child nears skeletal maturity if the deformity causes gait dysfunction or joint pain.
Phased Post-Operative Rehabilitation Protocols
The surgery does not end when the skin is closed; it ends when the child returns to the playground or the athletic field. A structured, phased rehabilitation protocol is essential to protect the fixation while preventing joint contractures and muscle atrophy.
Phase 1: Immediate Post-Operative (Weeks 0-3)
The primary goals in this phase are pain control, soft tissue healing, and protection of the fracture construct. Regardless of the fixation method (ESIN, Ex-Fix, or Plate), the limb is typically immobilized in a well-padded posterior splint or a bivalved long-leg cast to control the foot and ankle and prevent equinus contracture. The patient is made strictly Non-Weight Bearing (NWB) or Toe-Touch Weight Bearing (TTWB) with crutches or a walker. Elevation is critical to combat swelling.
Phase 2: Early Healing and Callus Formation (Weeks 3-6)
At the 3-to-4-week mark, clinical and radiographic evaluations are performed. If early bridging callus is visible on orthogonal radiographs, the long-leg cast or splint can often be transitioned to a short-leg cast or a removable Controlled Ankle Motion (CAM) boot. This is a critical juncture where active and active-assisted Range of Motion (ROM) of the knee and ankle must begin to prevent permanent stiffness. Weight-bearing status is cautiously advanced to Partial Weight Bearing (PWB), guided by patient comfort and radiographic progression.
Phase 3: Consolidation and Strengthening (Weeks 6-12)
By 6 to 8 weeks, robust secondary bone healing should be evident. For patients treated with ESIN or plates, the CAM boot is generally discontinued, and full weight-bearing is permitted. Physical therapy focuses heavily on restoring normal gait mechanics, rebuilding the atrophied quadriceps and calf musculature, and proprioceptive training. For patients in external fixators, frame removal is typically considered during this window once three out of four cortices show solid bridging bone.
Phase 4: Return to Sport (Months 3-6+)
Return to full contact sports or high-impact activities is not permitted until the fracture is completely obliterated on radiographs, the patient has full, painless range of motion of the knee and ankle, and the operative limb has regained at least 90% of the strength of the contralateral limb. Premature return to sport risks catastrophic re-fracture, particularly through stress risers at the ends of plates or at hardware removal sites. Hardware removal (such as extracting flexible nails) is typically scheduled electively 6 to 12 months post-injury, after complete consolidation.
Summary of Landmark Literature and Clinical Guidelines
To practice evidence-based pediatric orthopaedics, you must be intimately familiar with the landmark literature that dictates our current standard of care. The evolution of pediatric tibial fracture management has been heavily influenced by several key studies and societal guidelines.
The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines on the Management of Pediatric Diaphyseal Fractures strongly support the use of closed reduction and casting as the first-line treatment for the vast majority of closed tibial shaft fractures. However, they explicitly outline the indications for operative intervention, validating the use of ESIN as a highly effective, low-morbidity option for length-stable fractures in school-aged children.
The pioneering work by Flynn et al. established the definitive criteria for the use of titanium elastic nails, demonstrating superior outcomes
