

Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellow surgeons, to the operating theater. Today, we are undertaking a comprehensive masterclass on a fascinating, high-energy, and often technically demanding injury: the pectoralis major rupture. This intervention is not merely about reattaching a avulsed tendon; it is an intricate biomechanical reconstruction aimed at restoring formidable shoulder strength, dynamic stability, and cosmesis for our highly active, high-demand patient demographic. As we scrub in and prepare our surgical strategy, it is imperative to deeply understand the patho-epidemiology that drives these injuries and dictates our reconstructive approach.
The pectoralis major is one of the largest, most robust muscles of the shoulder girdle, serving as the primary engine for powerful adduction, forward flexion, and internal rotation of the humerus. Ruptures of this musculotendinous unit are relatively rare in the general population but have seen a dramatic exponential rise in incidence over the past three decades. This surge is almost exclusively correlated with the escalating popularity of high-intensity weightlifting, specifically the bench press, alongside participation in collision sports such as rugby, American football, and martial arts. The classic demographic is a muscular male between the ages of 20 and 40, often presenting after a catastrophic failure during a maximum-effort lift.
The pathomechanics of a pectoralis major rupture almost universally involve a massive eccentric load applied to a maximally contracted muscle. During the descent phase of a bench press, or when a patient violently attempts to break a fall, the humerus is forced into extension, abduction, and external rotation. This specific position disproportionately loads the inferior fibers of the sternocostal head. At approximately 30 degrees of humeral extension, these inferior fibers are stretched to their absolute physiological limit, placing them at a severe mechanical disadvantage. Consequently, they are typically the first to experience macroscopic failure. Once the sternocostal head yields, the load violently shifts to the clavicular head, often resulting in a catastrophic, propagating complete rupture of the entire complex.
We must also critically address the pharmacological elephant in the room: the use of anabolic-androgenic steroids (AAS). A significant percentage of patients presenting with acute pectoralis major ruptures have a history of AAS use. Exogenous androgens induce rapid, massive muscle hypertrophy that vastly outpaces the physiological adaptation of the corresponding tendon and its osseous insertion site. Furthermore, steroids can induce collagen dysplasia, decreasing the ultimate tensile strength and elastic modulus of the tendon. This creates a dangerous biomechanical mismatch—a hyper-powerful muscle engine pulling on a structurally compromised, stiffened tendon—making acute avulsion at the tendon-bone interface highly probable under extreme eccentric loading.
Detailed Surgical Anatomy and Biomechanics
Osteotendinous Architecture
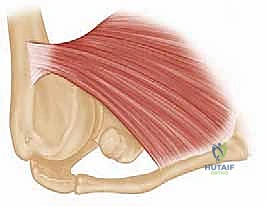
To execute a flawless anatomical repair, one must possess a three-dimensional mastery of the pectoralis major's unique architecture. The pectoralis major is a broad, fan-shaped, triangular muscle comprised of two distinct primary segments that converge onto a highly specific footprint on the proximal humerus. The clavicular head originates from the medial half of the anterior clavicle, while the much larger sternocostal head arises from the anterior sternum, the costal cartilages of the first six ribs, and the aponeurosis of the external oblique.
As these two muscle bellies transition laterally toward the humerus, they form a complex, bi-laminar tendon approximately 5 centimeters in length. The architecture of this insertion is an evolutionary marvel of biomechanical engineering. The tendon does not insert as a single flat sheet; rather, it twists upon itself. The clavicular head remains anterior and inserts distally along the lateral lip of the bicipital groove, forming a lamina roughly 1 centimeter in length.
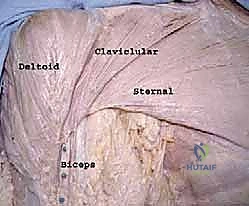
Conversely, the larger sternocostal head undergoes a dramatic 180-degree spiral. As it travels laterally, the inferior-most fibers of the sternocostal head twist upward and deep, ultimately inserting posterior and proximal to the clavicular head. This forms a longer lamina of approximately 2.5 centimeters. This unique spiraling mechanism is precisely what creates the characteristic, rounded inferior border of the anterior axillary fold. Understanding this twist is paramount during surgical reconstruction; simply tacking the tendon back to the bone without recreating this bi-laminar, spiraled footprint will result in altered biomechanics, persistent weakness, and a suboptimal cosmetic outcome.
Neurovascular Topography
Navigating the surgical approach requires meticulous respect for the surrounding neurovascular structures. The primary surgical corridor for a pectoralis major repair is the deltopectoral interval. This is a true internervous plane, bounded laterally by the deltoid muscle (innervated by the axillary nerve) and medially by the pectoralis major (innervated by the medial and lateral pectoral nerves). The sentinel landmark for this interval is the cephalic vein, which courses superficially within the groove. During our approach, the cephalic vein is typically preserved and retracted laterally with the deltoid to protect its delicate venous tributaries, though medial retraction is acceptable if the venous anatomy dictates.
The motor innervation to the pectoralis major is supplied by the medial and lateral pectoral nerves, which are named for their origins from the medial and lateral cords of the brachial plexus, respectively—not their anatomical position relative to the muscle. The medial pectoral nerve (C8, T1) pierces the pectoralis minor muscle and enters the deep, lateral surface of the sternocostal head. The lateral pectoral nerve (C5, C6, C7) courses medial to the coracoid process, pierces the clavipectoral fascia, and enters the deep surface of the clavicular head. While these nerves are generally safe during a standard distal tendon repair, aggressive medial mobilization of a chronically retracted muscle belly demands extreme caution to avoid devastating denervation.
Furthermore, the surgeon must remain cognizant of the axillary nerve and the local vascular supply. The axillary nerve (C5, C6) exits the quadrangular space and courses posteriorly around the surgical neck of the humerus. While it lies posterior to our primary field of dissection, straying deep to the conjoint tendon or drilling blindly across the humerus can place it at risk. The primary blood supply to the pectoralis major arises from the pectoral branch of the thoracoacromial artery. During the dissection, numerous muscular perforators will be encountered, particularly when mobilizing the muscle off the chest wall in chronic cases, necessitating precise bipolar electrocautery to maintain a bloodless field and prevent postoperative hematoma.
Clinical Evaluation and Diagnostic Imaging
Patient History and Physical Examination
A meticulous clinical evaluation is the cornerstone of an accurate diagnosis, as missed or delayed diagnoses of pectoralis major ruptures are unfortunately common in primary care settings. The patient's history will almost always feature a specific, high-energy inciting event. The classic narrative involves a heavy bench press or a sudden, forceful eccentric contraction (e.g., a waterskier holding the tow rope during a fall). Patients frequently report hearing an audible, distinct "pop" or feeling a tearing sensation across the anterior chest, immediately followed by severe, burning acute pain and profound weakness.
Physical examination in the acute phase is often complicated by significant guarding, swelling, and extensive ecchymosis that can track down the medial brachium, across the lateral chest wall, and into the axilla. However, once the initial acute swelling subsides—or if the patient is examined immediately post-injury—the pathognomonic sign is the loss of the normal anterior axillary fold contour. Medial retraction of the muscle belly is usually visible and becomes starkly apparent when the patient is asked to perform an isometric contraction. Palpation of the lateral chest wall will reveal a distinct, painful defect at the insertion site on the proximal humerus, and the surgeon may palpate a firm, bunched-up mass of retracted muscle medially.
Strength testing is critical for differentiating complete from partial tears and for isolating the involved heads. Resisted adduction, performed by having the patient press their palms together in front of their chest, will demonstrate profound weakness and vividly highlight the medial retraction of the sternocostal head. Resisted forward flexion at 90 degrees isolates and tests the integrity of the clavicular head. Resisted internal rotation will also demonstrate significant weakness compared to the contralateral side. It is also vital to test resisted abduction to ensure the deltoid is intact, ruling out a concurrent axillary nerve injury or deltoid avulsion.


Advanced Diagnostic Imaging
While the diagnosis of a pectoralis major rupture is primarily clinical, advanced diagnostic imaging is indispensable for precise preoperative planning. Standard plain radiographs of the shoulder (Anteroposterior, Scapular Y, and Axillary views) should always be obtained. While they rarely show the soft tissue injury, they are essential to rule out concurrent bony pathology, such as an anterior shoulder dislocation, a proximal humerus fracture, or a rare bony avulsion of the pectoralis insertion from the lateral lip of the bicipital groove. In chronic cases, radiographs may occasionally reveal heterotopic ossification at the site of the torn tendon.
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating pectoralis major injuries. A dedicated chest MRI or a specialized shoulder MRI with an expanded field of view encompassing the anterior chest wall is required. T2-weighted and Short Tau Inversion Recovery (STIR) sequences are particularly useful for identifying edema, hemorrhage, and the exact location of the tear. The MRI allows the surgeon to definitively categorize the injury: is it a complete avulsion at the tendon-bone interface, a tear at the musculotendinous junction, or a purely intramuscular tear? This distinction is critical, as true intramuscular tears are generally managed non-operatively, whereas tendon avulsions are prime candidates for surgical repair.
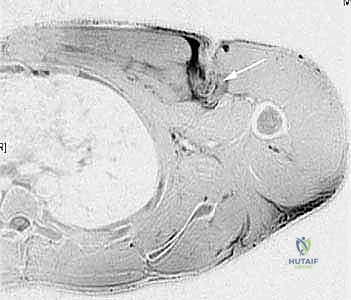

Furthermore, MRI provides invaluable information regarding the degree of medial retraction and the quality of the remaining tendon stump. In chronic cases, the MRI will reveal the extent of muscle atrophy and fatty infiltration, which are critical prognostic indicators for the success of a delayed reconstruction. While dynamic ultrasound can also be utilized to assess tendon continuity and retraction, its utility is highly operator-dependent. In the hands of an experienced musculoskeletal ultrasonographer, it can provide excellent real-time, dynamic assessment of the muscle, but MRI remains the definitive imaging modality of choice for surgical planning.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention versus conservative management hinges on a complex matrix of variables, including the patient's age, functional demands, chronicity of the injury, and the precise anatomical location of the tear. As orthopedic surgeons, our goal is to align the treatment strategy with the patient's physiological requirements and expectations. Non-operative management of complete distal tears inevitably leads to permanent cosmetic deformity and persistent functional deficits, specifically a 25% to 50% reduction in peak adduction and internal rotation strength. Therefore, in our active patient population, the threshold for surgical intervention is appropriately low.
Acute, complete ruptures at the tendon-bone interface or the distal musculotendinous junction in young, athletic, or high-demand occupational patients (e.g., military personnel, manual laborers, first responders) are absolute indications for surgical repair. Early operative intervention, ideally performed within the first 3 to 4 weeks post-injury, yields the most reliable outcomes. During this acute window, the tendon is relatively easy to mobilize, tissue quality is robust, and an anatomic, tension-free repair can be achieved without the need for complex allograft reconstruction.
The management of chronic tears (presenting >6 weeks post-injury) presents a significantly greater surgical challenge. Over time, the medially retracted muscle belly becomes encased in dense scar tissue, the tendon stump undergoes fibrotic degeneration, and the muscle itself may begin to show signs of atrophy. Despite these challenges, surgical reconstruction is still highly indicated in symptomatic patients who complain of unacceptable weakness, cramping, or cosmetic deformity. However, the surgeon must be prepared for extensive soft tissue mobilization and must have allograft tissue (such as Achilles tendon or semitendinosus) available on standby, as primary repair may be impossible due to severe retraction and loss of tendon length.
Conversely, non-operative management is reserved for a specific subset of patients. Intramuscular tears (muscle belly tears) have an excellent capacity for spontaneous healing and are almost universally treated conservatively with a brief period of immobilization followed by progressive rehabilitation. Partial tears in low-demand, elderly, or sedentary patients who are willing to accept mild to moderate strength deficits and cosmetic asymmetry are also managed non-operatively. Furthermore, patients with severe medical comorbidities that preclude safe anesthesia, or those who are non-compliant and unlikely to adhere to strict postoperative rehabilitation protocols, are generally contraindicated for surgical repair.
| Clinical Scenario | Recommendation | Rationale / Considerations |
|---|---|---|
| Acute Complete Tendon Avulsion (Active Patient) | Absolute Indication for Surgery | Restores peak adduction/internal rotation strength; prevents chronic retraction; resolves cosmetic deformity. Best outcomes if done < 4 weeks. |
| Acute Musculotendinous Junction Tear (High Demand) | Strong Indication for Surgery | High risk of persistent weakness if left untreated. Requires meticulous suturing techniques (e.g., Krackow) to capture muscle/tendon interface. |
| Chronic Retracted Tear (> 6 weeks) | Relative Indication for Surgery | Indicated for persistent weakness/cramping. Technically demanding; requires extensive mobilization; high likelihood of needing allograft augmentation. |
| Intramuscular (Muscle Belly) Tear | Contraindication to Surgery | High healing potential with conservative care. Sutures pull through friable muscle tissue; surgery risks further iatrogenic damage. |
| Elderly / Low-Demand Patient | Relative Contraindication | Patient may tolerate strength deficit well. Surgical risks (infection, anesthesia) may outweigh functional benefits. |
| Active Infection / Severe Comorbidities | Absolute Contraindication | Unacceptable risk of perioperative morbidity or hardware infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Anesthesia and Patient Positioning
Meticulous preoperative planning and optimal patient positioning are critical prerequisites for a smooth, efficient, and successful pectoralis major repair. The procedure is typically performed under general anesthesia. We highly recommend the addition of a regional interscalene nerve block, administered preoperatively by the anesthesia team. This provides excellent intraoperative muscle relaxation, which is vital for mobilizing the retracted tendon, and ensures profound postoperative analgesia, significantly reducing the requirement for systemic narcotics in the immediate recovery phase.
Positioning is a matter of surgeon preference, with both the beach-chair and supine positions being viable options. In our practice, we prefer a modified beach-chair position with the backrest elevated to approximately 30 to 45 degrees. This position allows for excellent visualization of the anterior chest wall and the deltopectoral interval, while also permitting gravity to assist in retracting the deltoid laterally. The operative arm is meticulously prepped and draped free to allow for full, unrestricted range of motion during the procedure. We utilize a sterile arm positioner (such as a Spider arm or a Mayo stand) to hold the arm securely in varying degrees of abduction and external rotation, which is essential for exposing the footprint and later for tensioning the repair.
Surgical Equipment and Templating
Prior to making the incision, the surgeon must ensure that all necessary specialized equipment is available in the operating theater. Pectoralis major repair requires robust fixation constructs capable of withstanding significant postoperative forces. The surgical tray should include heavy, non-absorbable sutures (e.g., #2 or #5 FiberWire or equivalent high-tensile strength tape), a variety of tendon grasping instruments (such as Allis or Babcock clamps), and specialized retractors (e.g., Gelpi, Weitlaner, and Richardson retractors).
Templating the fixation strategy is crucial. Depending on the surgeon's preferred technique and the quality of the host bone, the fixation may involve transosseous bone troughs, heavy-duty suture anchors (typically 5.5mm or larger, double or triple-loaded), or cortical button suspension devices. In acute cases, we favor a combined approach utilizing cortical buttons for strong unicortical or bicortical fixation, supplemented with suture anchors to compress the tendon footprint. If dealing with a chronic, retracted tear, the surgeon must absolutely ensure that appropriate allograft tissue (Achilles tendon with or without a bone block, or hamstring autograft/allograft) is thawed, prepped, and ready in the room before the incision is made, as the need for augmentation may only become apparent once the tendon stump is fully mobilized.
Step-by-Step Surgical Approach and Fixation Technique
The Deltopectoral Interval and Tendon Retrieval
The operation commences with a standard deltopectoral approach. A 5 to 8-centimeter longitudinal incision is made starting just inferior to the coracoid process and extending distally toward the axillary fold, following the natural skin cleavage lines. Subcutaneous dissection is carried down to the deltopectoral fascia. The cephalic vein is identified as the key landmark for the internervous interval between the deltoid and the pectoralis major. As previously noted, we generally prefer to retract the cephalic vein laterally with the deltoid muscle to preserve its delicate venous tributaries, though medial retraction is acceptable.

Once the interval is developed, the clavipectoral fascia is incised. In an acute setting, a large hematoma is typically encountered; this must be thoroughly evacuated and irrigated to visualize the underlying structures. The ruptured end of the pectoralis major tendon is usually found retracted medially. Using heavy Allis or Babcock clamps, the tendon edge is grasped. In acute injuries, the tendon is often easily mobilized laterally. However, in chronic cases, the muscle belly will be heavily scarred to the underlying chest wall, the conjoint tendon, and the pectoralis minor.
Extensive, meticulous blunt and sharp dissection is required to free the muscle. The surgeon must carefully sweep a finger deep to the pectoralis major muscle belly, releasing adhesions from the chest wall while strictly avoiding deep, blind dissection that could endanger the medial pectoral nerve or the underlying vascular structures. The goal is to achieve sufficient excursion so that the tendon stump can be pulled laterally to its anatomic insertion site on the humerus without excessive, unyielding tension.
Footprint Preparation and Tendon Mobilization
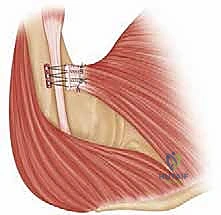
Simultaneous to tendon mobilization, the anatomic footprint on the humerus must be prepared. The insertion site is located on the lateral lip of the bicipital groove, extending distally from the inferior border of the subscapularis insertion. The long head of the biceps tendon serves as an excellent medial landmark; the repair must be placed strictly lateral to the groove to avoid tethering the biceps or causing postoperative tenosynovitis.

Using a combination of electrocautery, a periosteal elevator, and a motorized burr or rasp, the soft tissue remnants are cleared from the lateral lip of the bicipital groove. The cortical bone is lightly decorticated to expose a bleeding, cancellous bed. This bleeding bone surface is absolutely critical for promoting robust biological healing and integration of the tendon back into the osseous footprint. Care must be taken not to over-resect the bone, as the proximal humerus cortex can be surprisingly thin, and a strong bony bridge is required to support the subsequent fixation implants.
Biomechanical Fixation Techniques
Once the tendon is mobilized and the footprint is prepared, the tendon stump is meticulously prepared with heavy, non-absorbable sutures. We prefer a running, locked Krackow or whipstitch technique utilizing #2 or #5 high-tensile strength sutures or suture tape. At least two, and often three, separate grasping stitches are placed into the superior, middle, and inferior portions of the tendon stump. It is vital to ensure these stitches purchase a substantial amount of healthy, fibrous tendon tissue to prevent pull-through during tensioning.
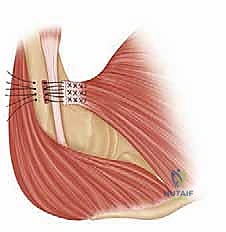
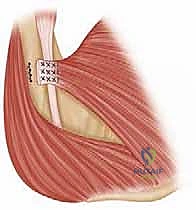
For the osseous fixation, several biomechanically validated techniques exist. The traditional "gold standard" involves creating a bone trough lateral to the bicipital groove and passing the sutures through drill holes (transosseous repair). However, modern techniques increasingly utilize strong metallic or PEEK suture anchors, or cortical button suspension devices. In our masterclass approach, we frequently utilize a hybrid technique. We drill unicortical or bicortical holes and shuttle the sutures through cortical buttons that rest on the posterior cortex of the humerus. This provides massive pull-out strength.
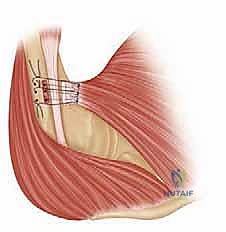
The arm is then positioned in approximately 30 degrees of abduction and 30 degrees of internal rotation to remove tension from the repair site. The sutures are systematically tied, firmly docking the tendon onto the decorticated footprint. We pay special attention to recreating the anatomic, bi-laminar insertion, ensuring the inferior fibers (sternocostal head) are secured properly to recreate the axillary fold. Additional suture anchors may be placed to compress the tendon edge flat against the bone, maximizing the surface area for biological healing. The wound is copiously irrigated, and the deltopectoral interval is closed in layers over a closed-suction drain to prevent postoperative hematoma formation.
Complications, Incidence Rates, and Salvage Management
While pectoralis major repair is generally highly successful, it is not without potential pitfalls. Surgeons must be acutely aware of the complication profile and be prepared to manage adverse events. The overall complication rate for primary repair is relatively low, typically cited between 5% and 10%, but this rate increases significantly in chronic reconstructions or revision scenarios.
The most devastating complication is re-rupture of the repaired tendon. This typically occurs in the early postoperative period (within the first 12 weeks) and is almost always the result of patient non-compliance with range-of-motion restrictions or a premature return to heavy lifting. Re-rupture presents with a sudden return of pain, weakness, and loss of the axillary fold. Salvage management of a re-rupture is exceptionally challenging, requiring a revision surgery that almost universally mandates massive allograft reconstruction (e.g., Achilles tendon with bone block) due to the severe degradation of the native tendon tissue and the compromised bone of the proximal humerus.
Infection is another significant concern, particularly given the location of the incision near the axilla, an area prone to bacterial colonization. Superficial wound infections can often be managed with oral antibiotics and local wound care. However, deep surgical site infections involving the hardware or the tendon repair site require aggressive intervention, including urgent operative irrigation and debridement, hardware retention if the repair is stable, and prolonged intravenous antibiotic therapy guided by intraoperative cultures.
Nerve injury is a rare but profound complication. The axillary nerve, musculocutaneous nerve, and the pectoral nerves are all theoretically
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding pectoralis-major-repair