Pediatric Shoulder Fracture Management: An Intraoperative Masterclass
Key Takeaway
Join this intraoperative masterclass on pediatric shoulder fractures, specifically addressing proximal humerus and sternoclavicular joint injuries. We'll meticulously cover essential surgical anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution for closed reduction percutaneous pinning and open reduction techniques. Learn crucial pearls, pitfalls, and comprehensive postoperative management to optimize outcomes in these challenging cases.
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues, fellows, and residents, to this definitive intraoperative masterclass. Today, we are undertaking a rigorous exploration into the nuanced and highly specialized domain of pediatric shoulder fractures. The pediatric shoulder girdle operates under a unique biological paradigm, wherein the remarkable remodeling potential of immature woven bone often dictates a nonoperative approach. However, this inherent biological advantage can sometimes lull the unwary surgeon into a false sense of security. Certain high-energy injury patterns, specific degrees of displacement in older adolescents, and injuries threatening the mediastinal envelope demand precise, timely, and mechanically sound surgical intervention. Our focus in this chapter will be heavily weighted toward the operative management of specific proximal humerus fractures and medial clavicle/sternoclavicular disruptions, where the clinical stakes are magnified by the immediate proximity of vital neurovascular and cardiopulmonary structures.
The Unique Biological Milieu of the Pediatric Shoulder
The pediatric shoulder is not merely a miniaturized adult shoulder; it is a dynamic, evolving biomechanical construct characterized by active physes and a robust, thick periosteal sleeve. The proximal humeral physis is a critical engine of longitudinal growth, responsible for approximately 80% of the humerus's total length. This highly active growth plate profoundly influences our treatment algorithms. Because of its massive remodeling capacity, fractures that would unequivocally require osteosynthesis in an adult can often be managed with simple immobilization in a young child. Understanding the chronobiology of these growth plates is paramount. The proximal humeral physis typically remains open until age 14 to 17 in females and 16 to 18 in males. Consequently, the closer a child is to skeletal maturity, the less remodeling potential remains, thereby lowering the threshold for surgical reduction and fixation.
Similarly, the medial clavicular epiphysis presents a unique developmental timeline that frequently confounds diagnosis and management. It is the last secondary center of ossification to appear in the human body, typically ossifying between the ages of 18 and 20, and it is the absolute last physis to fuse, often remaining open until the 23rd to 25th year of life. Therefore, what appears clinically and radiographically as a sternoclavicular joint dislocation in a 19-year-old patient is, in reality, almost always a Salter-Harris type I or II fracture through the medial clavicular physis. This anatomical distinction is critical, as the robust periosteal sleeve usually remains attached to the sternum, providing a biological hinge that can aid in reduction and subsequent remodeling, provided the pathomechanics are properly understood and respected.
Epidemiological Trends and Injury Mechanisms
Epidemiologically, proximal humerus fractures account for approximately 5% of all pediatric fractures, exhibiting a bimodal distribution. The first peak occurs in early childhood, often secondary to falls from a modest height or playground equipment, resulting in metaphyseal buckle or minimally displaced fractures. The second peak occurs during the adolescent growth spurt, typically involving high-energy sports trauma, equestrian accidents, or motor vehicle collisions. These adolescent injuries frequently manifest as Salter-Harris type II fractures, where the metaphyseal Thurston-Holland fragment remains attached to the intact posterior periosteal hinge. The mechanism of injury usually involves a fall onto an outstretched hand with the shoulder in extension and external rotation, driving the humeral shaft anteriorly and superiorly.
Sternoclavicular injuries and medial clavicle physeal fractures are significantly rarer, representing less than 1% of all pediatric fractures. They are almost exclusively the result of high-energy mechanisms, such as a direct blow to the medial clavicle or a massive compressive force applied to the lateral shoulder during a collision (e.g., a rugby tackle or a high-speed motor vehicle accident). The direction of the applied force dictates the displacement vector. An anterolateral compressive force typically produces a posterior displacement of the medial clavicle, driving it into the superior mediastinum. Conversely, a posterolateral force results in anterior displacement. While anterior displacements are visually striking and more common, posterior displacements are true orthopedic emergencies due to their potential to compress or lacerate the underlying trachea, esophagus, and great vessels.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is raised or a pin is driven, a profound, three-dimensional understanding of the regional anatomy is non-negotiable. The shoulder girdle represents a complex, high-traffic intersection of osseous pillars, dynamic muscular stabilizers, and delicate, life-sustaining neurovascular bundles. Ignorance of these anatomical relationships is the fastest route to catastrophic iatrogenic complications.
Proximal Humerus Osteology and Physeal Dynamics
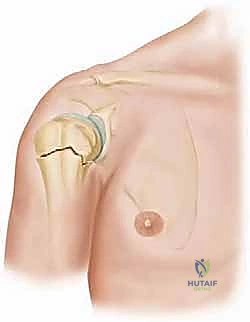
The proximal humerus consists of the articular head, the greater and lesser tuberosities, and the surgical and anatomic necks. In the pediatric patient, the proximal physis is not a simple planar structure; it is a complex, tent-shaped undulation that provides intrinsic mechanical stability against shear forces. The anterior periosteum of the proximal humerus is characteristically thinner and more tenuous than its thick, robust posterior counterpart. When a fracture occurs, the intact posterior periosteum acts as a tether, leading to the classic apex-anterior and varus angulation.
Furthermore, the long head of the biceps tendon, coursing through the bicipital groove, lies intimately adjacent to the fracture site. In completely displaced fractures, the proximal metaphyseal spike can buttonhole through the anterior periosteum, or the biceps tendon can become interposed between the fracture fragments. This soft tissue interposition acts as an insurmountable mechanical barrier to closed reduction, necessitating an open approach. The muscular forces acting on the fracture fragments further complicate reduction. The rotator cuff musculature (supraspinatus, infraspinatus, teres minor) abducts and externally rotates the proximal epiphyseal fragment, while the pectoralis major, latissimus dorsi, and teres major forcefully adduct and internally rotate the distal metaphyseal shaft.
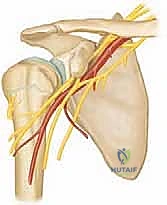
Neurovascular Topography and Danger Zones
The proximal humerus is enveloped by structures that demand absolute respect. Medially, the brachial plexus and the axillary artery and vein lie in dangerously close proximity to the surgical neck. Laterally, the axillary nerve is the structure at highest risk during percutaneous pinning or open approaches. The axillary nerve exits the axilla posteriorly through the quadrangular space, wrapping around the posterior and lateral aspects of the surgical neck of the humerus to innervate the deltoid and teres minor. In adults, the nerve lies approximately 5 to 7 centimeters distal to the lateral edge of the acromion. However, in the pediatric population, this distance is proportionally smaller and highly variable based on the child's age and height.
When placing lateral percutaneous pins, the trajectory must be carefully calculated to avoid transfixing or wrapping the axillary nerve. The musculocutaneous nerve, which pierces the coracobrachialis muscle, is also at risk during anterior approaches, particularly if aggressive medial retraction is employed. The vascular supply to the humeral head, primarily derived from the ascending branch of the anterior circumflex humeral artery and the robust posterior circumflex humeral artery, must be preserved. Fortunately, the robust anastomotic network in children makes avascular necrosis (AVN) following proximal humerus fractures exceedingly rare, even in completely displaced injuries.
Sternoclavicular Joint Anatomy and Mediastinal Proximity
The sternoclavicular (SC) joint, particularly its posterior aspect, is a region of extreme anatomical peril. It is a diarthrodial saddle joint, representing the sole true osseous articulation between the appendicular upper extremity and the axial skeleton. The joint's intrinsic osseous stability is poor; it relies almost entirely on its robust ligamentous complex, comprising the anterior and posterior sternoclavicular ligaments, the interclavicular ligament, and the costoclavicular (rhomboid) ligament. The posterior sternoclavicular ligament is the most critical stabilizer against both anterior and posterior translation.
Immediately posterior to the SC joint and the medial third of the clavicle lies the superior mediastinum, a densely packed anatomical bottleneck. The structures at immediate risk during a posterior dislocation include the brachiocephalic (innominate) artery and vein, the superior vena cava, the subclavian vessels, the vagus and phrenic nerves, the trachea, and the esophagus. The distance between the posterior aspect of the medial clavicle and these vital structures can be measured in mere millimeters. Therefore, a posterior sternoclavicular dislocation is not merely an orthopedic injury; it is a potentially life-threatening vascular and airway emergency that requires an immediate, coordinated multidisciplinary response, often mandating the standby presence of a pediatric thoracic or vascular surgeon during reduction maneuvers.
Exhaustive Indications and Contraindications
The decision to transition from nonoperative observation to surgical intervention in pediatric shoulder trauma requires a sophisticated synthesis of patient age, injury severity, physiological demands, and a deep understanding of natural history. The threshold for surgery is dynamic, shifting significantly as the child approaches skeletal maturity.
Decision Making in Proximal Humerus Fractures
For proximal humerus fractures, the Neer-Horwitz classification provides a useful framework based on the degree of displacement. However, the patient's age is the ultimate arbiter of treatment. In children under the age of 10 to 11 years, the remodeling potential is so vast that even fractures with 100% displacement and up to 70 degrees of angulation can remodel to normal anatomic alignment without functional deficit. In this cohort, surgery is rarely indicated unless the fracture is open, associated with a neurovascular injury, or part of a severe polytrauma where mobilization is required.
Conversely, in adolescents older than 11 to 12 years, the remodeling potential precipitously declines. In this older demographic, acceptable parameters for nonoperative management are generally restricted to less than 30 to 40 degrees of angulation and less than 50% translation. Fractures exceeding these parameters, or those that are highly unstable and repeatedly lose reduction in a sling or spica cast, require surgical stabilization. Furthermore, multi-system trauma patients, where the upper extremity must be utilized for weight-bearing during transfers (e.g., concomitant lower extremity fractures), are strong candidates for early internal fixation.
Triage and Indications for Sternoclavicular Injuries
The indications for intervention in medial clavicle physeal fractures and SC joint injuries are dictated primarily by the direction of displacement and the presence of compressive symptoms. Anterior displacements, while cosmetically prominent, rarely cause functional deficits and are almost universally treated nonoperatively with a brief period of sling immobilization for comfort. The resultant bony prominence often remodels significantly over time.
Posterior displacements, however, are absolute indications for urgent reduction due to the high risk of mediastinal compromise. Symptoms such as stridor, dyspnea, dysphagia, choking sensation, or venous engorgement of the ipsilateral upper extremity are clinical red flags indicating impending catastrophic compression. Even in the absence of overt symptoms, all documented posterior displacements should undergo an attempt at closed reduction under general anesthesia. If closed reduction fails—often due to buttonholing of the medial clavicle through the posterior periosteum or interposition of the subclavius muscle—prompt open reduction is mandatory.
| Parameter | Indications for Surgical Intervention | Contraindications / Nonoperative Management |
|---|---|---|
| Proximal Humerus (Age < 11) | Open fractures, vascular compromise, polytrauma requiring upper extremity weight-bearing. | Up to 100% displacement and 70° angulation are acceptable; manage with sling/swathe. |
| Proximal Humerus (Age > 11) | > 40° angulation, > 50% translation, irreducible fractures (biceps interposition), unstable reductions. | < 40° angulation, < 50% translation, minimally displaced Salter-Harris I/II. |
| Sternoclavicular Joint | Posterior displacement (urgent), mediastinal compression (stridor, dysphagia, venous congestion), failed closed reduction of posterior injury. | Anterior displacement (cosmetic deformity only), asymptomatic chronic dislocations. |
| Clavicle Shaft | Open fractures, skin tenting with impending necrosis, severe displacement in older adolescents with high athletic demands. | Most pediatric midshaft fractures, regardless of displacement, heal predictably with remodeling. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of any surgical intervention is largely determined before the first incision is made. Meticulous preoperative planning, rigorous advanced imaging analysis, and precise patient positioning are the cornerstones of a flawless intraoperative execution.
Clinical Evaluation and Advanced Imaging Protocols
A comprehensive history must detail the mechanism of injury, the precise onset of symptoms, and crucially, any antecedent neurologic symptoms or paresthesias in the distal extremity. For high-energy injuries, absolute adherence to Advanced Trauma Life Support (ATLS) protocols is mandatory before addressing the orthopedic injury. On physical examination, the skin must be meticulously evaluated for impending necrosis or open wounds. A thorough, documented neurologic examination assessing the brachial plexus, axillary nerve, and peripheral nerves is essential to establish a baseline and identify acute deficits.
Standard radiographic evaluation of the shoulder must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary view is critical for assessing the degree of anterior or posterior translation of the humeral head.


For suspected medial clavicle or SC joint injuries, standard chest radiographs are often insufficient due to overlapping rib and mediastinal shadows. The "serendipity view," an AP radiograph centered on the manubrium with the beam angled 40 degrees cephalad, is invaluable for comparing the relative superior-inferior positions of both medial clavicles.
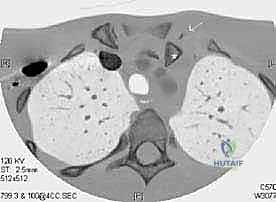
When a posterior sternoclavicular dislocation is suspected, a contrast-enhanced Computed Tomography (CT) scan is the absolute gold standard and should be obtained emergently. The CT scan, particularly with 3D reconstructions, provides unparalleled detail regarding the exact position of the displaced clavicle relative to the trachea, esophagus, and great vessels. The use of intravenous contrast allows for precise mapping of the vascular anatomy, ruling out occult intimal tears or partial occlusions.

Operating Room Setup and Anesthesia Considerations
For proximal humerus pinning, general anesthesia with profound muscle relaxation is required to overcome the deforming forces of the pectoralis major and rotator cuff. A regional interscalene block can be utilized for postoperative pain control, provided a thorough preoperative neurologic exam has been documented. For posterior SC joint reductions, the anesthesia team must be prepared for potential airway difficulties. The patient should be intubated, and blood products should be readily available in the room. A cardiothoracic or vascular surgeon should be formally consulted and ideally present in the operating suite during the reduction maneuver, as sudden dislodgement of the clavicle can unroof a tamponaded vascular laceration.
Patient Positioning and Fluoroscopic Optimization
For operative management of proximal humerus fractures, the patient is placed in a modified beach-chair position. The back of the radiolucent table is elevated approximately 30 to 40 degrees. Excessive elevation should be avoided, as it severely restricts the excursion of the C-arm and complicates the acquisition of true orthogonal fluoroscopic views.

A vacuum positioning device (beanbag) is utilized to secure the patient's torso, allowing the operative shoulder to be translated slightly off the lateral edge of the table. This is critical for achieving full extension of the arm during reduction maneuvers. A chest strap or heavily padded tape is secured across the contralateral torso to prevent the patient from being pulled off the table during longitudinal traction.


The entire forequarter, from the base of the neck to the fingertips, must be prepped and draped free to allow for unencumbered manipulation of the arm. The C-arm is typically brought in from the head of the table, parallel to the patient's torso. By tilting the C-arm over the shoulder, a true AP view can be obtained. Rotating the C-arm 90 degrees allows for an axillary lateral view without requiring the surgeon to reposition the potentially unstable fracture.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be methodical, respecting the delicate soft tissue envelope while achieving mechanically sound osseous stability. We will detail the techniques for both closed and open management of the proximal humerus, followed by the critical steps for addressing the posterior sternoclavicular joint.
Closed Reduction and Percutaneous Pinning of the Proximal Humerus
The vast majority of operative proximal humerus fractures can be managed with Closed Reduction and Percutaneous Pinning (CRPP). The reduction maneuver relies on reversing the mechanism of injury. An assistant provides counter-traction using a sheet wrapped around the patient's upper torso. The surgeon applies sustained longitudinal traction to the arm in a position of forward flexion and slight abduction. This traction must be maintained for several minutes to fatigue the spastic pectoralis major and latissimus dorsi muscles.
Once length is restored, the arm is gently externally rotated, and direct posterior pressure is applied to the anteriorly displaced proximal humeral shaft. This maneuver aims to unlock the metaphyseal spike from the anterior periosteum and hinge it back onto the intact posterior periosteal sleeve. Reduction is confirmed in orthogonal fluoroscopic planes.
Once an acceptable reduction is achieved, percutaneous pinning is performed. Smooth Kirschner wires (typically 1.6 mm to 2.5 mm, depending on the child's size) or partially threaded Steinmann pins are utilized. The preferred configuration is two or three lateral pins directed from distal-lateral to proximal-medial, engaging the dense subchondral bone of the humeral head.

To avoid the axillary nerve, the starting point for lateral pins should be carefully selected. A safe zone is generally considered to be distal to the deltoid insertion, though a more proximal starting point can be used if a mini-open technique is employed to directly visualize and protect the nerve. An anterior pin can be added for increased rotational stability, driven from anterior-distal to posterior-proximal, taking care to avoid the biceps tendon and musculocutaneous nerve. The pins are typically left protruding through the skin, bent, and capped to facilitate easy removal in the clinic.


Open Reduction Techniques for Irreducible Proximal Humerus Fractures
If closed reduction is unsuccessful after two or three concerted attempts, the surgeon must promptly transition to an open reduction. Repeated, forceful closed manipulation damages the physis and increases the risk of iatrogenic neurovascular injury. Irreducibility is almost always caused by the interposition of the long head of the biceps tendon, the anterior periosteum, or the deltoid muscle.
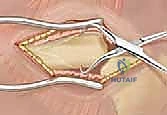
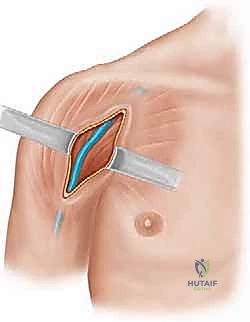
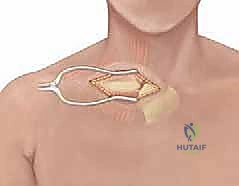
A standard deltopectoral approach is utilized. The skin incision is made over the coracoid process, extending distally along the deltopectoral groove. The cephalic vein is identified and typically retracted laterally with the deltoid muscle to preserve its primary venous drainage, while the pectoralis major is retracted medially.


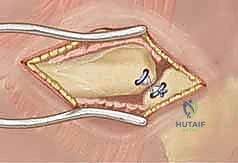
Deep dissection reveals the fracture site. The proximal metaphyseal fragment is often found buttonholed through the anterior periosteum. The long head of the biceps tendon must be identified and carefully extricated from the fracture site using a blunt hook or Freer elevator. Once the soft tissue interposition is cleared, the fracture is anatomically reduced under direct vision. Fixation is then achieved using the same percutaneous pinning principles described above, ensuring the pins do not traverse the biceps tendon or intra-articular space.
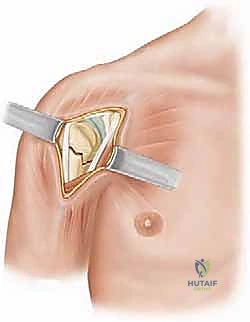
Surgical Management of Posterior Sternoclavicular Dislocations
For posterior SC joint dislocations, the patient is positioned supine with a bump placed vertically
