Pediatric Femoral Shaft Fractures: Masterclass in Flexible Intramedullary Nailing

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling a pediatric femoral shaft fracture with flexible intramedullary nailing. This masterclass will cover meticulous preoperative assessment, precise patient positioning, detailed surgical anatomy, and a granular, real-time breakdown of the retrograde nailing technique. We'll emphasize critical intraoperative decision-making, potential pitfalls, and comprehensive postoperative management to ensure optimal outcomes for our young patients.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we are confronted with a classic yet endlessly fascinating case: a pediatric femoral shaft fracture in a 7-year-old boy. We will be employing flexible intramedullary nailing (FIN), utilizing titanium elastic nails (TENs)—a technique that, when executed with biomechanical precision, offers unparalleled stability while permitting the micro-motion necessary for robust secondary bone healing. This intervention is not merely an exercise in hardware deployment; it is a profound application of pediatric osteology, dynamic biomechanics, and meticulous soft-tissue handling designed to accelerate mobilization and mitigate the profound psychosocial morbidity historically associated with spica casting in this age demographic.
The epidemiology of pediatric femoral shaft fractures demonstrates a distinct bimodal distribution. The first peak occurs in early childhood, often associated with low-energy falls or, critically, non-accidental trauma (child abuse). The second peak emerges in early adolescence, typically secondary to high-energy trauma such as motor vehicle collisions, pedestrian-versus-auto incidents, or extreme sports. Our patient sustained a spiral diaphyseal fracture during a football tackle, representing a moderate-energy torsional force. In evaluating these mechanisms, the clinician must maintain a high index of suspicion; a low-energy mechanism resulting in a transverse or comminuted diaphyseal fracture in an older child mandates a rigorous workup to exclude pathologic entities, including unicameral bone cysts, aneurysmal bone cysts, or primary bone sarcomas.
Before embarking on any surgical intervention, a comprehensive preoperative assessment is an absolute mandate, adhering strictly to Advanced Trauma Life Support (ATLS) protocols. The initial clinical evaluation must rigorously exclude vascular or neurologic compromise. A detailed neurovascular examination documenting palpable pulses, brisk capillary refill, intact dermatomal sensation, and baseline motor function is critical. Any deviation necessitates immediate vascular or neurosurgical consultation and potentially emergent exploration. Furthermore, high-energy mechanisms demand vigilance for concomitant injuries, including occult visceral trauma, closed head injuries, and impending compartment syndrome of the thigh—a rare but catastrophic complication if missed.
Finally, the clinical examination must extend beyond the immediate zone of injury. A subtle but indispensable step is the examination of the ipsilateral knee and hip. Femoral shaft fractures, particularly those resulting from significant axial or torsional loads, can be associated with ligamentous disruptions of the knee or occult injuries to the hip, such as a slipped capital femoral epiphysis (SCFE) or a femoral neck fracture. These concomitant injuries may be masked by the profound muscle spasm associated with the primary fracture and often only become apparent under anesthesia. A thorough evaluation under anesthesia, prior to prepping and draping, is a non-negotiable component of our surgical algorithm.
Detailed Surgical Anatomy and Biomechanics
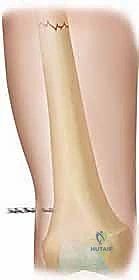
To master flexible intramedullary nailing, one must possess an intimate understanding of the dynamic, evolving anatomy of the pediatric femur. The femur develops from a primary ossification center in the diaphysis, appearing around the fourth week of gestation. Crucially, the proximal and distal epiphyses remain cartilaginous at birth. The distal femoral physis, which appears at approximately seven months of gestation, is particularly vital, contributing up to 70% of the longitudinal growth of the femur. Our surgical approach, specifically the selection of our entry portals in the distal metaphysis, must be meticulously planned to remain strictly extra-physeal to prevent catastrophic growth arrest or angular deformity.
The vascular anatomy of the pediatric femur dictates our biological approach to fracture fixation. The intact femur relies heavily on the endosteal blood supply, derived primarily from the nutrient artery, a branch of the profunda femoris. However, following a diaphyseal fracture, the endosteal supply is disrupted, and the periosteal vascular network undergoes rapid hypertrophy, becoming the dominant source of perfusion for the healing callus. Flexible intramedullary nailing is biologically superior to open plating precisely because it is a closed, or minimally invasive, technique that preserves this critical periosteal envelope and the osteogenic fracture hematoma, thereby optimizing the environment for rapid secondary bone healing.
Understanding the muscular anatomy is essential for anticipating the deforming forces acting upon the fracture fragments. The proximal fragment is typically subjected to flexion, abduction, and external rotation due to the unyielding pull of the iliopsoas and the gluteus medius and minimus. Conversely, the distal fragment is often drawn into varus by the adductor magnus and extended by the gastrocnemius. Diaphyseal fractures, such as the one we are treating today, are subject to significant shortening due to the longitudinal spasm of the robust quadriceps and hamstring muscle groups. Overcoming these forces requires adequate intraoperative traction and precise manipulation of the fragments during nail passage.
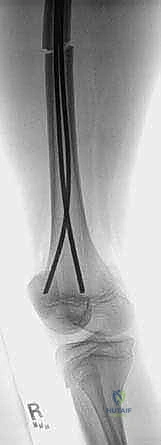
The biomechanical genius of the flexible intramedullary nail lies in the principle of symmetrical three-point bending. Unlike rigid, locked intramedullary nails used in adults, which provide absolute stability, titanium elastic nails rely on their modulus of elasticity. When two pre-bent nails of equal diameter are inserted from opposite sides of the metaphysis and advanced across the fracture site, they create a dynamic, internally braced construct. The nails exert outward pressure at the entry sites, inward pressure at the fracture site, and outward pressure in the proximal metaphysis. This symmetrical tension counteracts angular and rotational forces while permitting axial micro-motion, which is the fundamental mechanical stimulus for robust, circumferential callus formation.
Exhaustive Indications and Contraindications
The success of flexible intramedullary nailing is inextricably linked to rigorous patient selection. The ideal candidate is a pediatric patient between the ages of 5 and 11 years, weighing less than 49 kilograms (approximately 100 pounds). In this demographic, the medullary canal is sufficiently narrow to allow the elastic nails to achieve adequate cortical purchase, and the patient's body weight is not so immense as to overcome the yield strength of the titanium construct. For children younger than 5, nonoperative management with a hip spica cast remains the gold standard, offering excellent outcomes with minimal morbidity.
Fracture morphology is an equally critical determinant. Flexible nailing is exquisitely suited for transverse, short oblique, and short spiral fractures located within the middle 50% to 70% of the femoral diaphysis. These fracture patterns are inherently "length-stable," meaning that once the cortical ends are apposed, the bone itself resists further axial shortening. The elastic nails provide the necessary angular and rotational control, while the inherent stability of the fracture pattern prevents telescoping.
Conversely, strict contraindications must be respected to avert construct failure and catastrophic malunion. Patients weighing over 49 kilograms or those older than 12 years are generally poor candidates; the increased biomechanical demands often result in plastic deformation of the nails, loss of reduction, and severe leg length discrepancy. Severe comminution (length-unstable fractures) is a relative contraindication; if FIN is attempted in these scenarios, adjunctive stabilization, such as end caps or supplementary spica casting, is often required. Furthermore, fractures located in the proximal or distal subtrochanteric or supracondylar regions are contraindicated, as the nails cannot achieve the necessary three-point spread within the short metaphyseal fragments.
| Parameter | Favorable Indications for FIN | Absolute/Relative Contraindications |
|---|---|---|
| Patient Age | 5 to 11 years | < 5 years (Spica preferred), > 12 years (Rigid nail/Plate) |
| Patient Weight | < 49 kg (100 lbs) | > 49 kg (High risk of plastic deformation) |
| Fracture Location | Middle 50-70% of Diaphysis | Proximal 1/3 (Subtroch) or Distal 1/3 (Supracondylar) |
| Fracture Pattern | Transverse, Short Oblique, Short Spiral | Severe Comminution (Length Unstable), Segmental |
| Neuromuscular | Neurotypically normal | Severe Spasticity (e.g., severe Cerebral Palsy) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the blueprint for surgical success; it is where complications are anticipated and averted before the first incision is made. The foundation of this planning rests on high-quality, full-length orthogonal radiographs of the involved femur.

Crucially, these images must encompass the hip and knee joints to rule out concomitant intra-articular pathology. Advanced imaging, such as computed tomography (CT), is rarely indicated for isolated diaphyseal fractures but may be deployed if an underlying pathologic lesion or complex intra-articular extension is suspected.
Nail sizing and selection dictate the biomechanical integrity of the final construct. We rigorously apply the "40% Rule": the sum of the diameters of the two chosen nails must equal approximately 40% of the narrowest diameter of the medullary canal (the isthmus), as measured on the anteroposterior and lateral radiographs. For instance, an isthmus measuring 10 millimeters mandates the use of two 2.0-millimeter nails. It is an absolute biomechanical imperative that the two nails be of identical diameter; utilizing mismatched nails (e.g., a 3.0mm and a 2.0mm) will result in asymmetrical bending forces, inevitably driving the fracture into a varus or valgus malalignment.
Patient positioning on the operating table is a critical step that demands the surgeon's direct supervision. We advocate for the use of a radiolucent fracture table, which allows for precise, dialed-in traction and counter-traction.

The patient is positioned supine, with a well-padded perineal post secured to prevent pudendal nerve neurapraxia or soft tissue necrosis. The injured extremity is secured in the traction boot, and gentle, sustained longitudinal traction is applied to overcome muscle spasm and restore anatomic length. The limb is positioned in approximately 15 to 20 degrees of abduction to facilitate unhindered access to the medial entry portal.
The uninjured contralateral extremity must be managed with equal care. We employ a "scissoring" technique, placing the well leg in extension and dropping it below the level of the injured limb. This configuration removes the contralateral femur from the fluoroscopic field, allowing for crystal-clear lateral projections of the injured extremity without requiring complex C-arm maneuvers. We strictly avoid extreme lithotomy or highly flexed well-leg positions, as prolonged elevation in these postures has been definitively linked to devastating well-leg compartment syndrome. Once positioned, the C-arm is brought in to confirm baseline reduction and visualization from the trochanter to the distal physis.
Step-by-Step Surgical Approach and Fixation Technique
Initial Reduction and Entry Portal Preparation
With the patient prepped and draped, we initiate the procedure by confirming our closed reduction under fluoroscopy. The goal is not perfect anatomic alignment at this stage, but rather the restoration of length and the correction of gross angular and rotational deformities to facilitate smooth nail passage. Once acceptable alignment is confirmed, we turn our attention to the distal femur. Using the C-arm in the true AP plane, we meticulously identify and mark the distal femoral physis. Our entry points are precisely calculated to be 2.0 to 2.5 centimeters proximal to this physeal line, ensuring we remain safely within the metaphysis.
Longitudinal incisions, approximately 2 to 3 centimeters in length, are made medially and laterally over the marked entry sites. The dissection is carried down through the subcutaneous tissue. Laterally, the fascia lata is incised, and the vastus lateralis is bluntly split in line with its fibers. Medially, the vastus medialis is similarly split. Meticulous hemostasis is maintained, and blunt retractors are placed to expose the metaphyseal bone. It is paramount to avoid aggressive periosteal stripping, preserving the biological envelope.
Cortical Fenestration
Creating the cortical entry holes requires precision to prevent iatrogenic fractures or physeal injury. We utilize a sharp awl or a cannulated drill system.

The awl is initially introduced perpendicular to the bone cortex to establish a definitive starting point and prevent skiving.
Once the outer cortex is breached, the handle of the awl is systematically dropped toward the horizontal plane, angling the tip proximally at approximately a 45-degree angle to the long axis of the femoral shaft.

This oblique trajectory is critical; it creates a gliding path for the elastic nail, preventing it from abutting the opposite cortex and causing a catastrophic cortical blowout. The process is repeated on the contralateral side, ensuring both entry portals are symmetric and adequately sized to accommodate the chosen titanium nails.
Nail Contouring and Insertion
Prior to insertion, the titanium elastic nails must be meticulously contoured. A smooth, continuous bow is imparted to each nail, ensuring that the apex of the curve will reside exactly at the level of the fracture site once fully seated. This pre-bending is the engine of the three-point fixation biomechanics. Furthermore, the leading tip of the nail is slightly over-bent to facilitate "steering" off the inner cortices during passage.

The first nail is loaded into the T-handle or F-tool inserter. It is introduced into the prepared entry portal with the tip oriented to glide along the inner cortex.

Using oscillating, twisting motions rather than brute axial force, the nail is advanced up the medullary canal toward the fracture site.

The second nail is then introduced through the contralateral portal and advanced to the same level. It is imperative that both nails cross the fracture site simultaneously to prevent displacing the fracture fragments.
Fracture Passage and Final Seating
Crossing the fracture site is often the most technically demanding phase of the procedure. Under live fluoroscopy, the surgeon coordinates longitudinal traction, manual manipulation of the thigh, and the rotational steering of the nail tips.

If the fracture is recalcitrant, a percutaneous joystick (such as a Schanz pin) can be inserted into the proximal fragment to manipulate it into alignment.

Once the first nail crosses the fracture into the proximal fragment, the second nail is immediately advanced across the gap.
The nails are then driven proximally into the dense cancellous bone of the proximal metaphysis.

Crucially, the tips must be rotated so that they diverge—one anchoring toward the greater trochanter and the other toward the lesser trochanter. This divergence maximizes rotational stability.

Finally, the distal ends of the nails are cut, leaving approximately 1.5 to 2.0 centimeters protruding from the cortex.
This length is sufficient to allow for future hardware removal but short enough to minimize irritation of the iliotibial band and vastus musculature.

The wounds are thoroughly irrigated and closed in layers.
Complications, Incidence Rates, and Salvage Management
Despite its elegance, flexible intramedullary nailing is not without potential complications. The most frequently encountered issue, occurring in up to 15-20% of cases, is symptomatic hardware prominence at the distal insertion sites. If the nails are left too long, or if they back out due to fracture settling, they can cause profound irritation of the vastus medialis or the iliotibial band, leading to bursa formation, pain, and restricted knee flexion. Management typically involves conservative measures until radiographic union is achieved, followed by prompt hardware removal.
Malunion is a more severe complication, encompassing leg length discrepancies and angular or rotational deformities. Overgrowth of the fractured femur is a well-documented phenomenon in children under 10, often resulting in a 1 to 2 centimeter length discrepancy. Conversely, in heavier patients or those with length-unstable fracture patterns, the elastic nails may fail to maintain length, resulting in shortening. Angular deformities (varus/valgus or apex anterior/posterior) typically result from technical errors, most notably the use of mismatched nail diameters or failure to achieve divergent proximal fixation. While pediatric bone possesses tremendous remodeling potential, deformities exceeding 15 degrees in older children may require corrective osteotomy.
Neurologic and vascular injuries are rare but represent catastrophic surgical emergencies. Aggressive, prolonged traction on the fracture table can induce a traction neurapraxia of the sciatic or pudendal nerves. Iatrogenic injury to the superficial femoral artery or vein can occur during the medial approach if the dissection strays anteriorly or if the awl plunges through the posterior cortex. Meticulous adherence to anatomical landmarks and disciplined surgical technique are the only safeguards against these devastating events.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Symptomatic Hardware Prominence | 10% - 20% | Nails left > 2cm long; Nail back-out | Analgesia; Early removal after definitive bony union |
| Leg Length Discrepancy (Overgrowth) | 5% - 10% | Hyperemic response in children < 10 yrs | Usually resolves; Epiphysiodesis if > 2cm at skeletal maturity |
| Loss of Reduction / Malunion | 3% - 8% | Patient weight > 49kg; Mismatched nails; Comminution | Revision to submuscular plate or rigid IM nail; Corrective osteotomy |
| Skin Breakdown / Infection | 1% - 2% | Poor soft tissue handling; Prominent hardware | Local wound care; Oral/IV antibiotics; Hardware removal |
| Neurologic Injury (Neurapraxia) | < 1% | Excessive traction; Perineal post pressure | Observation; Physical therapy; Usually resolves spontaneously |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following flexible intramedullary nailing is phased, dynamic, and tailored to the biomechanical stability of the construct and the biologic progression of fracture healing. The immediate postoperative phase (Weeks 0-2) prioritizes pain management, edema control, and the restoration of early joint kinematics. Patients are typically discharged within 24 to 48 hours. Early, gentle active-assisted range of motion of the hip and knee is initiated immediately to prevent arthrofibrosis and stimulate synovial nutrition. Depending on the fracture pattern, patients are restricted to non-weight-bearing or toe-touch weight-bearing with the assistance of crutches or a walker.
The intermediate phase (Weeks 2-6) marks the transition from soft-tissue recovery to active bone healing. At the two-to-three-week mark, initial radiographic assessment should demonstrate the nascent formation of a periosteal callus. As the callus matures and bridges the fracture site, the patient's weight-bearing status is progressively advanced. Physical therapy during this phase focuses on isometric strengthening of the quadriceps, hamstrings, and gluteal musculature, which often atrophy rapidly following femoral trauma. Aquatic therapy can be highly beneficial during this transition, allowing for gait mechanics training in a reduced-gravity environment.
The late phase (Weeks 6-12 and beyond) represents the return to full functional capacity. By six to eight weeks, orthogonal radiographs should confirm robust, circumferential bridging callus, signifying clinical union. At this juncture, patients are cleared for full, unassisted weight-bearing. Advanced physical therapy focuses on proprioception, dynamic balance, and sports-specific agility drills. It is during this phase that the clinician must carefully assess for any leg length discrepancy or subtle rotational malalignment.
Hardware removal is a planned, final step in the treatment algorithm. Unlike rigid nails in adults, titanium elastic nails in pediatric patients are routinely removed to prevent long-term complications, such as soft-tissue irritation or theoretical stress shielding, and to avoid complications should a subsequent fracture occur. Removal is typically scheduled between 6 and 12 months postoperatively, contingent upon unequivocal radiographic evidence of complete cortical consolidation and remodeling. The removal procedure is generally a brief, outpatient surgery, though surgeons must be prepared for the possibility of bony overgrowth encapsulating the distal nail ends.
Summary of Landmark Literature and Clinical Guidelines
The evolution of pediatric femoral shaft fracture management has been heavily influenced by robust clinical literature and formalized practice guidelines. Historically, the American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines have documented a paradigm shift. While spica casting remains the unchallenged gold standard for children under five years of age, the guidelines strongly endorse flexible intramedullary nailing as the treatment of choice for neurotypically normal children aged 5 to 11 years, citing significantly reduced hospitalization times, faster return to weight-bearing, and profound improvements in psychosocial metrics for both the patient and the family.
