Pectoralis Major Transfer for Long Thoracic Nerve Palsy: An Intraoperative Masterclass
Key Takeaway
Join us in the OR for a detailed masterclass on pectoralis major transfer for long thoracic nerve palsy. We'll meticulously cover comprehensive anatomy, precise patient positioning, step-by-step surgical execution from incision to fixation, and critical pearls to manage scapular winging. Understand graft choices, tensioning, and rehabilitation for optimal outcomes in patients with persistent symptomatic serratus anterior dysfunction.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we address a formidable challenge in reconstructive shoulder surgery: the pectoralis major transfer for long thoracic nerve (LTN) palsy. This pathology represents a profound disruption of the scapulothoracic articulation, stripping the glenohumeral joint of its dynamic foundation. This operation transcends the mere transposition of a muscle-tendon unit; it is a sophisticated biomechanical reconstruction designed to restore critical shoulder kinematics, eradicate debilitating scapular winging, and return the patient to a highly functional state. Our objective is to meticulously re-establish the stable fulcrum necessary for unimpeded glenohumeral motion in three-dimensional space.
Pathogenesis of Long Thoracic Nerve Palsy
Long thoracic nerve palsy stands as the most ubiquitous etiology of symptomatic scapular winging, precipitating profound weakness or complete paralysis of the serratus anterior muscle. The pathogenesis of this neuropathy is highly variable, encompassing idiopathic, iatrogenic, viral, compressive, and traumatic origins. Most traumatic injuries are neurapraxic or axonotmetic, stemming from blunt force trauma to the lateral chest wall or acute traction injuries incurred during sudden, forceful depression of the shoulder girdle coupled with contralateral cervical lateral flexion. Iatrogenic injuries remain a significant clinical concern, frequently occurring during radical mastectomies, axillary lymph node dissections, first rib resections for thoracic outlet syndrome, or transaxillary sympathectomies.
In addition to mechanical trauma, viral etiologies such as Parsonage-Turner syndrome (neuralgic amyotrophy) frequently target the long thoracic nerve. This acute brachial neuritis typically presents with severe, unremitting shoulder girdle pain followed by profound weakness of the serratus anterior as the pain begins to subside. Regardless of the etiology, the resulting denervation deprives the scapula of its primary protractor and upward rotator. Without this critical tether to the posterior thoracic cage, the scapula destabilizes, leading to the pathognomonic medial and dorsal translation of the inferior angle—the classic "winged" posture.

The biomechanical cascade following serratus anterior paralysis is devastating to upper extremity function. The loss of upward scapular rotation severely limits glenohumeral elevation, typically capping active forward flexion and abduction at approximately 90 to 110 degrees. Furthermore, the uncoupling of the scapulothoracic rhythm precipitates secondary subacromial impingement, as the acromion fails to clear the advancing greater tuberosity during attempted arm elevation. This mechanical conflict, combined with the muscular fatigue of compensatory periscapular muscles (such as the upper trapezius and levator scapulae), generates significant pain and functional impairment, profoundly diminishing the patient's quality of life.
Clinical Presentation and Diagnostic Evaluation
Patients with LTN palsy typically present with a constellation of vague shoulder pain, profound weakness with overhead activities, and a characteristic cosmetic deformity of the posterior thorax. The pain is often described as a deep, aching sensation around the periscapular region, frequently radiating to the neck due to the compensatory spasm of the trapezius. Clinical examination reveals a visible prominence of the entire medial border of the scapula, which is dramatically exacerbated when the patient performs a wall push-up test or attempts resisted forward elevation.


A critical component of the physical examination is the Scapular Stabilization Test. By manually compressing the medial border of the scapula against the thoracic wall, the examiner artificially restores the serratus anterior's stabilizing function. If the patient subsequently demonstrates a marked improvement in active forward elevation and a reduction in pain, this firmly corroborates the diagnosis of serratus anterior dysfunction and predicts a favorable outcome following a successful muscle transfer. The clinician must also meticulously differentiate serratus winging from trapezius winging (spinal accessory nerve palsy), where the scapula translates laterally, and rhomboid winging (dorsal scapular nerve palsy).
Diagnostic imaging begins with standard orthogonal radiographs of the shoulder, cervical spine, and chest to exclude osseous abnormalities, such as osteochondromas of the ventral scapula, cervical spondylosis, or structural scoliosis. While advanced imaging like MRI is occasionally utilized to evaluate for compressive lesions along the nerve's course, Electromyography (EMG) and Nerve Conduction Velocity (NCV) studies remain the gold standard. These neurodiagnostic studies confirm denervation within the serratus anterior, map the severity of the injury, and, through serial evaluations every 3 to 6 months, track neural recovery. The persistence of dense fibrillation potentials and the absence of nascent motor unit potentials at 12 to 24 months post-injury constitute a definitive indication for surgical reconstruction.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the regional anatomy is an absolute prerequisite for executing this transfer safely and effectively. The surgical field encompasses the anterior chest wall, the depths of the axilla, and the posterior scapulothoracic articulation, requiring the surgeon to navigate a complex array of critical neurovascular structures.
The Serratus Anterior and Scapulothoracic Articulation
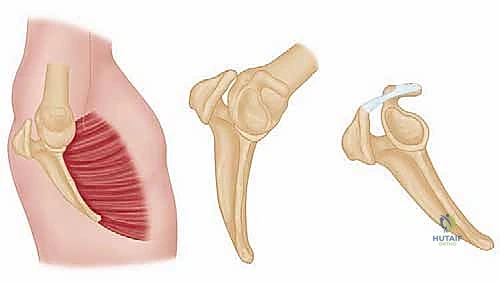
The serratus anterior is a broad, powerful muscle sheet that forms the medial wall of the axilla. It originates via nine fleshy digitations from the outer surfaces and superior borders of the upper nine ribs. The muscle fibers sweep posteriorly, intimately conforming to the convex curvature of the thoracic cage, deep to the subscapularis, to insert along the entire costal surface of the medial border of the scapula.
Anatomically and functionally, the serratus anterior is divided into three distinct segments. The superior division, originating from the first and second ribs, inserts near the superior angle of the scapula and acts primarily as an anchor. The middle division, arising from the second through fourth ribs, inserts along the length of the medial border and functions as a powerful protractor. The inferior division is the thickest, longest, and most biomechanically critical segment; it originates from the fifth through ninth ribs and converges to a robust insertion at the inferior angle of the scapula. This inferior division is the primary driver of upward scapular rotation and the principal structure whose function we seek to replicate with the pectoralis major transfer.
Biomechanically, the serratus anterior operates in a critical force couple with the upper and lower trapezius to dictate scapular kinematics. During arm elevation, the serratus anterior pulls the inferior angle anterolaterally, while the upper trapezius elevates the acromion and the lower trapezius depresses the medial spine of the scapula. This synchronized upward rotation of the glenoid provides a stable platform for the humeral head, maximizes the mechanical advantage of the deltoid, and prevents impingement of the rotator cuff beneath the coracoacromial arch. Loss of the serratus anterior disrupts this entire kinetic chain.
The Long Thoracic Nerve
The long thoracic nerve (Nerve of Bell) exhibits a unique and perilous anatomical course that predisposes it to injury. It arises from the ventral rami of the fifth, sixth, and seventh cervical nerve roots (C5, C6, C7). The C5 and C6 roots typically pierce the scalenus medius muscle, a common site for fascial entrapment, before merging. They are subsequently joined by the C7 root contribution, which usually travels anterior to the scalenus medius.

After its formation, the nerve dives posterior to the brachial plexus and the axillary vessels, entering the axillary sheath at the level of the first rib. It then descends vertically along the lateral chest wall, superficial to the fascia of the serratus anterior muscle. This superficial, exposed trajectory spanning approximately 24 centimeters makes the nerve extraordinarily vulnerable.
Unlike most motor nerves that run deep to the muscles they innervate, the LTN lies exposed on the superficial surface of the serratus anterior. It provides segmental innervation to the muscle digitations as it descends. Its vulnerability is exacerbated during surgical procedures in the axilla or lateral decubitus positioning, where excessive traction on the abducted arm can stretch the nerve against the first rib or the fascial bands of the scalene musculature, leading to ischemic neurapraxia.
The Pectoralis Major Muscle and Transfer Rationale
The pectoralis major is a massive, fan-shaped muscle that serves as the premier donor for reconstructing serratus anterior function. It is composed of two distinct heads: the clavicular head, originating from the medial half of the clavicle, and the sternocostal (sternal) head, originating from the anterior surface of the sternum, the superior six costal cartilages, and the aponeurosis of the external oblique.
These two heads converge laterally to form a complex, bilaminar tendon that inserts into the lateral lip of the bicipital groove of the humerus. Crucially, the tendon undergoes a 180-degree twist prior to insertion. The fibers of the clavicular head insert anteriorly and distally, while the fibers of the sternal head twist beneath them to insert more proximally and posteriorly. This twisted configuration must be carefully unraveled during surgical harvest to maximize the excursion of the sternal head.
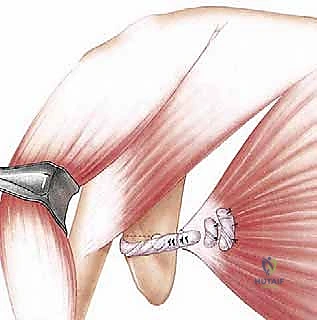
The sternal head is specifically selected for this transfer due to a confluence of favorable biomechanical properties. First, its mass and contractile power closely approximate those of the paralyzed serratus anterior. Second, when detached from the humerus and mobilized, it possesses excellent excursion. Third, and most importantly, when the sternal head tendon is augmented with a fascial graft and routed inferiorly to the inferior angle of the scapula, its vector of pull perfectly mimics the protracting and upwardly rotating action of the inferior division of the serratus anterior.
Neurovascular Structures at Risk
Mobilization of the pectoralis major sternal head necessitates meticulous dissection within the axilla, placing several critical neurovascular structures at risk. Deep to the pectoralis major lies the clavipectoral fascia, which encases the pectoralis minor and protects the underlying axillary artery, axillary vein, and the cords of the brachial plexus. Aggressive blind dissection in this region can lead to catastrophic vascular injury or irreversible plexopathy.
The innervation to the pectoralis major is supplied by the medial and lateral pectoral nerves. The lateral pectoral nerve (C5-C7) primarily innervates the clavicular head and the superior aspect of the sternal head. The medial pectoral nerve (C8-T1) pierces the pectoralis minor (or passes around its lateral border) to innervate the inferior aspect of the sternal head. During mobilization of the sternal head, the surgeon must identify and protect the medial pectoral nerve to ensure the transferred muscle remains viable and contractile. While distal arborizations may occasionally be sacrificed to achieve adequate excursion, the main trunk must be preserved.
Additionally, the long head of the biceps tendon resides within the bicipital groove, immediately deep to the insertion of the pectoralis major. When sharply releasing the sternal head tendon from the humerus, the surgeon must exercise extreme caution to avoid lacerating the biceps tendon or destabilizing its retinacular sheath. Finally, the cephalic vein, residing within the deltopectoral interval, must be carefully mobilized and retracted laterally to prevent avulsion or thrombosis during the initial exposure.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of a successful pectoralis major transfer. This procedure is not indicated for acute injuries, as the natural history of LTN neurapraxia is characterized by a high rate of spontaneous recovery. Surgical intervention is strictly reserved for chronic, refractory cases that have exhausted nonoperative modalities.
Patient Selection Criteria
The ideal candidate is a patient with isolated, symptomatic long thoracic nerve palsy who has undergone a minimum of 12 to 24 months of dedicated conservative management. This nonoperative phase must include aggressive physical therapy focused on maintaining passive glenohumeral range of motion to prevent adhesive capsulitis, as well as strengthening of compensatory periscapular stabilizers.
Serial EMG/NCV studies are mandatory. Surgery is indicated when these studies demonstrate a plateau in recovery, characterized by persistent denervation potentials and a lack of motor unit recruitment in the serratus anterior at the 1-to-2-year mark. Furthermore, the patient must demonstrate a positive scapular stabilization test preoperatively; if manual stabilization of the scapula fails to improve forward elevation, the surgeon must suspect concomitant glenohumeral pathology (e.g., massive rotator cuff tear, severe adhesive capsulitis) that will compromise the outcome of the transfer.
Table of Indications and Contraindications
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Absolute Indications | Symptomatic LTN palsy > 12-24 months | Allows adequate time for spontaneous neural recovery. |
| Failed conservative management | PT and bracing have not yielded functional improvement. | |
| EMG confirming persistent denervation | Objective evidence of irreversible muscle paralysis. | |
| Positive scapular stabilization test | Confirms that stabilizing the scapula will restore shoulder kinematics. | |
| Relative Indications | Pain refractory to non-op management | Severe periscapular spasm and impingement pain. |
| Severe occupational/ADL impairment | Inability to perform overhead work or basic daily tasks. | |
| Absolute Contraindications | Fixed scapulothoracic contracture | A stiff scapula cannot be dynamically mobilized by a transfer. |
| Global brachial plexopathy | Lack of functional donor muscles (pectoralis major must be 5/5 strength). | |
| Concomitant severe glenohumeral arthritis | Transfer will not restore motion if the primary joint is destroyed. | |
| Active infection | Standard surgical contraindication. | |
| Relative Contraindications | Medical non-compliance | Postoperative rehabilitation is rigorous and mandatory. |
| Advanced age with low functional demand | The extensive surgery and rehab may outweigh the benefits. | |
| Fascioscapulohumeral dystrophy (FSHD) | Progressive muscle disease may eventually affect the donor muscle; fusion is often preferred. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is essential to navigate the complexities of this dual-incision procedure. The surgeon must anticipate the required length of the graft, select the appropriate donor tissue, and position the patient to allow simultaneous access to the anterior chest and posterior scapula.
Graft Selection and Preparation
Because the native sternal head tendon of the pectoralis major lacks sufficient length to reach the inferior angle of the scapula, an intercalary graft is mandatory. The surgeon must engage in a detailed preoperative discussion with the patient regarding the choice between autograft and allograft tissues.
Autograft options typically include a strip of fascia lata or the semitendinosus/gracilis tendons harvested from the ipsilateral or contralateral lower extremity. Autograft remains the gold standard due to its superior biological integration, rapid incorporation, and elimination of disease transmission risk. Fascia lata provides a broad, robust sheet that is excellent for tubularization and weaving. However, autograft harvest extends operative time and introduces donor site morbidity, including pain, hematoma, and potential muscle herniation.
Alternatively, structural allografts (such as an Achilles tendon allograft or a robust semitendinosus allograft) offer an elegant solution that eliminates donor site morbidity and reduces tourniquet time. Modern sterilization techniques have rendered the risk of disease transmission negligible. For the pectoralis major transfer, a thick, high-quality allograft is highly effective, provided it is meticulously woven into the native tendon and securely fixated to the scapula. The choice ultimately depends on patient preference, surgeon experience, and graft availability.
Anesthesia, Positioning, and Draping
The procedure is typically performed under general anesthesia, often supplemented with a regional interscalene block for postoperative pain control. Muscle relaxants should be used judiciously, and their effects must be fully reversed prior to tensioning the graft to ensure accurate assessment of the resting muscle tone.
Patient positioning is critical. The lateral decubitus position is universally preferred. The patient is placed in the lateral decubitus position on a beanbag, leaning slightly posteriorly (approximately 20 to 30 degrees). This "sloppy lateral" position provides simultaneous, unhindered access to both the anterior deltopectoral interval and the posterior scapulothoracic articulation without the need for intraoperative repositioning.
The operative arm is draped free to allow for full manipulation throughout the procedure. An arm holder (such as a Spider or Trimble positioner) can be utilized to maintain the arm in varying degrees of abduction and external rotation during the anterior dissection, and forward flexion during the posterior tunneling phase. All bony prominences must be meticulously padded, and an axillary roll placed to protect the contralateral brachial plexus.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the pectoralis major transfer is a masterclass in tissue handling, neurovascular preservation, and biomechanical tensioning. The procedure is divided into three distinct phases: anterior mobilization, posterior preparation, and graft passage/fixation.
Anterior Exposure and Pectoralis Major Mobilization
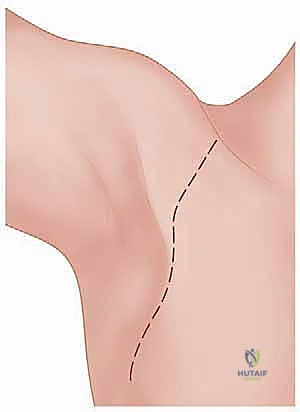
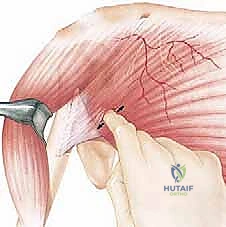
The operation commences with a standard anterior deltopectoral approach. An incision is made from the tip of the coracoid process extending distally toward the deltoid tuberosity. The cephalic vein is identified within the deltopectoral interval and typically retracted laterally with the deltoid muscle. The clavipectoral fascia is incised, exposing the insertion of the pectoralis major.
The surgeon must meticulously delineate the superior clavicular head from the inferior sternal head. A natural fat stripe often marks this interval. Blunt dissection is used to separate the two heads. The twisted insertion of the sternal head, which lies deep and proximal to the clavicular head, is identified.
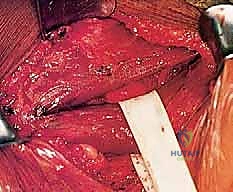
Using a right-angle clamp, the sternal head tendon is isolated, ensuring the long head of the biceps tendon is protected deep to the insertion. The sternal head tendon is sharply detached from the humerus as close to the bone as possible to maximize length. Heavy non-absorbable traction sutures (e.g., #2 FiberWire) are placed into the free edge of the tendon using a Krackow or locking whipstitch technique.
The critical step of mobilization follows. The sternal head must be freed from its fascial attachments to the chest wall to allow sufficient excursion toward the axilla. Using blunt finger dissection and careful electrocautery, the deep surface of the muscle is mobilized off the clavipectoral fascia. The surgeon must identify and preserve the medial pectoral nerve, which enters the deep surface of the muscle belly. Once mobilized, the chosen graft (autograft or allograft) is securely woven into the native sternal head tendon using a Pulvertaft weave technique, augmented with multiple interrupted non-absorbable sutures to create a biomechanically robust construct.
Posterior Exposure and Scapular Preparation
Attention is then directed posteriorly. A longitudinal or slightly oblique incision is made directly over the inferior angle of the scapula. The dissection is carried down through the subcutaneous tissue to expose the latissimus dorsi and the lower fibers of the trapezius.

The inferior angle of the scapula is identified within the triangle of auscultation. The fascial attachments of the latissimus dorsi and the paralyzed serratus anterior are elevated from the inferior angle using electrocautery. The bony surface of the inferior angle is aggressively decorticated using a burr or rongeur to create a bleeding cancellous bed, which is essential for robust tendon-to-bone healing.
Two or three transosseous drill holes are created through the inferior angle of the scapula. Alternatively, modern biocomposite or metallic suture anchors heavily loaded with high-tensile suture can be placed into the dense bone of the inferior angle. The preparation must be meticulous to prevent hardware pullout during the critical early rehabilitation phase.
Graft Passage, Tensioning, and Fixation
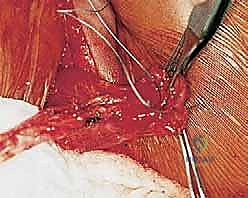
The most technically demanding phase of the procedure is the creation of the subcutaneous tunnel and the passage of the graft. A large, curved Kelly clamp or a specialized tendon passer is introduced from the posterior incision, directed deep to the latissimus dorsi, and advanced anteriorly through the axilla to emerge in the deltopectoral wound.

The surgeon must ensure the tunnel is wide enough to accommodate the bulky muscle-graft construct without constriction. The tunnel must pass superficial to the neurovascular bundle of the axilla to avoid catastrophic compression. The traction sutures attached to the graft are grasped, and the graft is smoothly pulled from anterior to posterior, emerging at the inferior angle of the scapula.
Tensioning the graft is the crux of the operation. The arm is positioned in approximately 30 degrees of abduction and 20 degrees of forward flexion. The scapula is manually pushed anteriorly and laterally against the chest wall to perfectly simulate the fully protracted, corrected position. With the scapula held in this anatomic position, the graft is pulled under maximal physiological tension.
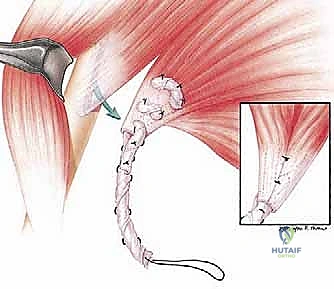
While maintaining this tension, the graft is secured to the decorticated inferior angle using the previously placed transosseous sutures or suture anchors. The fixation must be absolutely rigid. Once secured, the arm is gently taken through a limited range of motion to confirm that the scapula remains tightly apposed to the thoracic wall and that the graft tracks smoothly without impingement. The wounds are irrigated and closed in layers, and the patient is immediately placed into a specialized shoulder immobilizer.
Complications, Incidence Rates, and Salvage Management
While the pectoralis major transfer is highly effective, it is a major reconstructive procedure fraught with potential complications. Surgeons must be well-versed in the identification, prevention, and management of these adverse events.
Intraoperative and Postoperative Risks
Intraoperative neurovascular injury is the most devastating complication. Aggressive dissection deep to the pectoralis minor or an improperly routed axillary tunnel can result in injury to the axillary artery, vein, or the cords of the brachial plexus. The medial pectoral nerve is particularly vulnerable during the mobilization of the sternal head; denervation of the transfer renders the procedure entirely futile.
Postoperatively, hematoma formation in the large anterior dead space is a significant risk. Meticulous hemostasis and the liberal use of closed suction drains are mandatory. Infection, though relatively rare (<2%), can be catastrophic, potentially necessitating the removal of allograft tissue and leading to total failure of the reconstruction.
The most common mechanical complication is graft elongation or catastrophic rupture at the repair site. This typically occurs due to patient non-compliance during the early postoperative phase or inadequate initial fixation. Rupture presents as a sudden recurrence of severe winging and a popping sensation. Early recognition is critical, as prompt surgical revision and re-tensioning can salvage the outcome. If the transfer fails chronically due to stretching or muscle fibrosis, the surgical options become severely limited, often necessitating a salvage scapulothoracic fusion.
Table of Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention | Salvage / Management Strategy |
|---|---|---|---|
| Graft Rupture/Pullout | 5 - 10% | Rigid transosseous fixation; strict adherence to post-op immobilization. | Immediate surgical re-exploration, re-tensioning, and augmented fixation. |
| Hematoma Formation | 3 - 8% | Meticulous electrocautery; placement of large-bore closed suction drains. | Evacuation if compressive or expanding; antibiotics to prevent secondary infection. |
| Medial Pectoral Nerve Injury | < 2% | Careful identification and preservation during deep mobilization of sternal head. | Irreversible. May require a secondary transfer (e.g., Eden-Lange) or scapulothoracic fusion. |
| Infection (Deep) | 1 - 2% | Preoperative antibiotics; meticulous sterile technique; copious irrigation. | Surgical debridement, removal of allograft (if used), |
Clinical & Radiographic Imaging Archive
