Pediatric Forearm Shaft Fractures: Flexible Intramedullary Nailing Masterclass

Key Takeaway
This masterclass provides an exhaustive, real-time guide to flexible intramedullary nailing for pediatric forearm shaft fractures. We cover essential anatomy, meticulous preoperative planning, and a granular, step-by-step intraoperative execution from a surgeon's perspective. Fellows will learn precise techniques, critical pearls, potential pitfalls, and comprehensive postoperative management protocols for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Pediatric forearm shaft fractures represent a ubiquitous challenge within the realm of orthopedic trauma, accounting for a substantial proportion of all pediatric fractures evaluated in emergency departments worldwide. Historically, the pendulum of management swung heavily toward non-operative modalities, relying on the remarkable remodeling potential of the immature skeleton. However, contemporary pediatric orthopedics has witnessed a paradigm shift. While closed reduction and cast immobilization remain the gold standard for many of these injuries, a significant and clinically critical subset of patients demands operative intervention. This evolution is driven by a deeper understanding of forearm kinematics, the recognition of the limits of skeletal remodeling in older children, and the advent of refined surgical techniques such as flexible intramedullary nailing.
The epidemiology of these fractures reveals a bimodal distribution, with peaks occurring during early childhood and early adolescence, corresponding to periods of increased physical activity and sports participation. The mechanism of injury is classically an indirect force transmitted through the hand during a fall on an outstretched arm (FOOSH), though direct trauma can also occur. The energy of the injury, the position of the forearm at the moment of impact, and the inherent bone quality all dictate the resulting fracture pattern. We frequently encounter a spectrum ranging from plastic deformation and greenstick fractures to completely displaced and comminuted both-bone injuries. Understanding this spectrum is vital, as the management algorithm hinges upon accurate classification and an appreciation of the specific biomechanical disruption.
Flexible intramedullary nailing, often referred to as elastic stable intramedullary nailing (ESIN), has emerged as the premier surgical technique for displaced pediatric forearm shaft fractures. This masterclass will dissect the nuances of this procedure. ESIN operates on the principle of three-point fixation, where the inherent elasticity of the contoured titanium or stainless steel nails provides a dynamic, internal splint. This construct not only maintains length and alignment but also allows for micromotion at the fracture site, thereby promoting robust secondary bone healing via callus formation. The minimally invasive nature of the procedure preserves the fracture hematoma and the periosteal blood supply, which are critical elements for rapid osteogenesis.
The transition from non-operative to operative management must be a calculated decision, heavily influenced by patient age, fracture location, and the degree of displacement. As children approach skeletal maturity, their capacity for spontaneous correction of angular and rotational deformities diminishes precipitously. Therefore, the threshold for surgical intervention lowers in adolescents. The goal of this definitive guide is to equip the orthopedic surgeon with a comprehensive, step-by-step methodology for executing flexible intramedullary nailing, ensuring optimal functional outcomes while minimizing iatrogenic complications. We will explore the intricate anatomy, precise preoperative planning, meticulous surgical execution, and evidence-based rehabilitation protocols that define mastery in this domain.
Detailed Surgical Anatomy and Biomechanics
Osteology and Kinematics
A profound understanding of pediatric forearm osteology and its unique physiological responses is paramount before any surgical intervention is considered. The forearm functions as a highly complex, largely nonsynovial two-bone joint, boasting an impressive 180-degree range of motion in pronation and supination. This rotational capacity is absolutely critical for daily function, allowing the hand to be positioned optimally in space. The radial diaphysis extends from the most proximal aspect of the tubercle of Lister distally to the proximal base of the bicipital tuberosity proximally. The ulnar diaphysis corresponds to these exact same anatomical landmarks on the medial aspect of the forearm.

In the unfractured, native state, the relationship between the radius and ulna is not perfectly parallel. The radial styloid and bicipital tuberosity maintain an orientation slightly less than 180 degrees, while the ulnar styloid and coronoid process are closer to a true 180-degree relationship. This inherent "bow" of the radius, curving naturally out and away from the relatively straight ulna in the supinated anteroposterior plane, is the biomechanical linchpin for pronation and supination. Maintenance of this radial bow, and consequently the interosseous space, is vital for preserving forearm kinematics. Any loss of this bow, whether through malunion or improper surgical contouring, directly translates to a mechanical block in rotation.
The interosseous membrane (IOM) further complicates the structural integrity of the forearm. This robust ligamentous complex not only binds the radius and ulna together but also serves as a critical load-sharing mechanism, transferring forces from the distal radius to the proximal ulna. Disruption of the IOM, often seen in high-energy both-bone fractures or fracture-dislocations (such as Galeazzi or Monteggia variants), destabilizes the entire forearm axis. Surgical restoration must account for the tensioning of the IOM, which is optimally achieved when both bones are restored to their anatomic length and alignment.
Muscular Deforming Forces
Forearm shaft fractures are classically categorized into three distinct anatomical regions, each governed by specific deforming muscular forces that dictate the predictable patterns of displacement. Understanding these forces is essential for executing a successful closed reduction and for maintaining that reduction during intramedullary nail passage. The distal third of the forearm is dominated by the pronator quadratus. Fractures in this region typically result in the distal fragment being drawn into severe pronation and dorsal angulation, necessitating supination and volar directed pressure during reduction maneuvers.

The central third of the diaphysis is heavily influenced by the pronator teres, which inserts on the lateral convexity of the mid-radius. Fractures occurring proximal to this insertion leave the proximal fragment relatively supinated by the biceps and supinator, while the distal fragment is forcefully pronated by the pronator teres and pronator quadratus. This creates a severe rotational mismatch that must be carefully addressed. Conversely, fractures distal to the pronator teres insertion result in both the proximal and distal fragments being subjected to pronating forces, altering the required reduction vectors.
The proximal third of the forearm presents the most challenging reduction scenarios due to the unopposed action of the powerful supinators. The biceps brachii and the supinator muscle forcefully externally rotate and flex the proximal fragment. Meanwhile, the distal fragment is pronated by the combined forces of the pronator teres and pronator quadratus. Consequently, proximal third fractures often demand that the distal fragment be brought into profound supination to match the unyielding position of the proximal segment, a maneuver that can be technically demanding and requires meticulous fluoroscopic verification.
Neurovascular Topography
The forearm is a dense, highly specialized neurovascular corridor, and surgical navigation requires an intimate knowledge of its topography to avoid catastrophic iatrogenic injury. The arterial supply is robust, primarily driven by the brachial artery bifurcating into the radial and ulnar arteries. Preoperative and postoperative assessment of radial and ulnar pulses, alongside distal capillary refill, is a non-negotiable standard of care. Tense swelling in the setting of arterial compromise must immediately raise the suspicion for compartment syndrome, a surgical emergency.
The median nerve courses centrally down the volar forearm. Its motor branch, the anterior interosseous nerve (AIN), is of particular clinical significance. The AIN innervates the flexor pollicis longus, the pronator quadratus, and the radial half of the flexor digitorum profundus. Injury to the AIN manifests as an inability to form the "okay" sign (loss of IP flexion of the thumb and DIP flexion of the index finger). The median nerve itself is the most commonly injured nerve following both closed and open forearm shaft fractures due to its tethering and central location.
The ulnar nerve runs medially, protected by the flexor carpi ulnaris. Its motor function is critically tested by assessing the adduction of the thumb and the flexion of the ring and small fingers via the FDP. The autonomous sensory zone is the palmar tip of the small finger. Crucially, the ulnar nerve is the most frequent victim of iatrogenic injury during internal fixation, particularly during proximal ulnar approaches or when establishing the entry point for the ulnar intramedullary nail. The radial nerve divides into the posterior interosseous nerve (PIN) and the superficial radial nerve (SRN). The PIN is highly vulnerable during proximal radial exposures, while the SRN, providing sensation to the dorsal web space, is at extreme risk during the establishment of the distal radial entry point for ESIN.
Pediatric Remodeling Potential
The pediatric skeleton possesses a remarkable, yet finite, capacity for remodeling, a physiological phenomenon governed by precise biomechanical laws. The Hueter-Volkmann Law dictates that physeal orientation tends to "right its horizon" in response to altered mechanical loading. This means that angular deformities situated close to the growth plates and in the plane of joint motion have a high probability of spontaneous correction over time. Conversely, deformities in the middle of the diaphysis or those perpendicular to the plane of motion remodel poorly.
Wolff's Law further explains that true diaphyseal shaft remodeling occurs via bone adaptation to mechanical stress; bone is deposited where it is needed and resorbed where it is not. In the growing child, normal longitudinal growth from adjacent physes also contributes to the production of "straight bone" over time, gradually masking diaphyseal malunions. However, this biological safety net is not absolute.
This remodeling potential is most predictable and robust in children under the age of 8 to 10 years. As a child approaches adolescence, the remaining growth potential diminishes, and the tolerance for angular and rotational malalignment drops precipitously. Older children, and those presenting with complete, widely displaced fractures, have much stricter limits for acceptable displacement. Rotational malalignment, in particular, remodels exceptionally poorly at any age and must be anatomically corrected during surgical intervention to prevent permanent deficits in pronation and supination.
Exhaustive Indications and Contraindications
The decision to proceed with flexible intramedullary nailing in pediatric forearm fractures requires a nuanced synthesis of patient demographics, fracture morphology, and the limitations of conservative care. While closed reduction and casting remain the initial treatment for the vast majority of these injuries, surgical intervention is mandated when conservative measures fail to achieve or maintain an acceptable reduction, or when the fracture pattern inherently predicts a high rate of failure.
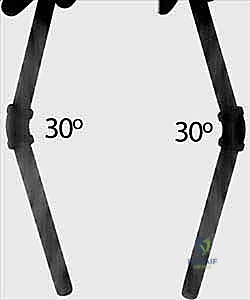
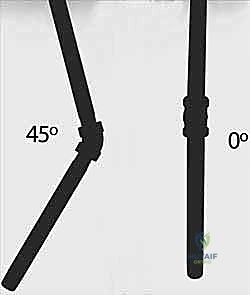
Age-dependent angulation limits are the primary drivers for surgical decision-making. In children under 8 to 10 years of age, greater than 20 degrees of angulation in the distal third, greater than 15 degrees in the central third, and greater than 10 degrees in the proximal third are generally unacceptable. For children over 10 years of age, the tolerance is much lower; generally, no more than 10 degrees of angulation is acceptable at any level due to the diminished remodeling potential. Furthermore, rotational malalignment exceeding 30 to 45 degrees is an absolute indication for correction, as it will not remodel and will result in a permanent mechanical block.
Flexible IM nailing is particularly suited for displaced complete fractures, even those with minor comminution (where butterfly fragments constitute less than 25% of the shaft diameter). It is the treatment of choice for unstable patterns that slip in the cast, open fractures requiring soft tissue management, and cases involving multiple extremity traumas where early mobilization is necessary. However, strict contraindications exist. Active infection at the surgical site is an absolute contraindication. Relative contraindications include severe comminution (which may lack the cortical contact necessary for ESIN stability, pushing the surgeon toward plate osteosynthesis) and fractures located too proximally or distally in the metaphysis, where the intramedullary nails cannot achieve adequate purchase.
| Category | Indications for Flexible IM Nailing | Contraindications for Flexible IM Nailing |
|---|---|---|
| Absolute | - Failure to achieve/maintain closed reduction within acceptable age-based parameters. - Open fractures (Gustilo-Anderson Types I, II, IIIA). - Polytrauma patients requiring early mobilization. - Pathologic fractures (depending on etiology). - Rotational malalignment > 45 degrees. |
- Active localized or systemic infection. - Fractures with intra-articular extension requiring anatomic reduction. - Extreme metaphyseal fractures lacking sufficient diaphyseal canal for nail purchase. |
| Relative | - Floating elbow (ipsilateral supracondylar humerus and forearm fracture). - Re-fractures with significant displacement. - Galeazzi or Monteggia fracture-dislocations (though ESIN is often used, plating may be preferred in older adolescents). |
- Severe comminution (>25% shaft diameter) lacking cortical contact for stability (plating preferred). - Older adolescents nearing skeletal maturity with narrow canals. - Weight > 50kg (increased risk of nail bending/failure, though not a strict cutoff). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Radiographic Analysis
Success in the operating theater is inextricably linked to meticulous preoperative preparation. The clinical evaluation must begin with a detailed history, focusing on the mechanism of injury. Understanding whether the injury resulted from a low-energy fall or a high-energy trauma (e.g., motor vehicle accident, fall from significant height) helps predict the severity of soft tissue damage and the likelihood of associated injuries. A comprehensive physical examination is mandatory, with particular attention paid to ruling out concomitant injuries to the ipsilateral wrist, elbow, and shoulder girdle.
The neurovascular examination must be exhaustive and documented clearly before any intervention. Motor function is assessed using the "rock-paper-scissors" method to isolate the radial, median, and ulnar nerves. The skin must be inspected circumferentially; any wound, no matter how diminutive, in the proximity of the fracture must be treated as an open fracture until proven otherwise. Furthermore, the surgeon must maintain a high index of suspicion for acute compartment syndrome. Tense, unyielding forearm swelling, pain out of proportion to the injury, and pain with passive stretch of the digits are ominous signs that require immediate attention and potentially emergent fasciotomy.
Radiographic analysis requires high-quality, orthogonal anteroposterior (AP) and lateral views of the entire forearm, strictly encompassing both the wrist and elbow joints. This is critical to rule out subtle Galeazzi or Monteggia variants. The surgeon must carefully assess the fracture level, pattern, and degree of displacement. A critical radiographic pearl to remember is that if angulation is present on both orthogonal views, the true magnitude of the angulation in the oblique plane is mathematically greater than what is measured on either individual two-dimensional radiograph.
Preoperative Templating and Implant Selection
Preoperative templating is a non-negotiable step in the surgical workflow. Using the pre-injury or initial injury radiographs, the surgeon must measure the narrowest canal diameter of both the radius (typically located in the midshaft) and the ulna (typically in the distal third). The goal is to select an intramedullary nail diameter that occupies approximately 40% of the narrowest canal diameter.
Crucially, we typically utilize the exact same-sized nail in both the radius and the ulna to ensure symmetrical biomechanical forces and prevent iatrogenic shifting of the fracture fragments. Implants measuring 2.0 mm, 2.5 mm, and occasionally 3.0 mm in diameter are the most commonly employed. It is a fundamental tenet of ESIN that it is far worse to select implants that are too large rather than slightly too small. Oversized nails can become incarcerated in the diaphysis, causing iatrogenic comminution, propagation of the fracture, or immense difficulty during both insertion and eventual hardware removal.
In addition to nail sizing, the surgeon must estimate the degree of rotational malalignment from the radiographs by assessing the cortical widths and the profile of the bicipital tuberosity relative to the radial styloid. The soft tissue envelope must also be factored into the implant selection; in cases of severe swelling, the approach and entry points may need to be slightly modified to avoid excessive tension on the skin edges during closure.
Operating Room Setup and Patient Positioning
The choreography of the operating room setup is designed to maximize surgical efficiency and fluoroscopic visualization. The patient is placed in a supine position on the operating table. The involved extremity is carefully extended and positioned on a sturdy, completely radiolucent hand table. This hand table is the physical foundation of the procedure; it must allow for easy, unobstructed C-arm visualization of the entire forearm, from the olecranon to the carpus, in both AP and lateral planes without requiring awkward manipulation of the patient's shoulder.

The C-arm fluoroscopy unit is positioned on the side of the table opposite the operative arm, allowing the C-arm to swing freely in a 90-degree arc to obtain orthogonal views rapidly. The primary fluoroscopy monitor should be placed near the foot of the operating table, directly in the surgeon's line of sight, ensuring that the surgical team does not have to turn their heads away from the sterile field to view the images.
A nonsterile pneumatic tourniquet is applied high on the upper arm, near the axilla, prior to the sterile prep. While we do not routinely inflate the tourniquet for closed reduction and percutaneous nailing, it serves as a critical safety contingency should an open reduction become necessary due to soft tissue interposition or intractable bleeding. The sterile preparation must encompass the entire arm from the fingertips to the tourniquet. Draping is executed with a sterile, impervious U-drape as the base layer. A critical technical pearl is the application of an additional sterile skirt (a sterile paper half-sheet) draped over the C-arm receiver and the proximal aspect of the hand table. This creates a vastly expanded sterile field, preventing inadvertent contamination during the dynamic maneuvers required for fracture reduction and nail insertion.

Step-by-Step Surgical Approach and Fixation Technique
Surgical Approach and Entry Point Preparation
The procedure commences with the establishment of precise entry points, a step that dictates the trajectory of the nails and the ultimate success of the fixation. We typically address the easier fracture first—usually the ulna—to stabilize the forearm segment before tackling the more complex radial reduction. For the ulna, a small 1-2 cm longitudinal incision is made over the lateral aspect of the proximal ulna, approximately 1-2 cm distal to the olecranon apophysis. Blunt dissection is utilized down to the periosteum to avoid injury to the ulnar nerve, which lies medially.
An awl or a drill bit (slightly larger than the selected nail diameter) is used to breach the near cortex. The entry angle is critical; it must begin perpendicular to the bone to prevent skiving, then gradually angle to approximately 45 degrees relative to the shaft axis to facilitate smooth nail passage into the medullary canal.
For the radius, the entry point is established distally. A similar 1-2 cm incision is made over the lateral aspect of the distal radius, proximal to the distal radial physis. Extreme caution must be exercised here to identify and protect the superficial branch of the radial nerve (SRN), which courses directly through this operative field.

The awl is introduced just proximal to the physis, again starting perpendicular and angling proximally.

Prior to insertion, the titanium nails must be meticulously contoured. The radial nail is pre-bent to recreate the normal anatomical radial bow. The apex of the bend should correspond to the location of the fracture to maximize the three-point fixation biomechanics. The ulnar nail is left relatively straight or given a very mild curve to match the native ulnar anatomy.

Fracture Reduction and Nail Advancement
With the entry portals established, the ulnar nail is introduced first. The nail is mounted on a T-handle and advanced manually with oscillating, twisting motions. Hammering should be avoided if possible, as it increases the risk of cortical perforation or iatrogenic fracture.

The nail is advanced to the level of the fracture site. At this juncture, closed reduction is performed. Traction, counter-traction, and precise manipulation based on the deforming muscular forces (as discussed in the anatomy section) are utilized to align the fragments.

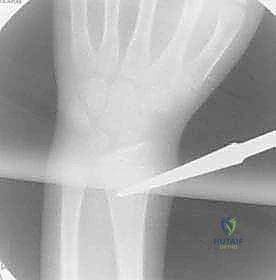
Fluoroscopy is essential here. Once the fracture is aligned, the nail is carefully advanced across the fracture site and seated into the distal ulnar metaphysis.

If closed reduction is impossible due to soft tissue interposition (often periosteum or muscle), an F-tool can be used percutaneously to manipulate the fragments.
If this fails, a small, limited open reduction at the fracture site is mandated. There is no clinical benefit to prolonged, traumatic closed reduction attempts when a 2 cm incision can quickly and safely resolve the obstruction.

Attention then turns to the radius. The contoured radial nail is inserted distally and advanced to the fracture.

The radial reduction is often more challenging due to the rotational forces. The surgeon must ensure the radial bow is perfectly restored.

The nail is passed across the fracture site under live fluoroscopy.

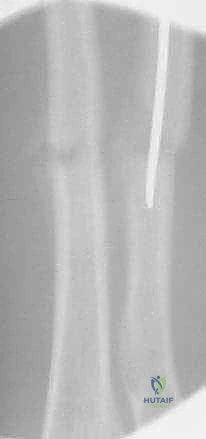
The tip of the radial nail should be driven into the proximal radial metaphysis, ideally stopping just short of the proximal physis to avoid growth arrest.

Throughout this process, the surgeon must continuously verify fracture alignment, nail trajectory, and the restoration of the interosseous space on both AP and lateral fluoroscopic views.
Final Positioning and Wound Closure
Once both nails successfully traverse their respective fracture sites and are embedded in the opposing metaphyses, final adjustments are made. The surgeon rotates the nails slightly to maximize the tensioning of the interosseous membrane and lock the fractures into their anatomical positions.

The C-arm is used to confirm the final reduction, ensuring that length, alignment, and rotation are completely restored.


The next critical step is cutting the nails. The nails must be cut leaving approximately 1.0 to 1.5 cm protruding from the entry cortex.
This length is crucial; it must be long enough to allow for easy grasping during future hardware removal, but short enough to avoid excessive prominence beneath the skin, which is the leading cause of postoperative pain and bursitis.

The protruding ends can be slightly bent away from the skin to minimize irritation.

The surgical sites are copiously irrigated with sterile saline. The deep fascial layers are generally not closed to prevent localized compartment syndrome. The subcutaneous tissues are approximated with absorbable sutures, and the skin is closed with a running subcuticular stitch or simple interrupted sutures.

Final, static orthogonal radiographs are obtained to document the surgical outcome.

The limb is then cleansed, and sterile dressings are applied.

