Pediatric Limb Salvage: Expandable Endoprosthesis Implantation Masterclass
Key Takeaway
Join us in the OR for a detailed masterclass on expandable endoprosthesis implantation in pediatric limb salvage. We'll cover indications, meticulous preoperative planning, precise anatomical considerations, and step-by-step intraoperative execution for common sites like the distal femur. Learn critical pearls, pitfalls, and comprehensive postoperative management to ensure optimal outcomes for our young patients requiring limb length maintenance.
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues, fellows, and residents, to the operating theater and the rigorous academic study of orthopaedic oncology. Today, we are tackling one of the most rewarding yet technically formidable challenges in our field: limb salvage in the immature skeleton utilizing expandable endoprostheses. This is a procedure that demands not only meticulous preoperative planning and precise intraoperative execution but also a profound, dynamic understanding of pediatric growth, biomechanics, and spatial anatomy. Our overarching goal transcends the mere excision of a malignant neoplasm; we are tasked with restoring durable biomechanical function and maintaining limb length equality in a growing child, thereby offering them the highest possible functional quality of life into adulthood.
The Evolution of Pediatric Limb Salvage
Historically, the diagnosis of a primary malignant bone tumor in a child, such as osteosarcoma or Ewing sarcoma, was a virtual mandate for amputation or rotationplasty. The paradigm shifted dramatically in the late 20th century with the advent of neoadjuvant multi-agent chemotherapy, which transformed these previously fatal diseases into survivable conditions. As five-year survival rates for localized disease climbed past seventy percent, the orthopaedic community was challenged to develop reconstructive techniques that could adapt to the growing skeleton. Early attempts with static adult-type prostheses inevitably led to severe limb length discrepancies (LLD), requiring complex, staged revision surgeries or resulting in unacceptable functional deficits. The conceptualization and subsequent engineering of the expandable endoprosthesis revolutionized our approach, allowing the implant to "grow" in tandem with the contralateral limb.
Patho-Epidemiology of Primary Bone Sarcomas
We primarily consider this sophisticated reconstructive approach for osteosarcoma and Ewing sarcoma, the two most ubiquitous primary malignant bone tumors in the pediatric demographic. These aggressive neoplasms disproportionately afflict children and adolescents during periods of rapid skeletal growth, with a significant percentage diagnosed before the age of sixteen, and a critical subset presenting before the age of twelve. Osteosarcoma typically arises in the metaphysis of long bones—most frequently the distal femur, proximal tibia, and proximal humerus—directly adjacent to the most active physes in the body. Ewing sarcoma, while often diaphyseal, can also involve metaphyseal regions and requires extensive resection margins. The remarkable advancements in targeted systemic therapies and refined surgical techniques over the past three decades have dramatically improved survival trajectories, even in the presence of limited pulmonary metastases. This improved oncologic prognosis unequivocally underscores the absolute necessity for durable, functional, and adaptable limb salvage solutions.
The Biomechanical Imperative of Expandable Implants
The deployment of an expandable endoprosthesis is not merely a geometric exercise in matching bone length; it is a complex biomechanical intervention. The growing skeleton is highly responsive to mechanical loading, governed by Wolff's Law. When a massive metallic implant is introduced, it alters the physiological stress distribution, leading to potential stress shielding, osteolysis, and implant loosening over time. Expandable prostheses must be engineered to mitigate these forces while housing an internal lengthening mechanism—whether mechanical (e.g., minimally invasive worm-drive) or non-invasive (e.g., electromagnetic induction). Furthermore, the fixation of these devices in the pediatric intramedullary canal, which is often narrow and structurally immature, requires specialized techniques, including the use of custom-fluted stems, hydroxyapatite-coated collars for extracortical bone bridging, and precise cementing techniques to ensure long-term survivorship of the construct.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the intricate, evolving anatomy of the growing skeleton is the non-negotiable foundation for safe and oncologically sound tumor resection and subsequent reconstruction. The pediatric musculoskeletal system is not simply a miniature adult system; it is a dynamic landscape of active physes, highly vascularized periosteum, and shifting muscular intervals.
Growth Plate (Physis) Physiology and Vascularity
During childhood and adolescence, the physis is a critically important, avascular cartilaginous structure strategically nestled between two vital, distinct vascular beds: the epiphyseal and metaphyseal circulations. The epiphyseal vessels supply oxygen and essential nutrients necessary for chondrocyte survival, proliferation, and matrix synthesis within the reserve and proliferative zones of the physis. Preserving this epiphyseal blood supply is absolutely critical if any remaining growth potential is to be salvaged following a joint-sparing, physeal-preserving tumor resection. Conversely, the metaphyseal vessels interact intimately with the hypertrophic zone chondrocytes, a process crucial for normal endochondral ossification and primary spongiosa formation.
Furthermore, the pediatric periosteum is exceptionally thick, highly active, and osteogenic. It is not merely a fibrous covering; it is a vital source of osteoprogenitor cells and contributes massively to appositional bone growth and fracture healing. During surgical exposure, excessive periosteal stripping must be meticulously avoided, especially near remaining growth plates, to maintain subsequent growth velocity and to facilitate critical bony ongrowth to the prosthesis, particularly around hydroxyapatite-coated collars designed to promote extracortical bridging.
Neurovascular Topography of the Distal Femur and Proximal Tibia
The distal femur represents the most common site for pediatric osteosarcoma (approximately 52% of cases). The surgical approach is typically anteromedial, often involving a medial parapatellar arthrotomy. The primary neurovascular structures at risk include the femoral artery and vein, which lie posteromedial to the femur within the adductor canal and must be rigorously protected during posterior dissection, especially when defining posterior tumor margins. The popliteal vessels, located posterior to the knee joint and deep to the gastrocnemius, demand extreme care during posterior capsular release.
For the proximal tibia (accounting for roughly 24% of cases), the anatomy is arguably more unforgiving. The popliteal artery trifurcates distally, and its branches are tethered by the soleal arch. The common peroneal nerve is highly vulnerable as it wraps around the fibular neck; it is susceptible to stretch neuropraxia or direct transection during lateral exposure or aggressive retraction. We must meticulously identify, neurolyse, and protect this nerve early in the dissection. The muscular intervals for both regions require reflection of the extensor mechanism. Preservation of the quadriceps mechanism, patellar tendon, and the pes anserinus insertion is crucial for restoring dynamic knee stability and active extension post-reconstruction.
Upper Extremity and Proximal Femoral Considerations
In the proximal humerus (10% of cases), we utilize the expansile approach of Henry, exploiting the deltopectoral interval. The axillary nerve is the structure at highest risk; it wraps around the surgical neck of the humerus deep to the deltoid and is highly vulnerable during superior, lateral, or posterior extra-articular dissection. The radial nerve, residing in the spiral groove posteriorly, is at risk during diaphyseal transection. Retraction of the deltoid superiorly and the pectoralis major medially provides access, but the neurovascular bundle in the axilla must be constantly palpated and protected.
For the proximal femur (6% of cases), a direct lateral approach (Watson-Jones or a modified Hardinge) is typically employed. The femoral artery and vein lie medial to the femur, safely away from the lateral approach, but the sciatic nerve, coursing posterior to the hip joint and deep to the gluteus maximus, is at significant risk during posterior capsular release or excessive anterior retraction of the femur. The superior gluteal nerve and vessels, which supply the critical abductor musculature (gluteus medius and minimus), are at risk during superior dissection or detachment of the gluteal muscles from the greater trochanter. Restoring abductor tension via secure reattachment to the prosthesis is paramount to preventing a debilitating postoperative Trendelenburg gait.
Exhaustive Indications and Contraindications
The decision to utilize an expandable endoprosthesis is highly nuanced, multi-factorial, and must be individualized to the patient. It is primarily driven by the patient's chronological and skeletal age, precise tumor location, anticipated physeal sacrifice, and the mathematically projected limb-length discrepancy at skeletal maturity.
Thresholds for Limb Length Discrepancy (LLD)
The core, absolute indication for an expandable prosthesis is the anticipated limb-length discrepancy at skeletal maturity. For the lower extremity, if the estimated leg-length discrepancy is calculated to be more than 3 cm, an expandable prosthesis is unequivocally indicated. Discrepancies exceeding 3 cm lead to severe pelvic obliquity, compensatory scoliosis, and significantly increased energy expenditure during ambulation. For projected discrepancies less than 3 cm, we might consider conventional "adult-type" prostheses, manufactured slightly longer (up to 1.5 cm) to over-lengthen the limb acutely, or we may opt for a contralateral epiphyseodesis to equalize limb lengths at maturity.
In the upper extremity, the functional tolerance for length discrepancy is significantly higher. The threshold for utilizing an expandable prosthesis in the arm is typically a projected discrepancy of more than 5 cm. If the discrepancy is less than 5 cm, we can frequently insert a conventional static prosthesis that is 2 to 3 cm longer than the resected segment, effectively allowing the contralateral, healthy limb to "catch up" during remaining growth. A slight arm-length discrepancy is predominantly a cosmetic concern, with true functional deficits in reach and bimanual activities arising only when the difference becomes massive.
Age, Chemotherapy, and Physeal Sacrifice
Bone tumors in children frequently occur in the metaphyseal region, directly adjacent to the most active growth plates (e.g., distal femur, proximal tibia). Achieving wide oncologic margins often necessitates the complete sacrifice of a major physis, leading to an immediate and profound growth arrest in that segment. Expandable prostheses are specifically designed to counteract this exact iatrogenic deficit. Furthermore, we must account for the systemic effects of neoadjuvant and adjuvant chemotherapy. Intensive cytotoxic regimens independently suppress global bone growth and delay skeletal maturation, further complicating LLD calculations and contributing to potential discrepancies.

Patient age and skeletal maturity are the final arbiters. Generally, females older than 11 years or males older than 13 years rarely require expandable prostheses. At these ages, the remaining growth potential of the affected physes usually translates to an estimated growth discrepancy of less than 3 cm. Utilizing an expandable implant in a patient nearing skeletal maturity exposes them to the mechanical risks of a complex device without the requisite benefit.
Tabular Breakdown of Indications and Contraindications
| Category | Indications for Expandable Endoprosthesis | Contraindications / Relative Contraindications |
|---|---|---|
| Patient Demographics | Skeletally immature (Males < 13 yrs, Females < 11 yrs); High functional demand. | Skeletally mature; Projected LLD < 3cm (Lower Ext) or < 5cm (Upper Ext). |
| Oncologic Factors | Primary bone sarcomas (Osteosarcoma, Ewing); Expected long-term survival; Resection requires physeal sacrifice. | Uncontrolled systemic metastasis with poor prognosis; Inability to achieve negative margins without amputation. |
| Anatomical Factors | Projected LLD > 3cm (Lower Extremity) or > 5cm (Upper Extremity). | Inadequate soft tissue coverage; Severe neurovascular encasement requiring resection of major bundles. |
| Medical/Systemic | Medically optimized; Adequate hematologic parameters post-chemotherapy. | Active local or systemic infection; Severe immunocompromise precluding major reconstruction. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous, obsessive preoperative planning is the cornerstone of a successful oncologic and functional outcome in pediatric limb salvage. This phase involves a comprehensive, multidisciplinary assessment of the tumor volume, the patient's exact growth potential, and the highly specific engineering requirements of the chosen reconstructive strategy.
Advanced Imaging and Skeletal Maturity Assessment
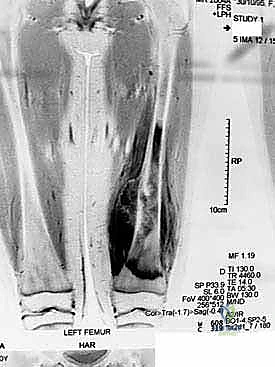
For any pediatric patient with a suspected or confirmed malignancy, an exhaustive staging imaging protocol is mandatory. Plain radiographs of the affected bone assess macroscopic bone destruction and periosteal reaction. Contrast-enhanced MRI of the entire affected bone is absolutely critical for defining intramedullary skip lesions and soft tissue tumor extension. The MRI dictates our planned level of bone transection, aiming for a minimum of 2-3 cm of normal marrow beyond the tumor extent. A high-resolution Chest CT is utilized to screen for pulmonary metastases, while an Isotope Bone Scan or PET-CT detects multifocal osseous disease.

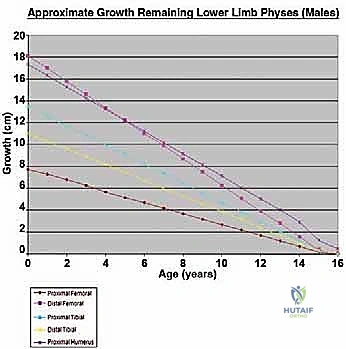
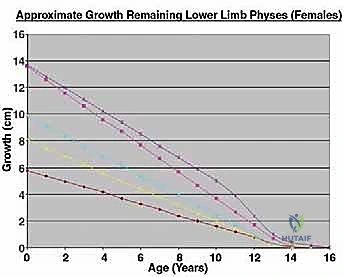
Beyond standard oncologic staging, we require specialized orthopaedic measurements. Measured full-length scanograms of both the affected and contralateral limbs are critical for calculating current limb length and templating the prosthesis. A standardized hand/wrist radiograph is obtained to estimate skeletal bone age using the Greulich and Pyle atlas. This provides a vastly more accurate prediction of remaining growth than chronological age alone. The Estimated Limb-Length Discrepancy (LLD) at skeletal maturity is then calculated. While traditionally derived using the Anderson and Green charts, the validated Multiplier Method has emerged as a highly accurate and simpler predictor, utilizing chronological age and a single length measurement to definitively determine if an expandable prosthesis is indicated.
Engineering Communication and Implant Selection
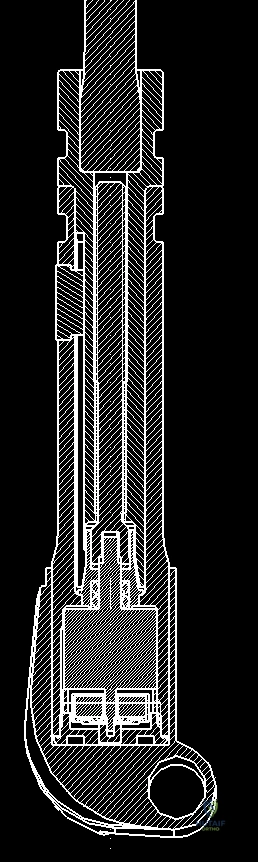
Once the resection level is determined, accurate measured radiographs and MRI cross-sections are transmitted to the prosthesis engineers. They will custom-fabricate or modularly assemble the implant to match the resected bone length precisely, accounting for the required joint line restoration and soft tissue tension. We currently utilize two main categories of expandable prostheses: minimally invasive (mechanical) and non-invasive (electromagnetic).

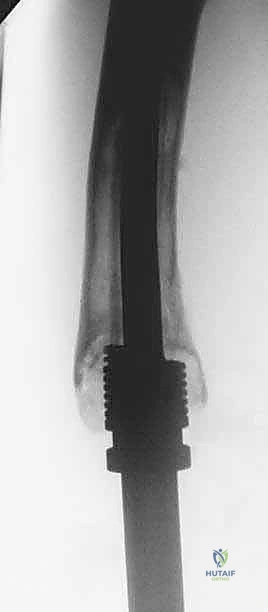
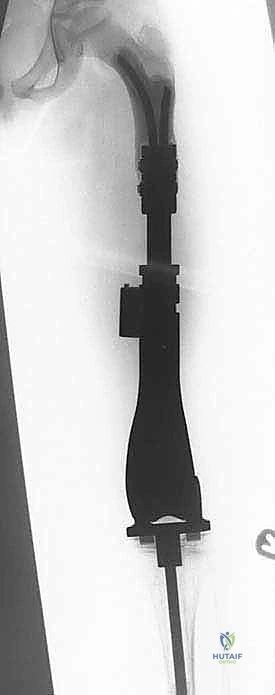
The Minimally Invasive Expandable Prosthesis (e.g., the JTS implant) is lengthened via an internal worm-drive mechanism. It requires a minor percutaneous procedure where an Allen key is inserted through a small stab incision to manually turn the mechanism. While highly reliable and mechanically robust, it carries a cumulative risk of infection with each lengthening procedure. Conversely, Non-invasive Expandable Prostheses (e.g., Repiphysis or Mutars Xpand) utilize an internal electromagnetic motor driven by an external magnetic coil placed over the limb in the outpatient clinic. This eliminates the need for repeated anesthesia and surgical incisions, drastically reducing the risk of secondary periprosthetic joint infection, though these devices are mechanically more complex and historically prone to internal mechanism failures.


Patient Optimization and Operative Setup
Prior to surgery, the patient must be rigorously optimized. We mandate a comprehensive screening for all potential infective foci, including a dental hygienist review, MRSA swabbing, and inspection of central venous catheter sites. Hematologic parameters must be sufficient to withstand major surgery, especially following neoadjuvant chemotherapy; our institutional protocol requires an absolute neutrophil count >1000/mm³ and a platelet count ≥75,000/mm³.
Patient positioning is critical. For distal femoral and proximal tibial resections, the patient is positioned supine on a radiolucent table. A sterile tourniquet may be applied high on the thigh, though it is often kept uninflated to allow for accurate assessment of tissue perfusion and hemostasis during the resection. The entire limb is prepped and draped free to allow full range of motion, which is essential for assessing joint kinematics and soft tissue tension during the trial reduction of the endoprosthesis.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a pediatric limb salvage procedure is a masterclass in anatomical precision, oncologic radicality, and biomechanical reconstruction. The procedure is conceptually divided into the extirpative phase (tumor resection) and the reconstructive phase (implant fixation and soft tissue coverage).
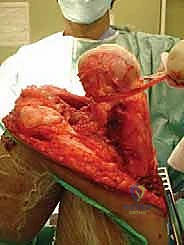
Exposure and Oncologic Resection
The incision is meticulously planned to incorporate the previous biopsy tract within an ellipse of skin, ensuring the tract is excised en bloc with the main tumor specimen to prevent local seeding. For a distal femoral resection, an extended anteromedial incision is utilized. Deep dissection proceeds through the virgin tissue planes, maintaining a thick cuff of normal muscle around the pseudocapsule of the tumor.

The neurovascular bundle (femoral/popliteal vessels) is identified proximally in the normal anatomy of the adductor canal and traced distally, carefully dissecting it away from the posterior aspect of the tumor block. Once the neurovascular structures are safeguarded and the joint capsule is appropriately addressed (often requiring intra-articular resection for distal femur, or extra-articular resection if the joint is contaminated), the level of the diaphyseal osteotomy is identified based on preoperative MRI measurements.

The osteotomy is performed using an oscillating saw under continuous saline irrigation to prevent thermal necrosis of the remaining bone. The entire tumor specimen is then delivered from the field and immediately sent for pathological evaluation of the margins.
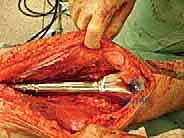
Canal Preparation and Implant Trialing
Following resection, the remaining host bone canal must be prepared. In pediatric patients, the intramedullary canal is often narrow, necessitating careful sequential reaming. We must balance the need for adequate implant stem diameter (for mechanical strength) against the risk of iatrogenic cortical perforation or fracture.


A trial prosthesis is assembled and inserted. This is a critical step to assess limb length, joint line restoration, and soft tissue tension. The knee (or relevant joint) is put through a full range of motion. We assess for patellar tracking, varus/valgus stability, and ensure there is no impingement of the expansion mechanism. If the soft tissues are excessively tight, a slightly shorter modular segment may be required; if too lax, a longer segment is chosen to ensure joint stability.


Definitive Fixation and Soft Tissue Reconstruction
Fixation in the pediatric skeleton is challenging. While press-fit, hydroxyapatite-coated stems are utilized to encourage biologic fixation and extracortical bone bridging, cemented stems remain the gold standard in many centers due to the immediate stability they provide in compromised, irradiated, or chemotherapy-affected bone.


If cementing, a cement restrictor is placed, the canal is pulsatile-lavaged and dried, and third-generation cementing techniques (vacuum mixing, retrograde injection) are employed. The definitive prosthesis is impacted into place, ensuring correct version.
The final, and arguably most crucial, step for functional recovery is the soft tissue reconstruction. The extensor mechanism must be meticulously reapproximated. In cases where significant local muscle was resected to achieve oncologic margins, rotational muscle flaps (such as a medial gastrocnemius flap for the proximal tibia) are frequently employed to provide robust, vascularized soft tissue coverage over the metallic implant, drastically reducing the risk of postoperative wound breakdown and deep infection.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced engineering, the implantation of a massive expandable endoprosthesis in a pediatric patient undergoing cytotoxic chemotherapy carries a formidable complication profile. We classify these failures broadly using the Henderson classification for tumor prostheses: Type 1 (Soft tissue failure), Type 2 (Aseptic loosening), Type 3 (Structural failure), Type 4 (Infection), and Type 5 (Tumor progression).
Periprosthetic Joint Infection (PJI) and Aseptic Loosening
Infection (Henderson Type 4) is the most devastating complication, with incidence rates ranging from 5% to 15% in this highly vulnerable population. The combination of massive metallic foreign bodies, extensive soft tissue dissection, prolonged operative times, and chemotherapy-induced immunosuppression creates a perfect storm for bacterial colonization. Management of a deep PJI typically requires a two-stage revision: complete explantation of the expandable device, insertion of an antibiotic-impregnated cement spacer, prolonged intravenous antibiotics, and eventual reimplantation once the infection is eradicated.
Aseptic loosening (Henderson Type 2) is a long-term mechanical complication. The pediatric bone-implant interface is subjected to high functional demands and the unique stresses of the expansion process. Over time, stress shielding and micromotion can lead to osteolysis and loss of fixation. Revision surgery for aseptic loosening often requires transitioning to a larger diameter stem, utilizing longer modular segments, or employing complex biologic augmentation techniques like impaction bone grafting.

Mechanical Failure of the Expansion Mechanism
Structural failure (Henderson Type 3) is uniquely problematic in expandable prostheses. The internal lengthening mechanisms—whether the worm-drive of the minimally invasive models or the internal gearbox of the non-invasive electromagnetic models—are susceptible to jamming, mechanical stripping, or fatigue failure under the massive cyclic loads of pediatric ambulation.

When the expansion mechanism fails, the prosthesis can no longer lengthen, effectively converting it into a static implant and leading to progressive LLD. Salvage management requires surgical exploration to either replace the internal expansion module (if modularity allows) or to perform a complete revision of the entire diaphyseal segment of the prosthesis.
Tabular Summary of Complications and Salvage Strategies
| Complication (Henderson Type) | Estimated Incidence | Primary Salvage Management Strategy |
|---|---|---|
| Type 1: Soft Tissue Failure (e.g., extensor lag, wound breakdown) |
