Pelvic Resection: An Intraoperative Masterclass in Complex Oncologic Surgery
Key Takeaway
This masterclass provides an exhaustive, real-time surgical guide to pelvic resections. Fellows will learn critical anatomical landmarks, meticulous neurovascular dissection, precise osseous cuts, and strategies for managing complex tumors. We cover preoperative planning, intraoperative execution, and postoperative care, emphasizing technique, rationale, and complication avoidance for superior patient results.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking one of the most formidable challenges in the realm of orthopaedic oncology: a complex pelvic resection. The human pelvis, characterized by its intricate neurovascular networks, vital visceral topography, and uniquely demanding biomechanical load-sharing properties, requires an approach that transcends standard osteology. This intervention is not merely a bone resection; it is a high-stakes symphony of three-dimensional anatomical comprehension, uncompromising surgical precision, and dynamic intraoperative decision-making. Historically, primary malignant tumors of the pelvis were managed almost exclusively with hemipelvectomy (hindquarter amputation). However, advances in advanced cross-sectional imaging, neoadjuvant therapies, and reconstructive bioengineering have ushered in an era where limb-sparing pelvic resections are not only feasible but represent the standard of care for appropriately selected patients.



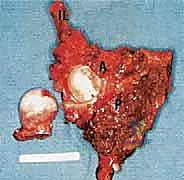
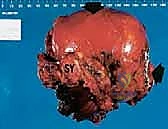
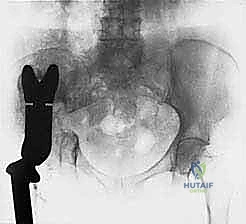
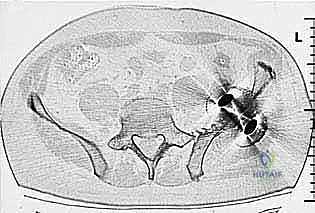
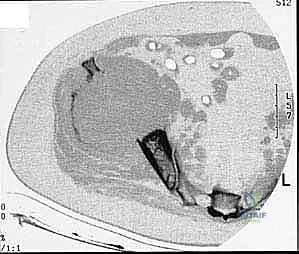
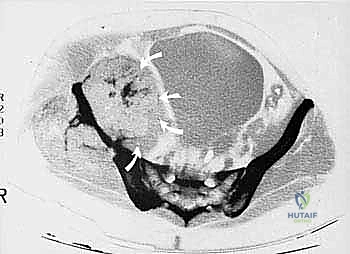
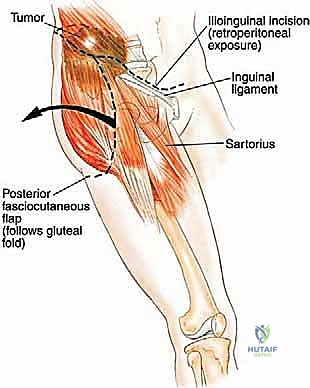
Primary malignant bone tumors of the pelvis account for approximately 10% to 15% of all primary bone sarcomas, with chondrosarcoma, osteosarcoma, and Ewing sarcoma constituting the vast majority. Chondrosarcoma, which our current patient presents with in the left periacetabular region, is particularly notorious in this anatomical location. These are primarily malignant osseous tumors characterized by a high propensity for massive myxomatous components and insidious extracompartmental extension. Because chondrosarcomas are largely recalcitrant to conventional chemotherapy and radiotherapy, the oncologic outcome rests almost entirely on the surgeon's ability to achieve an R0 (microscopically negative) resection margin. The anatomical constraints of the pelvis make achieving these wide margins exceptionally difficult, leading to local recurrence rates that historically eclipse those of appendicular sarcomas.
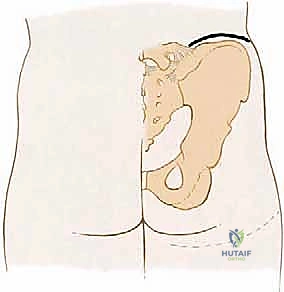
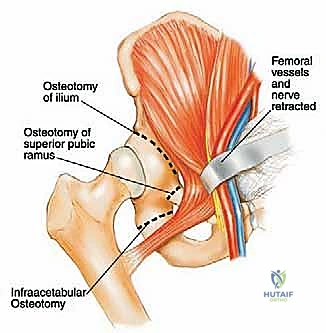
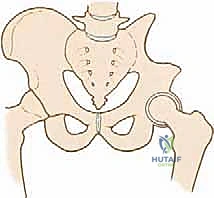
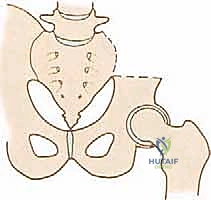
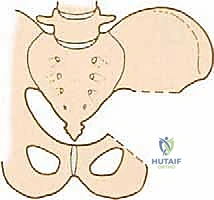
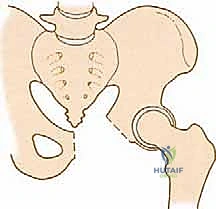
The epidemiology of pelvic sarcomas dictates a highly specialized, multidisciplinary approach. Patients often present late due to the capacious nature of the pelvic basin, which allows tumors to reach an enormous volume before compressing adjacent structures or causing palpable masses. Pain is typically the initial symptom, often misdiagnosed as radiculopathy, sacroiliitis, or degenerative joint disease of the hip. By the time a definitive diagnosis is established, the tumor frequently involves multiple zones of the pelvis. The Enneking and Dunham classification system remains our fundamental framework for describing these resections: Type I (iliac wing), Type II (periacetabular), Type III (pubis and ischium), and Type IV (sacral). Resections spanning multiple zones, particularly those involving the acetabulum (Type II), present the highest degree of reconstructive complexity and biomechanical compromise.
Understanding the patho-epidemiology also requires an appreciation of the metastatic cascade and local tissue infiltration. Pelvic tumors often breach the thin cortices of the ilium or the quadrilateral surface of the acetabulum early in their biological course, invading the iliacus or obturator internus muscles. The rich venous plexus of the pelvis provides a direct conduit for pulmonary metastasis, while the proximity to the lumbosacral plexus and major iliac vessels creates a perilous surgical environment. Consequently, mastering pelvic resection requires not just technical dexterity, but a profound respect for the aggressive biology of these neoplasms and the unforgiving nature of pelvic anatomy.

Detailed Surgical Anatomy and Biomechanics
Fellows, this is where our anatomical knowledge must be absolute. The pelvis is a labyrinth of vital structures, and navigating it requires a three-dimensional mental map that accounts for both normal anatomy and tumor-induced distortion. We must identify, isolate, protect, or—when oncologically mandated—intentionally sacrifice these structures with full prescience of the functional and physiological consequences. The biomechanical integrity of the pelvic ring, which transfers the entire axial load of the torso to the lower extremities, must be completely understood to plan an effective reconstruction or to accept a flail extremity.
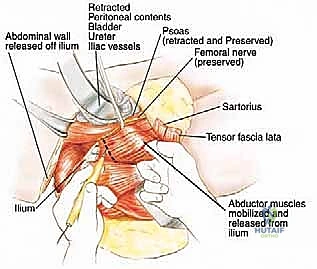
The architectural constraints of the pelvis leave zero margin for error. The proximity of the genitourinary and gastrointestinal tracts to the osseous boundaries means that visceral mobilization is a prerequisite for nearly all deep pelvic tumor extirpations. The peritoneum must be carefully swept medially, exposing the retroperitoneal space without violating the fascial planes that contain the malignancy. This delicate balance between achieving adequate exposure and maintaining oncologic compartmentalization is the hallmark of a master pelvic surgeon.
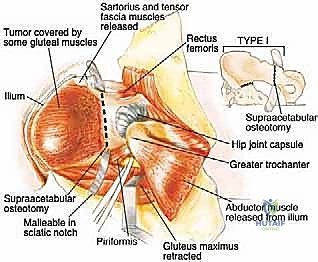
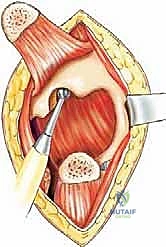
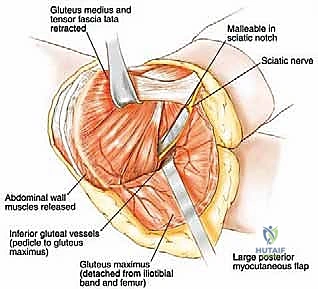
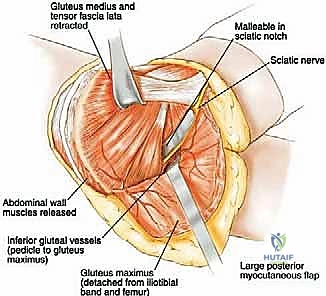
Furthermore, the muscular anatomy serves dual purposes: it acts as a barrier to tumor spread but also provides the necessary soft tissue envelope for reconstruction. The gluteus maximus, medius, and minimus are critical for postoperative ambulation. Preserving their neurovascular pedicles during massive resections is paramount. If the abductor mechanism must be sacrificed for oncologic margins, the biomechanical paradigm shifts entirely, necessitating complex tendon transfers or accepting a permanent Trendelenburg gait.
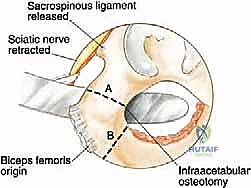
The interplay between the osseous anatomy and the ligaments—specifically the sacrospinous, sacrotuberous, and iliolumbar ligaments—dictates the intrinsic stability of the pelvic ring. Disruption of these ligaments during Type I or Type IV resections profoundly alters load distribution, often requiring lumbo-pelvic fixation to restore spinopelvic harmony. We will now dissect the specific anatomical subsystems that govern our surgical approach.

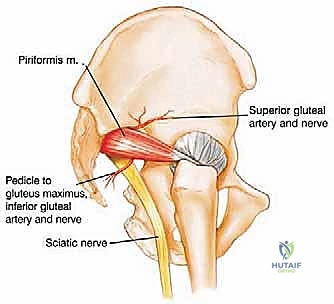
Pelvic Neurology and the Lumbosacral Plexus
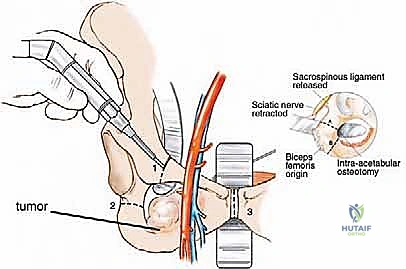
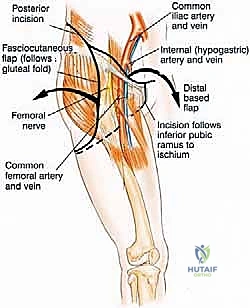
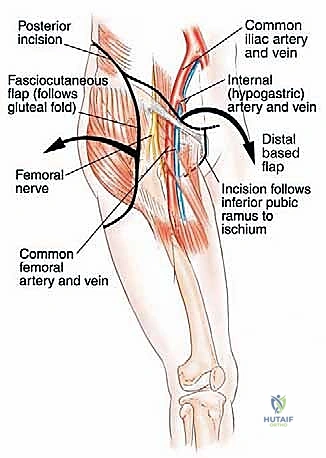
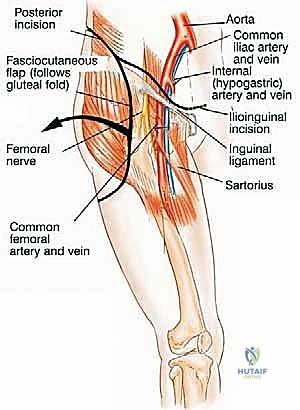
The neural anatomy of the pelvis is perhaps the most critical determinant of postoperative functional outcome and limb viability. The sciatic nerve (L4, L5, S1, S2, S3) is the largest nerve in the body and a paramount target for protection. It emerges from the pelvis through the greater sciatic notch, typically coursing inferior to the piriformis muscle, and enters the posterior compartment of the thigh lateral to the ischial tuberosity. We must remain hyper-vigilant of anatomical variants; in approximately 10% to 15% of patients, the common fibular division of the sciatic nerve pierces or exits superior to the piriformis, making its identification during posterior exposure highly precarious. It is accompanied by the inferior gluteal artery, which must be carefully managed to avoid devascularizing the gluteus maximus—a muscle essential for soft tissue coverage and closure.
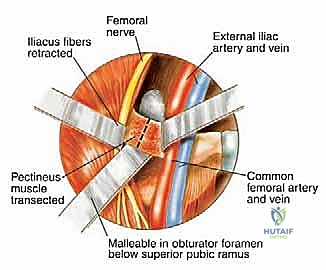
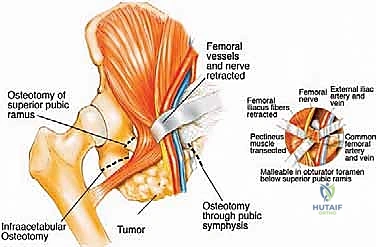
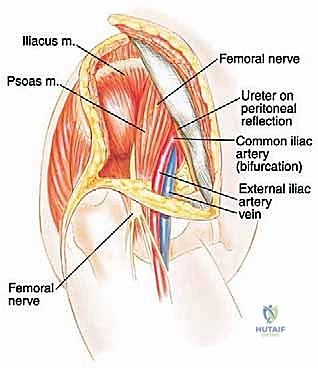
The femoral nerve (L2, L3, L4), arising from the posterior divisions of the ventral rami, passes inferolaterally between the psoas and iliacus muscles. It exits the pelvis under the inguinal ligament, lateral to the superficial femoral artery. During an internal hemipelvectomy, we identify the femoral nerve early in the iliopsoas interval. The nerve is highly susceptible to traction injury during prolonged retraction of the iliopsoas muscle belly. Meticulous dissection and the use of vessel loops for gentle, dynamic retraction are mandatory to preserve quadriceps function and anterior thigh sensation.
The obturator nerve (L2, L3, L4), formed from the anterior branches of the lumbar plexus, descends through the psoas, coursing distally over the sacral ala into the true pelvis, lateral to the ureter and deep to the internal iliac vessels. In Type III resections (obturator ring), this nerve is frequently encased by tumor and must be sacrificed. The resulting medial thigh numbness and loss of hip adduction is a functional deficit most patients tolerate remarkably well, as the pectineus and the adductor magnus (partially innervated by the femoral and sciatic nerves, respectively) provide compensatory adduction.
Finally, the pudendal nerve (S2, S3, S4) and the autonomic pelvic splanchnic nerves represent the frontier of visceral preservation. Coursing through Alcock's canal, the pudendal nerve governs perineal sensation and sphincter control. Bilateral sacrifice of the S2-S4 roots during extensive sacral resections results in profound bowel, bladder, and sexual dysfunction. Preoperative counseling regarding these specific neurologic deficits is an absolute ethical and clinical requirement before embarking on massive posterior pelvic resections.
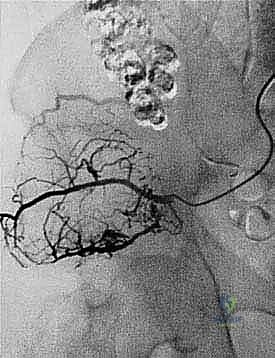
Pelvic Vasculature and Hemodynamic Control
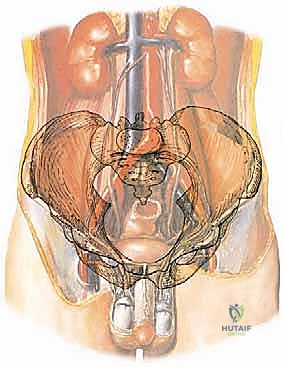
The vascular architecture of the pelvis is unforgiving. The abdominal aorta bifurcates at the L4 level into the common iliac arteries, which further divide into the internal and external iliac arteries at the level of the sacroiliac joint (S1). The external iliac artery courses along the pelvic brim to become the femoral artery, while the internal iliac artery dives into the true pelvis to supply the viscera, gluteal region, and perineum. A critical landmark during deep pelvic dissection is the ureter, which crosses the common iliac bifurcation anteriorly. Unintentional injury to the ureter during vascular mobilization is a catastrophic complication that necessitates immediate urologic intervention and risks chronic fistula formation.
Venous anatomy is even more treacherous than the arterial supply due to the thin-walled nature of the pelvic veins and the extensive collateral networks, such as the presacral venous plexus (Batson's plexus). The external and internal iliac veins lie posterior and medial to their corresponding arteries. Ligation of the internal iliac vein is often required for medial tumor mobilization, but extreme care must be taken to avoid tearing the confluence at the common iliac vein, which can result in massive, life-threatening hemorrhage. The presacral veins, lacking valves and tethered to the sacral periosteum, can bleed profusely if disrupted; control often requires bone wax, hemostatic matrix, or packing, rather than conventional electrocautery.
Furthermore, we must always anticipate the "corona mortis"—an anastomotic connection between the obturator and external iliac (or inferior epigastric) vascular systems located on the posterior aspect of the superior pubic ramus. Failure to identify and ligate this anastomosis prior to a pubic osteotomy will lead to rapid retraction of the bleeding vessel into the deep pelvis. The incidence of this variant is high enough that its presence should be assumed until proven otherwise during the exposure of the superior pubic ramus.
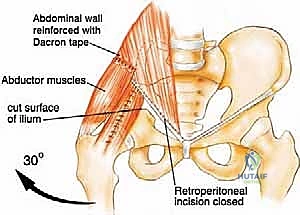
Collateral circulation must also be factored into our reconstructive planning. The deep circumflex iliac artery (DCIA) and the inferior epigastric artery are vital for the viability of regional soft tissue flaps, such as the rectus abdominis myocutaneous flap. If the external iliac system must be resected en bloc with the tumor, immediate vascular reconstruction with a synthetic graft (e.g., PTFE) or autologous vein graft is required to salvage the limb. The ischemic time must be strictly monitored, and temporary shunting may be necessary during prolonged reconstructive phases.



Biomechanical Load Transfer and Pelvic Ring Disruption
The native pelvis operates as a rigid, closed osteoligamentous ring. Axial loads from the spine are transmitted through the sacrum, across the sacroiliac joints, through the dense trabecular bone of the ilium (the sciatic buttress), and into the acetabulum, where the load is dispersed into the femoral head. This intricate load-sharing mechanism minimizes energy expenditure during bipedal locomotion. Understanding the precise vectors of these forces is essential for any reconstructive endeavor.
A Type I (iliac) resection disrupts the superior load-bearing arch, but if the acetabulum and a strut of bone connecting it to the sacrum remain intact, weight-bearing can often be preserved without massive reconstruction. The remaining bone can hypertrophy over time according to Wolff's Law. However, if the resection extends to the sacroiliac joint, lumbo-pelvic dissociation occurs, requiring robust spinopelvic fixation using pedicle screws and massive structural rod constructs to prevent proximal migration of the hemipelvis.
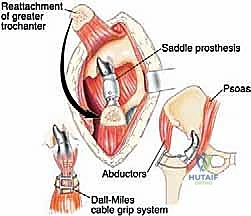
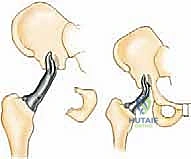
Conversely, a Type II (periacetabular) resection completely obliterates the load-transfer mechanism between the axial skeleton and the lower extremity. Reconstruction of this defect is arguably the most complex biomechanical challenge in orthopaedics. Options include massive structural allografts, custom 3D-printed triflange implants, saddle prostheses, or accepting a flail hip (pseudoarthrosis). Each reconstructive modality battles against colossal shear forces at the bone-implant or bone-graft interface.
Understanding these vector forces is critical; failure to achieve rigid initial fixation or subsequent biological integration inevitably leads to hardware fatigue, screw pullout, and catastrophic mechanical failure. The "flail hip" or resection arthroplasty, while historically viewed as a salvage option, remains a highly viable choice for patients with poor soft tissue envelopes or high infection risks. While it results in a significant limb length discrepancy and requires lifelong use of assistive devices, it eliminates the risk of hardware failure and provides a durable, albeit mechanically compromised, oncologic solution.
Exhaustive Indications and Contraindications
The decision to proceed with a limb-sparing pelvic resection versus a hemipelvectomy, or to opt for palliative management, requires rigorous patient selection. The primary goal is always oncologic clearance; functional preservation is strictly secondary. A meticulously planned resection that leaves microscopic disease (R1) or macroscopic disease (R2) behind does a profound disservice to the patient, virtually guaranteeing local recurrence and drastically reducing overall survival. The margin of resection is the single most important prognostic factor under the surgeon's direct control.
The indications for internal hemipelvectomy encompass primary malignant bone tumors confined to the pelvis where a wide excision is anatomically feasible. It is also indicated for selected cases of solitary, radioresistant metastatic lesions (such as renal cell or thyroid carcinoma) where complete extirpation offers a substantial survival or palliative benefit. Furthermore, locally aggressive benign lesions, such as massive giant cell tumors or aneurysmal bone cysts that have destroyed the joint and are not amenable to curettage, may necessitate segmental resection.
Contraindications are primarily dictated by the inability to achieve negative margins without sacrificing the very structures that make the limb functional or viable. If the tumor completely encases the external iliac artery and vein, and simultaneously infiltrates the lumbosacral plexus (particularly the L4-S1 nerve roots), preserving the limb will result in a flail, anesthetic, and potentially ischemic appendage that is functionally inferior to a well-fitted hemipelvectomy prosthesis.
Relative contraindications include extensive contamination of the fascial planes from a poorly planned prior biopsy, which may force the surgeon to expand the resection field beyond reconstructable limits. Additionally, severe cardiopulmonary comorbidities or profound malnutrition may preclude the patient from surviving the massive physiologic insult of a 12-hour pelvic resection. In such cases, less morbid palliative options, including cryoablation, embolization, or radiation, must be considered.
| Parameter | Indications for Limb-Sparing Pelvic Resection | Contraindications (Absolute & Relative) |
|---|---|---|
| Tumor Pathology | Primary bone sarcomas (Chondrosarcoma, Osteosarcoma, Ewing), isolated solitary metastasis (e.g., Renal Cell Carcinoma), locally aggressive benign tumors (Giant Cell Tumor). | Highly metastatic disease with poor life expectancy, systemic dissemination precluding local control. |
| Neurovascular Status | Major neurovascular bundles (sciatic nerve, external iliac vessels) are free of tumor or can be safely bypassed/grafted. | Absolute: Encasement of the external iliac vessels and the sciatic nerve precluding functional limb salvage. |
| Soft Tissue Envelope | Adequate tumor-free muscle and myocutaneous flaps available for robust soft tissue coverage of the reconstruction. | Relative: Massive fungating tumors, extensive prior radiation causing severe tissue fibrosis and compromised healing potential. |
| Visceral Involvement | Tumor is well-encapsulated or pushing against viscera without direct invasion of bladder, rectum, or major ureters. | Absolute: Extensive invasion into the pelvic viscera requiring unacceptably morbid exenteration for a marginal oncologic benefit. |
| Patient Physiology | Good baseline physiologic reserve, capable of withstanding massive fluid shifts, prolonged anesthesia, and rigorous rehabilitation. | Relative: Severe cardiopulmonary comorbidities, profound malnutrition, or inability to participate in postoperative rehabilitation. |

Pre-Operative Planning, Templating, and Patient Positioning
Before a single scalpel stroke is made, the entire surgical battle plan must be exhaustively detailed. Pelvic tumor surgery carries the highest rates of complications, surgical site infections, and mechanical failures among all anatomic sites, underscoring the absolute necessity of fastidious preoperative evaluation. The margin for error is non-existent; a millimeter of miscalculation can result in a positive oncologic margin or a catastrophic vascular injury. The planning phase is where the operation is truly won or lost.
The modern standard of care mandates that all cases be reviewed by a multidisciplinary tumor board (MDT). This board must include orthopaedic oncologists, musculoskeletal radiologists, pathologists, medical oncologists, radiation oncologists, and often vascular or urologic surgeons. This collective expertise ensures that the timing of surgery—particularly in relation to neoadjuvant chemotherapy or radiation—is perfectly optimized, and that all potential intraoperative contingencies are anticipated.
Advanced Imaging and 3D Templating
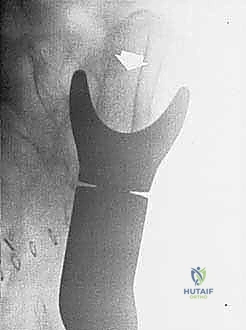
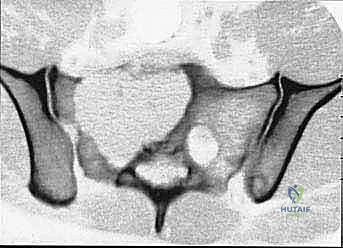
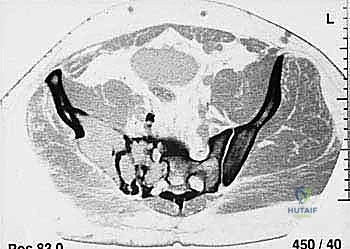
Our patient assessment begins with a multimodal imaging protocol. While plain radiography provides an initial overview of lytic or blastic destruction, it grossly underestimates the true intramedullary and soft-tissue extent of the tumor. High-resolution CT with intravenous contrast and 3D reconstruction is our primary workhorse. It delineates cortical destruction, maps the osseous anatomy for virtual osteotomy planning, and defines the critical relationship between the tumor mass and the major pelvic blood vessels.
MRI with and without gadolinium contrast is the gold standard for evaluating soft tissue extension, marrow replacement, and the involvement of adjacent muscle compartments and neurovascular bundles. We scrutinize the T1-weighted images to assess marrow margins and the T2-weighted fluid-sensitive sequences (such as STIR) to identify peritumoral edema, which must be respected during the resection to avoid leaving satellite tumor cells behind. FDG-PET/CT is indispensable for systemic staging, detecting distant metastases, and assessing the biological activity of the
Clinical & Radiographic Imaging Archive