Pediatric Femoral Shaft Fractures: A Masterclass in External Fixation

Key Takeaway
This masterclass provides a comprehensive, immersive guide to pediatric femoral external fixation. Fellows will learn intricate surgical anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution for EBI and AO/Synthes techniques. We cover pin placement, reduction maneuvers, and crucial pearls and pitfalls, ensuring a deep understanding of this critical procedure for femoral shaft fractures in children.
Comprehensive Introduction and Patho-Epidemiology
Pediatric femoral shaft fractures represent a significant proportion of major skeletal trauma in children and adolescents, demanding a nuanced understanding of evolving skeletal biology, biomechanics, and modern surgical techniques. Historically, the management of these injuries was overwhelmingly conservative, relying heavily on prolonged traction and spica casting. However, the paradigm has dramatically shifted over the last three decades. The psychosocial burden on the family, the economic impact of prolonged hospitalization or parental work absence, and the recognition of cast-related complications have driven a widespread consensus favoring operative stabilization for patients older than six years. As orthopedic surgeons, we must master a variety of fixation modalities, and external fixation remains an indispensable, highly versatile tool in our armamentarium.
The epidemiology of pediatric femoral shaft fractures demonstrates a classic bimodal age distribution, with distinct etiological factors driving each peak. The first peak occurs in early childhood, typically around two to three years of age. At this developmental stage, the skeletal architecture is characterized by a higher proportion of relatively weak woven bone. Coupled with the child’s newly acquired, often unsteady ambulation and a high propensity for low-energy falls, the femur is particularly susceptible to spiral or oblique fracture patterns. It is also imperative in this age group to maintain a high index of suspicion for non-accidental trauma, especially in non-ambulatory infants or when the mechanism of injury does not correlate with the fracture pattern.
Conversely, the second peak emerges in early adolescence, around age twelve, and extends into the teenage years. Fractures in this demographic are almost exclusively the result of high-energy trauma. Motor vehicle collisions, pedestrian-struck incidents, all-terrain vehicle (ATV) accidents, and high-velocity sporting injuries are the primary culprits. These high-energy mechanisms frequently result in complex, comminuted fracture patterns, significant soft tissue stripping, and a higher incidence of concomitant injuries, including traumatic brain injuries, thoracic trauma, and solid organ damage.

In the context of modern pediatric traumatology, external fixation serves a dual purpose. It is both a definitive management strategy for specific fracture patterns and a critical component of Damage Control Orthopedics (DCO). In the polytraumatized child presenting with the "lethal triad" of coagulopathy, hypothermia, and acidosis, prolonged surgical interventions like intramedullary nailing or complex plating are contraindicated. External fixation allows for rapid, minimally invasive stabilization of the major long bone, mitigating the systemic inflammatory response syndrome (SIRS), decreasing the risk of fat embolism or acute respiratory distress syndrome (ARDS), and facilitating nursing care and pulmonary toilet while the patient is resuscitated in the intensive care unit.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and the biomechanical forces acting upon the pediatric femur is the foundation of successful external fixation. The femur is the largest and strongest bone in the human body, surrounded by a massive muscular envelope that exerts immense deforming forces the moment skeletal continuity is disrupted. Understanding these vectors is paramount to achieving and maintaining an anatomical reduction.
Deforming Muscular Forces
The location of the fracture along the femoral diaphysis dictates the specific muscular deforming forces at play. In proximal third and subtrochanteric fractures, the proximal fragment is notoriously difficult to control. It is powerfully abducted by the gluteus medius and minimus, externally rotated by the short external rotators (piriformis, superior and inferior gemelli, obturator internus and externus, and quadratus femoris), and flexed by the iliopsoas. Consequently, the proximal fragment assumes a flexed, abducted, and externally rotated posture. The distal fragment is simultaneously pulled proximally by the rectus femoris, hamstrings, and adductors, resulting in profound shortening and varus angulation.
Midshaft fractures are primarily subjected to the overriding forces of the massive thigh musculature, leading to significant shortening. The adductor magnus, longus, and brevis exert a strong medial pull on the distal fragment, typically resulting in a varus deformity. The powerful quadriceps mechanism anteriorly and the hamstring complex posteriorly exacerbate the loss of length, making longitudinal traction a critical first step in the reduction maneuver.
Distal third and supracondylar femoral fractures present a unique and highly challenging biomechanical scenario. The distal fragment is subjected to a powerful apex-posterior deforming force driven by the gastrocnemius muscle, which originates from the posterior aspect of the medial and lateral femoral condyles. If not properly anticipated and neutralized, this apex-posterior angulation can lead to vascular compromise of the popliteal artery, delayed union, or a malunion that significantly alters knee joint kinematics.
Neurovascular Corridors and Safe Zones
When applying an external fixator, the surgeon must navigate the soft tissue envelope with absolute precision to avoid catastrophic iatrogenic injury to major neurovascular structures. The femur is divided into functional corridors, and selecting the correct trajectory for pin insertion is non-negotiable. The medial aspect of the thigh is an absolute "no-go" zone for external fixation pins. Proximally, the femoral artery, vein, and nerve course through the femoral triangle and subsequently enter the adductor (Hunter's) canal, protected only superficially by the sartorius muscle. Deeper within the medial compartment, the profunda femoris artery and its perforating branches provide critical vascularity to the musculature; injury here can result in massive, life-threatening hemorrhage or compartment syndrome.
The posterior thigh houses the sciatic nerve, which descends deep to the long head of the biceps femoris. While direct transfixion of the sciatic nerve by a laterally placed pin is rare, excessive posterior angulation of pins, particularly in the proximal or mid-diaphysis, can cause nerve impingement or neuropraxia. Furthermore, overly aggressive blunt dissection or the use of dull drill bits can cause soft tissue wrapping, indirectly tethering and injuring the nerve.
The lateral aspect of the femur provides the safest and most reliable corridor for pin placement. The vastus lateralis provides a robust muscular cushion. Pins should be placed strictly laterally or slightly anterolaterally. However, surgeons must remain vigilant regarding the lateral femoral cutaneous nerve in the extremely proximal thigh. In the distal femur, as one approaches the metaphyseal flare, the popliteal artery and vein lie directly posterior to the bone. Pins placed in the distal fragment must be strictly lateral and must not over-penetrate the medial cortex excessively, lest they endanger the popliteal bundle or the common peroneal nerve as it courses laterally toward the fibular head.
Osteology and Physeal Considerations
The pediatric skeletal system is defined by the presence of open physes (growth plates), which are highly metabolically active and uniquely susceptible to iatrogenic trauma. The distal femoral physis is particularly critical, as it is the fastest-growing physis in the human body, contributing approximately 70% of the longitudinal growth of the femur and 40% of the overall growth of the lower extremity. Any surgical intervention must meticulously respect this anatomical boundary.
The cardinal rule of pediatric external fixation is the "2 cm rule." The surgeon must ensure a minimum of 2 centimeters of intact bone between the outermost external fixation pin and the adjacent physis. Furthermore, there must be at least 2 centimeters of intact bone between the innermost pin and the fracture site to prevent propagation of the fracture or interference with the fracture hematoma and subsequent callus formation.
Violation of the physis with a drill bit or a Schanz screw can lead to catastrophic consequences, including partial or complete physeal arrest. A central physeal arrest will result in a progressive limb length discrepancy (LLD), whereas a peripheral arrest will cause a tethering effect, leading to progressive angular deformity (e.g., valgus or varus knee) as the child grows. Pre-operative templating and strict intra-operative fluoroscopic visualization are mandatory to verify pin-to-physis distances.
Exhaustive Indications and Contraindications
The decision to utilize external fixation for a pediatric femoral shaft fracture requires a sophisticated synthesis of patient-specific variables, including age, weight, physiological status, fracture morphology, and the presence of concomitant injuries. While flexible intramedullary nailing (e.g., Titanium Elastic Nails - TENs) has become the gold standard for many length-stable midshaft fractures in school-aged children, external fixation retains highly specific, irreplaceable indications.
Indications for Operative Management
The most absolute indication for external fixation in pediatric femoral trauma is the polytraumatized patient. In the setting of Damage Control Orthopedics (DCO), a child presenting with severe head trauma, blunt thoracic injury, or hemodynamic instability cannot tolerate the physiological hit of a prolonged open reduction or intramedullary reaming. External fixation allows for rapid, life-saving stabilization of the femur in under 30 minutes, controlling hemorrhage from the fracture site, reducing pain, and facilitating immediate transfer to the pediatric intensive care unit.
Open fractures of the femoral shaft, particularly Gustilo-Anderson Type II, IIIA, and IIIB injuries, strongly favor external fixation. These injuries are characterized by significant soft tissue stripping, periosteal devascularization, and gross contamination. Placing intramedullary hardware in this setting carries an unacceptably high risk of deep intramedullary infection. External fixation provides rigid skeletal stability while allowing unimpeded access to the soft tissue wounds for serial debridement, vacuum-assisted closure (VAC) application, and eventual soft tissue reconstruction by plastic surgery.
Certain complex fracture morphologies also dictate the use of external fixation. Highly comminuted, length-unstable fractures where flexible nails would fail to maintain length and rotation are excellent candidates. Furthermore, very proximal subtrochanteric fractures or very distal diaphyseal-metaphyseal junctional fractures often lack sufficient medullary canal length for the stable seating of flexible nails. In these extreme proximal or distal zones, a carefully constructed external fixator provides superior biomechanical control.
Contraindications and Alternative Modalities
While highly versatile, external fixation is not without contraindications. Absolute contraindications are rare but include severe metabolic bone diseases such as severe Osteogenesis Imperfecta, where the osteopenic bone cannot provide adequate cortical purchase for the Schanz screws, leading to immediate catastrophic pull-out.
Relative contraindications revolve heavily around the psychosocial environment of the patient. External fixation requires meticulous, daily pin site care to prevent infection. If the surgeon assesses that the patient's family is non-compliant, lacks the cognitive ability to perform pin care, or resides in an environment with extremely poor hygiene, alternative fixation methods should be strongly considered. Additionally, in older, heavier adolescents approaching skeletal maturity (typically >50 kg or >12 years old with closed or closing physes), rigid, trochanteric-entry locked intramedullary nailing is often preferred over external fixation due to the high risk of frame failure or pin bending in heavy patients.
Alternative modalities must always be weighed. Spica casting remains appropriate for isolated fractures in children under 5-6 years of age. Submuscular bridge plating is an excellent alternative for length-unstable or comminuted fractures in children where flexible nailing is insufficient, offering the benefit of avoiding external pins, though it requires a more extensive surgical exposure and a subsequent hardware removal surgery.
| Indication Category | Specific Scenarios Favoring External Fixation | Contraindications / Scenarios Favoring Alternatives |
|---|---|---|
| Patient Physiology | Polytrauma (DCO), Hemodynamic instability, Severe Traumatic Brain Injury. | Stable, isolated injuries in older adolescents (Favor Rigid IM Nail). |
| Soft Tissue Status | Gustilo-Anderson Type II, III open fractures, massive degloving, burns. | Clean, closed fractures with good soft tissue envelope (Favor TENs or Plating). |
| Fracture Morphology | Severe comminution (length unstable), extreme proximal/distal junctional zones. | Transverse/short oblique midshaft fractures (Favor TENs). |
| Psychosocial Factors | Compliant family, ability to perform daily pin care. | Non-compliant family, poor hygiene, inability to follow up. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of an external fixation procedure is largely determined before the patient ever enters the operating theater. Meticulous pre-operative planning, precise templating, and optimal patient positioning are critical steps that mitigate intra-operative complications and ensure a smooth, efficient surgical workflow.
Imaging Modalities and Templating
Standard radiographic evaluation must include high-quality, orthogonal anteroposterior (AP) and lateral radiographs of the entire femur. Crucially, the imaging must capture the joint above (the hip and pelvis) and the joint below (the knee). This is mandatory to rule out ipsilateral femoral neck fractures, pelvic ring disruptions, or associated knee ligamentous injuries, which are frequently missed in high-energy trauma. If the patient is stable, a scanogram or full-length standing radiograph of the uninjured contralateral limb is highly beneficial to establish the patient's baseline anatomical length, which will serve as the reduction target.
Templating is an essential exercise. Using digital or physical overlays, the surgeon must pre-determine the optimal pin sites, frame configuration, and hardware dimensions. For pediatric femurs, pin diameter is a critical variable. The core diameter of the Schanz screw should not exceed one-third of the diaphyseal diameter of the bone at the insertion site; exceeding this threshold drastically increases the risk of iatrogenic fracture through the pin hole. Typically, 4.0-mm to 5.0-mm Schanz screws are utilized, depending on the child's age and bone caliber.
During templating, the surgeon explicitly maps out the "safe zones." The physes are identified, and the 2-centimeter boundary is marked. The fracture extent is delineated, ensuring another 2-centimeter clearance. The frame configuration—whether a simple monolateral/uniplanar frame for a simple fracture, or a modular/biplanar frame for a highly unstable comminuted fracture—is selected based on the anticipated biomechanical demands.
Operating Room Setup and Patient Positioning
The choice of operating table is a strategic decision. While a fracture table allows for sustained mechanical traction and facilitates closed reduction, it severely limits access to the patient if a conversion to an open approach is required, and it can complicate the management of polytraumatized patients with spine or pelvic injuries. Therefore, placing the patient supine on a fully radiolucent flat table is generally preferred. This setup offers maximum versatility, unimpeded access to the airway for anesthesia, and allows for simultaneous surgical interventions by other trauma teams.
Proper positioning requires meticulous attention to detail. A small radiolucent bump is placed under the ipsilateral hemipelvis. This serves to internally rotate the lower extremity to a neutral position, counteracting the natural tendency of the injured leg to fall into external rotation. All bony prominences, including the sacrum, contralateral heel, and elbows, must be heavily padded to prevent decubitus ulcers during what can sometimes be a lengthy polytrauma resuscitation.
The entire injured lower extremity is prepped and draped freely from the level of the iliac crest down to the toes. Draping the leg freely allows the surgeon to assess rotational alignment clinically by comparing the patella-to-foot axis with the contralateral side. The C-arm fluoroscopy unit is typically brought in from the contralateral side of the table, positioned perpendicular to the patient. The surgeon must confirm that the C-arm can easily track from the hip joint down to the knee joint in both AP and lateral planes without obstruction before the surgical incision is made.
Step-by-Step Surgical Approach and Fixation Technique
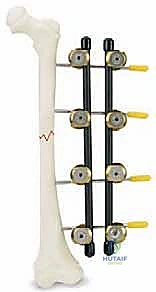
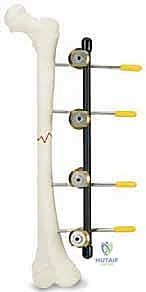
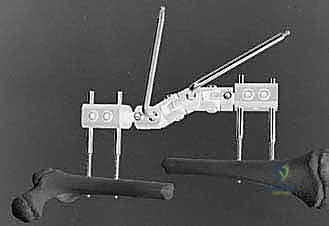
The intra-operative execution of external fixation requires a blend of anatomical precision, respect for soft tissues, and mechanical engineering principles. For this masterclass, we will detail the application using a standard modular or monolateral system, such as the EBI DFS XS Fixator, though the fundamental principles apply universally across modern fixator designs.
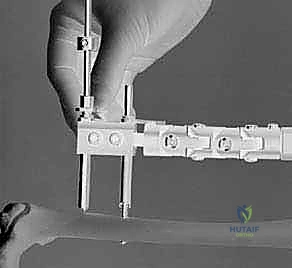
Initial Incision and Soft Tissue Dissection
The procedure begins by identifying the most challenging fragment to control, which is typically the distal fragment due to its tendency for apex-posterior angulation and the proximity of the distal femoral physis. Using fluoroscopic guidance, the pre-templated pin sites are marked on the skin laterally.
A sharp, longitudinal stab incision, approximately 1 to 1.5 centimeters in length, is made through the skin and subcutaneous tissue. It is critical to make the incision slightly larger than the pin diameter to prevent skin tenting and subsequent pressure necrosis, which is a primary catalyst for pin tract infections. Following the skin incision, blunt dissection is absolutely mandatory. Using a small hemostat or a blunt periosteal elevator, the surgeon dissects down to the lateral cortex (the linea aspera).
The instrument is used to gently spread the fibers of the vastus lateralis longitudinally, rather than cutting them. This blunt spreading technique pushes muscular branches of the profunda femoris artery out of the trajectory and prevents the muscle tissue from wrapping around the drill bit. Once the instrument touches bone, it is swept anteriorly and posteriorly to palpate the curvature of the lateral cortex, ensuring the pin will be placed centrally on the diaphyseal axis.
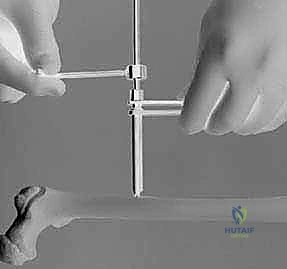
Pin Insertion Protocol
With the bone exposed, the soft tissue guide (consisting of an outer sleeve and an inner trocar) is inserted through the dissected corridor and seated firmly against the lateral cortex. The surgeon must verify both visually and fluoroscopically that the trocar is perfectly perpendicular to the anatomical axis of the femur in both the AP and lateral planes. Off-axis drilling can lead to eccentric pin placement, glancing off the cortex, or inadequate biomechanical hold.
Once positioning is confirmed, the trocar is removed, and the appropriate drill guide
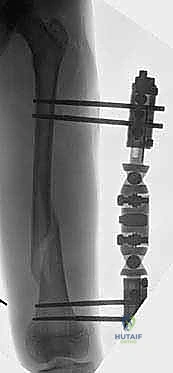
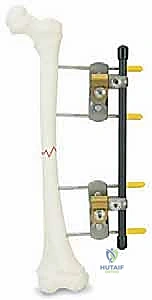
Clinical & Radiographic Imaging Archive