Pectoralis Major Transfer: Reconstructing Irreparable Subscapularis Tears
Key Takeaway
Welcome to the OR, fellows. Today, we're tackling the complex pectoralis major transfer for irreparable subscapularis tears. This masterclass will guide you through meticulous preoperative planning, exact patient positioning, and granular step-by-step intraoperative execution. We'll cover critical anatomical landmarks, neurovascular protection, instrument precision, and advanced fixation techniques, ensuring a comprehensive understanding of this challenging reconstructive procedure.
Comprehensive Introduction and Patho-Epidemiology
The management of irreparable subscapularis tears represents one of the most formidable challenges in modern reconstructive shoulder surgery. The subscapularis muscle, the largest and most powerful of the four rotator cuff muscles, serves as the primary internal rotator of the glenohumeral joint and acts as a critical anterior stabilizer of the humeral head. When this vital structure is compromised, the delicate transverse force couple of the shoulder is disrupted, leading to profound kinematic alterations, devastating functional loss, and accelerated glenohumeral degeneration. A pectoralis major transfer is not merely a salvage procedure; it is a meticulously planned biomechanical reconstruction designed to restore this anterior force couple, re-center the humeral head, and salvage the patient's quality of life.
Subscapularis tears most frequently occur following acute traumatic events, such as falls onto an outstretched arm, forceful hyperextension injuries, or abrupt external rotation forces applied to an abducted arm. Furthermore, anterior shoulder dislocations are a well-documented catalyst for subscapularis avulsions, particularly in older patient populations where the tendon may already be compromised by age-related microvascular attenuation. While isolated tears of the upper tendinous insertion are common, massive trauma can precipitate a complete avulsion involving both the tendinous upper two-thirds and the muscular lower one-third of the footprint. In rare instances, chronic repetitive microtrauma and insidious tissue degeneration can lead to attrition and eventual failure of the subscapularis tendon without a discrete traumatic event.
A pathognomonic feature of subscapularis tears—and a primary reason they are frequently missed during initial clinical evaluations—is the preservation of the anterior fascial sleeve. Unlike supraspinatus or infraspinatus tears, which typically retract and expose the bare articular cartilage and the greater tuberosity footprint, a torn subscapularis tendon often retracts medially while leaving a contiguous layer of fascial tissue spanning the anterior shoulder. This "hidden lesion" obscures the underlying pathology, as the fascial sleeve remains attached to the lesser tuberosity, mimicking an intact tendon on superficial inspection or suboptimal imaging. Consequently, patients often present with chronic, retracted tears that have surpassed the critical biological window for primary repair.
When a subscapularis tear remains untreated for approximately six months or longer, the muscle undergoes irreversible architectural changes characterized by severe volumetric atrophy and fatty infiltration, typically progressing to Goutallier Grade III or IV. At this juncture, the native tendon becomes inelastic and heavily retracted medial to the glenoid rim. Any attempt at primary mobilization and repair under such circumstances would result in exorbitant tension across the repair site, invariably leading to catastrophic early failure. Recognizing this state of irreparability is the crucial inflection point where the orthopedic surgeon must pivot toward regional muscle transfer options, with the pectoralis major serving as the historically proven and biomechanically sound workhorse for anterior reconstruction.
The Natural History of the Deficient Subscapularis
Understanding the natural history of an untreated, irreparable subscapularis tear is essential for counseling patients and justifying surgical intervention. The loss of the anterior force couple allows the posterior cuff (infraspinatus and teres minor) to exert an unopposed posterior and superior pull on the humeral head. This dynamic imbalance initially manifests as increased, uncontrolled external rotation and profound weakness in internal rotation, severely limiting activities of daily living such as reaching the abdomen or lower back.
As the pathology progresses, the dynamic instability transitions into static superior and anterior migration of the humeral head. The coracoacromial arch becomes the secondary restraint to superior translation, leading to progressive wear of the acromial undersurface and the coracoid process. This altered kinematic environment rapidly accelerates articular cartilage degradation, culminating in a specific pattern of rotator cuff tear arthropathy characterized by eccentric anterior and superior glenoid wear.
Nonoperative management, consisting of physical therapy focused on periscapular stabilization and compensatory strengthening of the deltoid and remaining intact cuff, rarely alters this biomechanical trajectory in the setting of a massive, retracted tear. Corticosteroid injections and nonsteroidal anti-inflammatory drugs (NSAIDs) may offer transient symptomatic relief but do not address the underlying mechanical deficit. Therefore, in the appropriately selected patient, surgical reconstruction via a pectoralis major transfer is the definitive intervention to halt this degenerative cascade and restore functional shoulder kinematics.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the regional anatomy is the absolute prerequisite for executing a pectoralis major transfer safely and effectively. The subscapularis originates from the deep, volar surface of the scapula—the subscapular fossa—and courses laterally to insert onto the lesser tuberosity of the humerus. The insertion footprint is broad and comma-shaped, with the superior two-thirds being distinctly tendinous and the inferior one-third being primarily muscular. This superior tendinous portion interdigitates with the coracohumeral ligament and the superior glenohumeral ligament to form the biceps reflection pulley, explaining the high incidence of concomitant long head of the biceps tendon (LHBT) subluxation or dislocation in the presence of subscapularis tears.
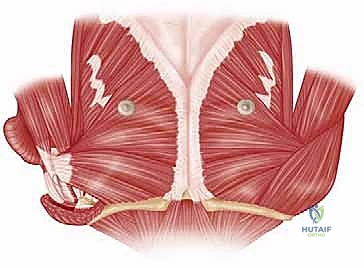
The pectoralis major, our selected donor muscle, is a massive, fan-shaped, bilaminar muscle that provides powerful adduction, internal rotation, and flexion of the humerus. It is anatomically divided into two primary heads: the clavicular head and the sternocostal (sternal) head. The clavicular head originates from the medial one-half to one-third of the clavicle, forming the anterior lamina of the muscle belly. The larger sternocostal head originates from the anterior surface of the manubrium, the superior six costal cartilages, and the aponeurosis of the external oblique muscle, forming the posterior lamina.

These two distinct muscular heads converge laterally to form a complex, U-shaped bilaminar tendon that inserts onto the lateral lip of the intertubercular (bicipital) groove of the humerus. A critical anatomical nuance for the reconstructive surgeon is the twisted nature of the sternal head's insertion: the most inferior muscular fibers of the sternal head course superiorly and posteriorly to insert on the most proximal aspect of the humeral footprint. Consequently, when the tendon is released from the humerus, the muscle tends to "flip" or untwist. To maintain proper spatial orientation and optimal length-tension relationships during the transfer, the superior corner of the released tendon must be meticulously tagged with heavy non-absorbable suture immediately upon detachment.
Critical Neurovascular Boundaries
The success of the pectoralis major transfer hinges entirely on the preservation of its neurovascular pedicles during mobilization. The muscle receives its innervation from the medial and lateral pectoral nerves, branches of the medial and lateral cords of the brachial plexus, respectively. The lateral pectoral nerve (C5-C7) primarily innervates the clavicular head and the superior aspect of the sternal head, entering the muscle belly at a mean distance of 12.5 cm (range, 10.0 to 14.9 cm) medial to its humeral insertion. The medial pectoral nerve (C8-T1) pierces the pectoralis minor to innervate the sternocostal head, entering the pectoralis major approximately 11.9 cm (range, 9.0 to 14.5 cm) from the humeral insertion and roughly 2.0 cm from the inferior muscular border.
Clinical Pearl: To prevent devastating iatrogenic denervation of the transferred muscle, medial dissection and mobilization of the pectoralis major must be strictly limited to a maximum of 6 to 8 cm medial to its humeral insertion. Violating this boundary risks traction injury or direct transection of the pectoral nerves, rendering the transfer functionally useless.
Furthermore, the musculocutaneous nerve must be carefully respected, particularly when performing a subcoracoid transfer. This nerve branches from the lateral cord and penetrates the conjoint tendon (coracobrachialis and short head of the biceps) at an average of 6.1 cm (range, 3.5 to 10 cm) distal to the coracoid process tip. During the creation of a subcoracoid tunnel for the transferred pectoralis tendon, aberrant or proximal branches of the musculocutaneous nerve are at high risk of iatrogenic injury if blunt dissection is not executed with extreme caution. Finally, the anterior humeral circumflex artery, which courses laterally at the demarcation between the tendinous and muscular portions of the pectoralis major insertion, must be identified and coagulated or ligated during the humeral release to prevent obscuring hemorrhage.
Exhaustive Indications and Contraindications
The decision to proceed with a pectoralis major transfer requires a rigorous clinical evaluation and a clear understanding of the patient's functional deficits, physiological age, and anatomical limitations. The primary indication is a chronic, irreparable tear of the subscapularis tendon in a patient experiencing intractable pain and significant functional disability, specifically profound weakness in internal rotation and loss of anterior active elevation. "Irreparability" is generally defined by the presence of static superior or anterior humeral head subluxation, severe tendon retraction medial to the glenoid rim (Patte Stage 3), and advanced fatty infiltration of the muscle belly (Goutallier Grade III or IV) on magnetic resonance imaging (MRI) or computed tomography (CT).
Patients typically present with a positive "lift-off" test (inability to lift the dorsum of the hand away from the lower back), a positive "belly-press" test (inability to maintain pressure on the abdomen without flexing the wrist or dropping the elbow posteriorly), and a positive "bear-hug" test. Furthermore, patients will demonstrate increased passive external rotation compared to the contralateral side, lacking a firm end-point due to the absence of the anterior capsulotendinous restraint. The transfer is highly indicated in younger, active patients who require restoration of strength for activities of daily living or manual labor, and who are not yet candidates for reverse total shoulder arthroplasty (RTSA).
Contraindications must be strictly observed to prevent catastrophic surgical failures. Absolute contraindications include a deficient or paralyzed deltoid muscle (specifically the axillary nerve), as the deltoid is the primary elevator of the shoulder and its function is paramount following any rotator cuff reconstruction. Advanced glenohumeral osteoarthritis or established rotator cuff tear arthropathy (Hamada Grade 3 or higher) is a strong contraindication, as a soft-tissue transfer will not address the arthritic pain and will likely fail in the setting of altered joint mechanics; these patients are better served with an RTSA.
Table 1: Indications and Contraindications for Pectoralis Major Transfer
| Category | Criteria | Clinical Rationale |
|---|---|---|
| Primary Indications | Irreparable Subscapularis Tear | Goutallier Grade III/IV, retraction medial to glenoid, >6 months chronicity. |
| Intractable Pain & Weakness | Positive belly-press, lift-off, and bear-hug tests; loss of internal rotation power. | |
| Failed Primary Repair | Revision scenario where native tissue is attenuated or structurally compromised. | |
| Concomitant Irreparable Supraspinatus | Can be combined with other transfers (e.g., Latissimus Dorsi) if posterior cuff is intact. | |
| Absolute Contraindications | Deltoid Deficiency / Axillary Nerve Palsy | Deltoid is essential for elevation; transfer will fail without deltoid function. |
| Advanced Glenohumeral Arthritis | Soft tissue transfer cannot salvage an arthritic joint; RTSA is indicated. | |
| Severe Coracoid Impingement | May require coracoplasty to prevent abrasion of the transferred tendon. | |
| Active Infection | Absolute contraindication for any elective reconstructive orthopedic procedure. | |
| Relative Contraindications | Advanced Physiological Age | Lower functional demands may be adequately managed non-operatively or with RTSA. |
| Uncontrolled Medical Comorbidities | High risk for perioperative complications or poor soft-tissue healing. | |
| Poor Patient Compliance | Inability to adhere to strict postoperative immobilization and phased rehabilitation. |
Furthermore, global brachial plexopathy or severe cervical radiculopathy compromising the pectoral nerves renders the donor muscle non-functional. Relative contraindications include older patients with low functional demands, where the extensive rehabilitation required for a tendon transfer may outweigh the potential benefits. In such cases, a biologically conservative approach or arthroplasty may be more appropriate.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful pectoralis major transfer. The clinical examination must be corroborated with high-quality imaging. A standard radiographic shoulder series—comprising an anteroposterior (AP) view, a true AP of the glenohumeral joint (Grashey view), a scapular Y view, and an axillary lateral view—is mandatory. These radiographs allow the surgeon to assess for proximal humeral migration (diminished acromiohumeral interval), anterior subluxation of the humeral head, and the presence of degenerative joint disease. The axillary view is particularly critical for evaluating static anterior subluxation, a hallmark of massive subscapularis deficiency.
Advanced soft-tissue imaging is non-negotiable. An MRI without contrast is typically sufficient to evaluate the degree of subscapularis tendon retraction, the cross-sectional area of the muscle belly, and the extent of fatty infiltration using the Goutallier classification system. The MRI will also delineate the status of the superior and posterior rotator cuff, which heavily influences the overall prognosis. Additionally, the surgeon must meticulously evaluate the long head of the biceps tendon, which is frequently subluxated, medially dislocated, or partially torn in these patients. If the patient has a pacemaker or other MRI contraindications, a CT arthrogram provides excellent visualization of tendon retraction and muscle quality.

Once the decision for surgery is finalized, meticulous attention to patient positioning is required. The procedure is performed with the patient under general anesthesia, typically supplemented with an interscalene regional nerve block for optimal postoperative pain control. The patient is placed in the modified beach chair position, with the head of the bed elevated to approximately 45 to 60 degrees.
Optimizing the Surgical Field
Proper positioning of the head and neck is paramount to avoid iatrogenic cervical spine or brachial plexus injuries. The head is secured in a commercially available foam headrest, ensuring the cervical spine remains in a neutral alignment without excessive lateral flexion, rotation, or extension. The non-operative arm is heavily padded and secured across the patient's abdomen or on an arm board. All bony prominences, including the sacrum, greater trochanters, and heels, must be meticulously padded to prevent pressure necrosis.
The operative arm is prepped and draped free to allow for unrestricted manipulation throughout the procedure. We highly recommend utilizing a sterile, commercially available pneumatic or hydraulic arm positioner (such as a Spider limb positioner). This device allows the surgeon to dynamically adjust the arm into varying degrees of abduction, forward flexion, and rotation, which is critical for exposing the subcoracoid space, mobilizing the pectoralis major, and precisely tensioning the transfer during final fixation. The surgical prep should extend from the base of the neck, across the sternum to the contralateral mid-clavicular line, and down to the costal margin to ensure the entire pectoralis major muscle is accessible within the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
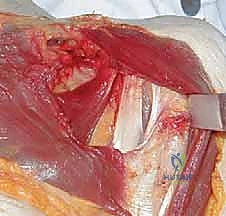
The surgical execution of a pectoralis major transfer demands meticulous soft tissue handling and precise anatomical navigation. We utilize an extensile deltopectoral approach, which provides unparalleled access to the anterior shoulder, the coracoid process, and the entire footprint of the pectoralis major.
Incision and Deep Exposure
A curvilinear incision measuring approximately 8 to 10 centimeters is made, beginning just lateral to the tip of the coracoid process and extending distally along the deltopectoral groove toward the deltoid tuberosity.
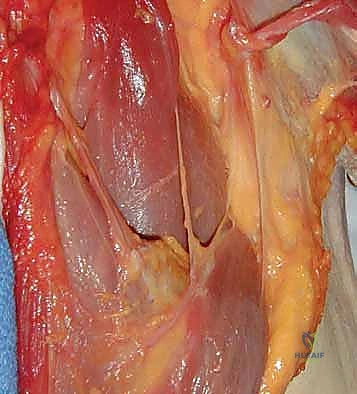
Subcutaneous flaps are elevated to expose the deltopectoral fascia. The cephalic vein is identified as the primary landmark for the interval. While the vein can be retracted either medially or laterally, we prefer to retract it laterally with the deltoid muscle to preserve its primary venous tributaries and minimize the risk of postoperative cephalic vein thrombosis. The deltopectoral interval is bluntly developed, and a self-retaining retractor is placed to maintain exposure.
The clavipectoral fascia is incised lateral to the conjoint tendon, exposing the subscapularis space. At this juncture, the long head of the biceps tendon is systematically evaluated. Given the high incidence of pathology associated with subscapularis tears, an open subpectoral biceps tenodesis or a simple tenotomy is routinely performed to eliminate a significant source of anterior shoulder pain. The native subscapularis is then explored. Even in cases deemed "irreparable" on MRI, an aggressive attempt is made to mobilize the tendon by releasing the anterior, superior, and posterior capsular adhesions. If a partial repair of the inferior footprint is achievable, it should be performed, as it augments the overall biomechanical construct and provides a biological scaffold for the transfer.
Pectoralis Major Harvest and Mobilization
The insertion of the pectoralis major on the lateral lip of the bicipital groove is sharply defined. Depending on the patient's specific anatomical requirements and the surgeon's preference, either the clavicular head alone, the sternal head alone, or the entire whole muscle can be transferred. For this masterclass, we will describe the transfer of the clavicular head, which provides an excellent vector for internal rotation and superior stability.
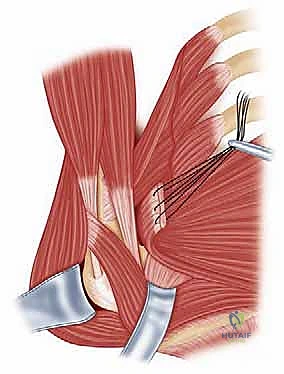
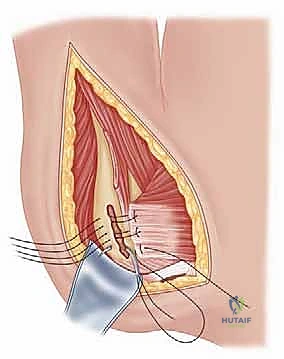
The interval between the clavicular and sternal heads is bluntly developed. The clavicular head is sharply detached from its humeral insertion, taking care to coagulate the anterior humeral circumflex artery branches. Immediately upon detachment, the superior and inferior corners of the tendon are tagged with heavy, non-absorbable traction sutures (e.g., #2 FiberWire) to prevent the muscle from "flipping" and losing its spatial orientation.

The muscle belly is then carefully mobilized medially. Crucial Step: As previously emphasized, this medial dissection must strictly halt at 6 to 8 centimeters from the insertion site to absolutely guarantee the preservation of the lateral pectoral nerve. Blunt finger dissection is used to free the deep surface of the muscle from the underlying clavipectoral fascia and the pectoralis minor.
Routing and Final Fixation
The routing of the transferred tendon can be performed either superficial or deep to the conjoint tendon (subcoracoid). The subcoracoid routing, championed by Resch, is biomechanically superior as it more closely replicates the native vector of the subscapularis and prevents anterior subluxation of the transfer. However, it carries a higher risk of injury to the musculocutaneous nerve.
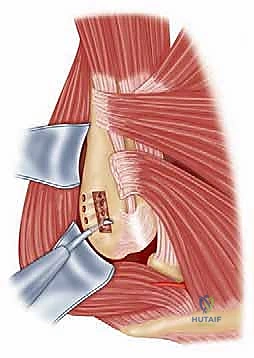
To create the subcoracoid tunnel, blunt dissection is performed deep to the conjoint tendon, staying strictly on the anterior surface of the subscapularis muscle belly to avoid plunging into the brachial plexus. A passing suture or a large curved clamp is passed through the tunnel from lateral to medial. The traction sutures of the pectoralis tendon are retrieved and the tendon is gently shuttled deep to the conjoint tendon toward the lesser tuberosity.
The lesser tuberosity footprint is decorticated with a high-speed burr or a rasp to create a bleeding bony bed, optimizing tendon-to-bone healing. Fixation is typically achieved using a double-row or a transosseous-equivalent suture anchor construct. Two to three double-loaded suture anchors are placed in the medial aspect of the lesser tuberosity articular margin.

The sutures are passed through the transferred pectoralis tendon using a penetrating grasper or a suture shuttle device. The arm is positioned in approximately 30 degrees of internal rotation and 30 degrees of forward flexion to remove tension from the construct. The medial row knots are tied securely. The suture tails are then brought laterally and secured with knotless anchors on the lateral aspect of the lesser tuberosity, compressing the tendon footprint against the decorticated bone.

The construct is directly visualized and palpated to ensure robust fixation and appropriate tension. The arm is gently taken through a range of motion to confirm stability and assess the safe limits of external rotation, which will dictate the postoperative rehabilitation parameters. The wound is copiously irrigated, and a closed suction drain may be placed deep to the deltopectoral interval if significant dead space or oozing is present. The deltopectoral fascia is loosely approximated, followed by standard layered closure of the subcutaneous tissue and skin.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, pectoralis major transfers are complex reconstructive procedures fraught with potential complications. The surgeon must be acutely aware of these risks, employ rigorous preventative strategies, and possess a clear algorithm for salvage management should complications arise.
The most devastating complication is iatrogenic nerve injury. The musculocutaneous nerve is at the highest risk during the creation of the subcoracoid tunnel. Overzealous blind dissection or failure to maintain a trajectory directly on the anterior scapular neck can lead to traction, compression, or transection of this nerve, resulting in profound weakness of elbow flexion and sensory deficits in the lateral forearm. Similarly, the pectoral nerves are vulnerable to traction injury if the medial mobilization of the pectoralis muscle belly exceeds the 6 to 8 centimeter safety threshold. If a nerve injury is suspected postoperatively, an electromyogram (EMG) should be obtained at 6 to 12 weeks. Most neuropraxic injuries will resolve with observation, but structural lesions may require microsurgical exploration and nerve grafting.
Failure of the transfer construct is another significant concern. This can occur due to anchor pullout from osteoporotic bone, suture breakage, or interstitial tearing of the transferred tendon. Construct failure typically presents as an acute loss of internal rotation strength and a recurrence of the preoperative "lift-off" or "belly-press" signs, often accompanied by a sudden pop or sharp pain during early rehabilitation. Non-compliance with the postoperative immobilization protocol is a leading cause of early failure.
Table 2: Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Musculocutaneous Nerve Injury | 2% - 5% | Blunt, careful dissection deep to conjoint tendon; stay on anterior scapular neck. | Observation for neuropraxia; EMG at 6-12 weeks; microsurgical exploration if no recovery. |
| Pectoral Nerve Injury | 1% - 3% | Strictly limit medial muscle mobilization to <8 cm from humeral insertion. | Irreversible if transected; requires compensatory strengthening of surrounding musculature. |
| Construct Failure / Anchor Pullout | 5% - 10% | Use double-row fixation; decorticate footprint; strict adherence to rehab protocol. | Revision fixation if tissue quality permits; conversion to Reverse Total Shoulder Arthroplasty (RTSA) if severe. |
| Postoperative Stiffness | 10% - 15% | Early, controlled passive ROM within safe zone established intraoperatively. | Aggressive physical therapy; arthroscopic capsular release if refractory after 6-9 months. |
| Infection (Superficial/Deep) | 1% - 2% | Preoperative antibiotics; meticulous hemostasis; minimize OR traffic. | Superficial: Oral antibiotics. Deep: Urgent surgical I&D, culture-specific IV antibiotics. |
| Anterior Escape / Subluxation | 3% - 7% | Ensure proper tensioning of the transfer; subcoracoid routing preferred. | Conversion to RTSA to provide static constraint via semi-constrained biomechanics. |
Postoperative stiffness is a frequent complication, often resulting from prolonged immobilization or an overly tight transfer construct. While a slight loss of terminal external rotation is expected and even desired to protect the reconstruction, profound adhesive capsulitis requires aggressive intervention. Management begins with a prolonged
