Pelvic External Fixation: An Intraoperative Masterclass for Trauma Stabilization

Key Takeaway
Join us in the OR for a masterclass on pelvic external fixation. This guide covers comprehensive surgical anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative execution. We'll delve into precise pin placement, reduction techniques, and frame application. Critical pearls, potential pitfalls, and strategies for managing postoperative complications are thoroughly discussed, ensuring fellows gain a deep understanding of this essential trauma procedure.
Comprehensive Introduction and Patho-Epidemiology
The management of high-energy pelvic ring disruptions represents one of the most formidable challenges in orthopedic trauma surgery. These injuries are rarely isolated; they are hallmarks of massive kinetic energy transfer, typically resulting from motor vehicle collisions, motorcycle crashes, pedestrian-versus-auto incidents, or falls from significant heights. The immediate threat to life is exsanguinating hemorrhage, driven by the profound vascularity of the pelvic basin and the mechanical expansion of the pelvic volume. When the pelvic ring is disrupted, particularly in "open book" or anteroposterior compression (APC) patterns, the true volume of the pelvis increases exponentially. According to the formula for a sphere, even a modest increase in the radius (or diastasis of the symphysis) leads to a massive increase in the volume capable of sequestering blood, effectively abolishing the retroperitoneal tamponade effect that normally arrests venous bleeding.
Understanding the patho-epidemiology of these injuries requires a deep appreciation of the Young-Burgess classification system, which categorizes injuries based on the vector of the deforming force: Anteroposterior Compression (APC), Lateral Compression (LC), Vertical Shear (VS), and Combined Mechanical (CM) mechanisms. APC injuries result in external rotation of the hemipelvis, sequentially tearing the symphysis pubis, the sacrotuberous and sacrospinous ligaments, and finally the anterior sacroiliac ligaments. Lateral compression injuries, conversely, drive the hemipelvis inward, often resulting in impacted sacral fractures and horizontal pubic rami fractures, which paradoxically decrease pelvic volume but can still cause life-threatening visceral or vascular injury due to bony spicules. Vertical shear injuries represent the most severe manifestation of instability, characterized by complete disruption of both the anterior and posterior ligamentous complexes, leading to multidirectional instability of the hemipelvis.
The application of a pelvic external fixator in this acute setting is a masterclass in damage control orthopedics. It is not merely a carpentry exercise of placing pins in bone; it is a life-saving resuscitative maneuver. By manually reducing the pelvic volume and stabilizing the osseous structures, the external fixator restores the boundaries of the retroperitoneal space, facilitating clot formation and promoting hemodynamic stability. Furthermore, it prevents the continuous mechanical disruption of nascent clots that occurs with patient transfers, nursing care, and respiratory excursions. While modern trauma protocols heavily utilize temporary pelvic binders in the pre-hospital and emergency department settings, the external fixator remains the gold standard for durable, provisional (and sometimes definitive) anterior ring stabilization in the rotationally unstable patient.
The epidemiological burden of these injuries is substantial, with mortality rates historically ranging from 10% to 50% in the presence of hemodynamic instability. The advent of standardized multidisciplinary protocols—incorporating early pelvic binding, massive transfusion protocols, interventional radiology for angioembolization, and rapid application of external fixation—has significantly improved survivorship. However, the morbidity associated with these injuries remains high, including chronic pain, leg-length discrepancies, dyspareunia, and profound functional limitations. Therefore, the precision with which we execute our initial stabilization directly influences not only the patient's immediate survival but also their long-term functional outcome and the feasibility of subsequent definitive internal fixation.
Detailed Surgical Anatomy and Biomechanics
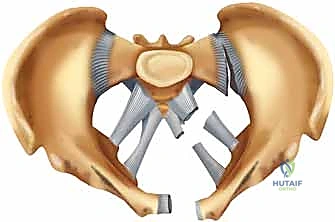
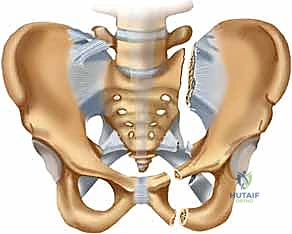
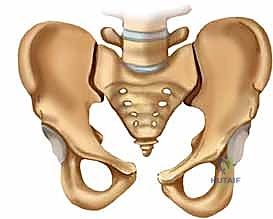
To safely and effectively apply a pelvic external fixator, the orthopedic surgeon must possess an intimate, three-dimensional understanding of pelvic osteology, ligamentous restraints, and the perilous neurovascular landscape. The pelvic ring is an osteoligamentous structure designed to transmit the axial load of the torso from the sacrum to the lower extremities via the acetabula. It is composed of the sacrum and the paired innominate bones (ilium, ischium, and pubis). However, the osseous architecture alone provides minimal inherent stability; the pelvis relies almost entirely on its robust ligamentous complexes to maintain structural integrity under physiologic loads.
The concept of the "posterior tension band" is paramount in understanding pelvic biomechanics. The posterior pelvic ring is stabilized by the strongest ligaments in the human body. The interosseous sacroiliac ligaments form the primary defense against vertical shear forces, suspending the sacrum between the ilia. The posterior sacroiliac ligaments, running from the posterior superior iliac spine (PSIS) to the sacrum, resist both rotational and vertical displacement. Anteriorly, the symphysis pubis acts as a strut, resisting external rotation forces. The pelvic floor ligaments—the sacrotuberous and sacrospinous ligaments—act as secondary stabilizers, preventing excessive flexion of the sacrum and resisting external rotation of the hemipelvis. Disruption of the anterior structures alone (e.g., APC II) leads to rotational instability, while combined anterior and posterior disruption (e.g., APC III, VS) results in catastrophic multidirectional instability.
Navigating the neurovascular anatomy during pin placement is fraught with hazard. The internal iliac artery and its branches are the primary sources of arterial hemorrhage in pelvic trauma. The superior gluteal artery is particularly vulnerable as it exits the greater sciatic notch, often injured by displaced posterior ring fractures or during aggressive posterior reduction maneuvers. However, it is the presacral and paravesical venous plexuses that are responsible for up to 90% of pelvic hemorrhage. These valveless veins are easily torn by shearing forces and bleed profusely into the expanded retroperitoneal space. The application of an anterior external fixator indirectly addresses this venous bleeding by reducing the pelvic volume and providing a stable environment for tamponade.
Neurologically, the lumbosacral plexus lies in close proximity to the sacroiliac joint and the anterior sacral ala, making it highly susceptible to stretch or transection injuries. For the anterior approach to external fixation, the lateral femoral cutaneous nerve (LFCN) is the structure most at risk. The LFCN typically exits the pelvis medial to the anterior superior iliac spine (ASIS), passing under or through the inguinal ligament. However, anatomical variants are common, and the nerve may drape directly over the ASIS or the anterior iliac crest. Iatrogenic injury during iliac crest pin placement leads to meralgia paresthetica—a painful dysesthesia of the anterolateral thigh that can be severely debilitating. Similarly, the femoral nerve, lying in the iliopsoas groove, can be injured if supra-acetabular pins are placed too medially or plunge too deeply through the inner table of the ilium.
Exhaustive Indications and Contraindications
The decision to apply a pelvic external fixator must be deliberate, guided by the patient's hemodynamic status, the specific injury pattern, and the overall trajectory of their polytrauma care. The primary indication is the acute resuscitation of a hemodynamically unstable patient with a rotationally unstable pelvic ring disruption (APC II, APC III, and certain LC patterns with profound internal rotation or contralateral "windswept" deformities). In these scenarios, the external fixator acts as an adjunct to damage control resuscitation, rapidly decreasing pelvic volume and stabilizing the bony elements to facilitate clot formation.
Beyond acute resuscitation, external fixation serves as a vital tool for provisional stabilization. In patients with severe vertical shear injuries or highly comminuted posterior ring disruptions, definitive internal fixation may be delayed due to patient physiology, associated injuries (e.g., traumatic brain injury, pulmonary contusions), or soft tissue compromise (e.g., Morel-Lavallée lesions). Here, the external fixator maintains gross alignment, facilitates nursing care, allows for upright positioning to improve pulmonary mechanics, and prevents further soft tissue envelope degradation until definitive osteosynthesis can be safely undertaken.
In highly selected cases, pelvic external fixation can serve as the definitive treatment. This is most commonly applicable in isolated APC II injuries (symphyseal diastasis with intact posterior tension bands) where the patient is not a candidate for anterior symphyseal plating due to severe suprapubic soft tissue injury, urological contamination (e.g., open bladder rupture, urethral avulsion requiring suprapubic tube), or extreme physiological frailty. If utilized definitively, the frame must be robustly constructed and maintained for a minimum of 6 to 12 weeks to allow for adequate ligamentous healing.
Indications and Contraindications Matrix
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Absolute Indications | Hemodynamically unstable patient with "open book" (APC II/III) pelvic fracture. | Rapid reduction of pelvic volume to achieve retroperitoneal tamponade and arrest venous hemorrhage. |
| Relative Indications | Provisional stabilization of vertically unstable (VS) fractures prior to definitive ORIF. | Facilitates nursing care, pulmonary toilet, and prevents ongoing soft tissue trauma from mobile bony fragments. |
| Definitive Indications | APC II injuries with severe anterior urogenital contamination or compromised anterior soft tissues. | Avoids placing internal hardware through a contaminated or compromised surgical field. |
| Absolute Contraindications | Severe comminution of the iliac wings or supra-acetabular corridors precluding safe pin purchase. | Pins will fail to achieve purchase, potentially displacing fracture fragments or entering the hip joint/viscera. |
| Relative Contraindications | Planned definitive anterior internal fixation within 24-48 hours in a hemodynamically stable patient. | Pin tracts may contaminate the surgical field for planned symphyseal or quadrilateral surface plating. |
| Relative Contraindications | Morbid obesity with massive abdominal pannus. | Pannus may rest on the frame, causing pressure necrosis, pin tract infections, and loss of reduction. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful pelvic external fixation, even in the acute trauma setting where time is of the essence. The process begins in the trauma bay with the Advanced Trauma Life Support (ATLS) protocol. If a pelvic binder was applied pre-hospital or in the emergency department, it should remain in place until the surgical team is ready to prep and drape, or until it is systematically replaced by the external fixator in the operating room. Premature removal of the binder can lead to a catastrophic loss of tamponade and sudden hemodynamic collapse.
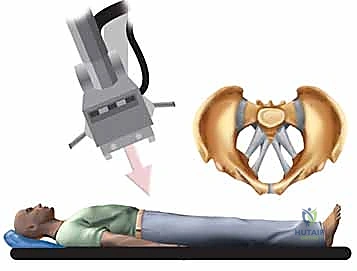
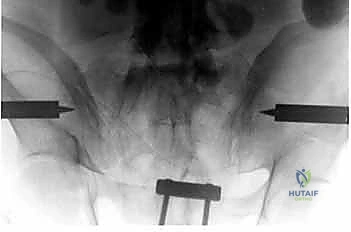
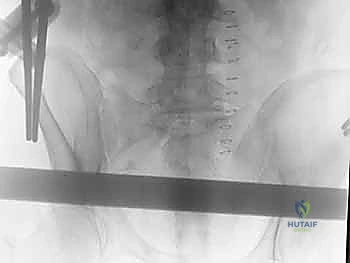
Radiographic evaluation is critical for preoperative templating. The standard trauma anteroposterior (AP) pelvis radiograph is the initial screening tool. In a hemodynamically unstable patient, this single view is sufficient to diagnose an "open book" injury and justify immediate external fixation. However, whenever the patient's physiology permits, dedicated pelvic inlet and outlet views should be obtained.
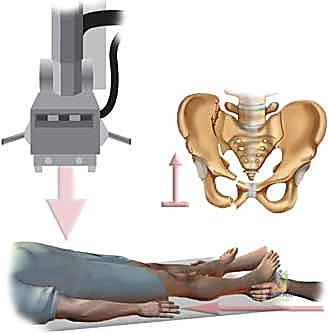
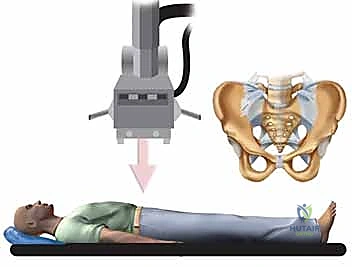
The Inlet view, taken with the beam angled 45 degrees caudad, provides a true axial perspective of the pelvic ring. It is indispensable for assessing anterior-posterior translation, rotational deformity, and impaction of the sacrum.
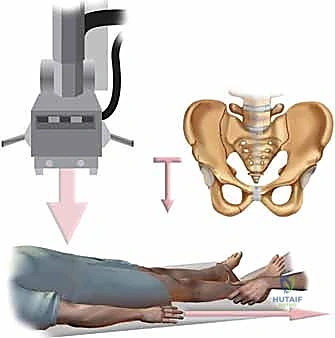
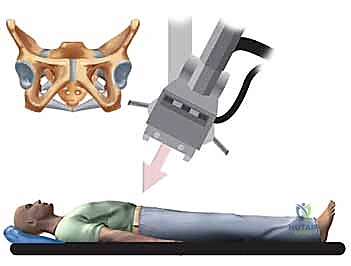
The Outlet view, taken with the beam angled 45 degrees cephalad (perpendicular to the anterior surface of the sacrum), is the best view for assessing vertical translation of the hemipelvis and identifying sacral foraminal fractures.
If a preoperative CT scan is available, it provides unparalleled three-dimensional understanding of the fracture morphology, particularly the integrity of the osseous corridors required for pin placement.
Patient positioning must facilitate both the surgical approach and unhindered fluoroscopic imaging. The patient is positioned supine on a fully radiolucent Jackson table or a standard operating table with a radiolucent extension. The arms should be positioned at 90 degrees or secured across the chest to allow the C-arm to arc freely over the pelvis. A Foley catheter must be inserted prior to prepping to decompress the bladder, moving it out of the retropubic space and away from potential aberrant pin trajectories. The abdomen, pelvis, and bilateral thighs down to the knees are prepped and draped in a standard sterile fashion. The C-arm is typically brought in from the side opposite the surgeon, and its mobility (ability to obtain AP, Inlet, Outlet, and oblique views) must be confirmed before the first incision.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative execution of pelvic external fixation relies on the utilization of one of two primary osseous corridors: the iliac crest or the supra-acetabular (anterior inferior iliac spine - AIIS) pathway. The choice of corridor dictates the surgical approach, the fluoroscopic views required, and the ultimate biomechanical stability of the construct. Biomechanical studies have consistently demonstrated that supra-acetabular pins offer superior pull-out strength and construct rigidity compared to iliac crest pins, primarily due to the dense column of bone extending from the AIIS to the posterior superior iliac spine (PSIS).

The Iliac Crest Technique
The iliac crest technique involves placing pins into the gluteal pillar, the thickest portion of the anterior ilium. While technically less demanding regarding fluoroscopy, it is fraught with risks of LFCN injury and pin pull-out in osteoporotic bone.
The procedure begins with a 2-3 cm longitudinal incision centered over the anterior iliac crest, starting approximately 2 cm posterior to the ASIS. This posterior starting point is critical to avoid the converging inner and outer tables at the very tip of the ASIS and to minimize the risk to the LFCN.

Blunt dissection is carried down through the subcutaneous tissues to the fascial layer. The fascia is incised longitudinally, and the periosteum is elevated minimally to expose the bony crest. Using a drill sleeve to protect the soft tissues, a starting hole is made.
The trajectory of the pin is paramount; it must be directed between the inner and outer tables of the ilium. The surgeon must aim towards the thickest bone, which generally requires directing the drill slightly medial and inferior, aiming roughly toward the greater sciatic notch.
Fluoroscopic guidance (Obturator Oblique and Iliac Oblique views) can be utilized to confirm that the drill has not breached the cortices. Typically, two 5.0 mm or 6.0 mm half-pins are placed in each iliac crest to provide sufficient stability.

The Supra-Acetabular Technique
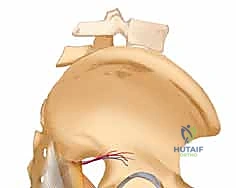
The supra-acetabular technique is the preferred method for modern trauma surgeons due to its robust biomechanical profile. The target is the dense bone corridor running from the AIIS to the PSIS, directly above the acetabular dome.

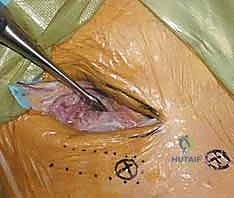
A 2 cm vertical incision is made starting at the level of the ASIS and extending distally, directly over the palpable AIIS. Blunt dissection separates the sartorius and tensor fasciae latae, taking extreme care to retract the lateral femoral cutaneous nerve medially or laterally depending on its anatomical variant.

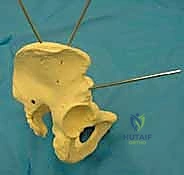
The starting point is critical and must be confirmed fluoroscopically. The C-arm is positioned in an Obturator Oblique Outlet view (often referred to as the "teardrop view"). This view looks directly down the dense osseous corridor above the hip joint.

A guide wire or drill is placed on the AIIS, and its position is confirmed to be superior to the acetabulum and centered within the teardrop.

Once the starting point is confirmed, the drill is advanced. The C-arm is then switched to an Iliac Oblique Inlet view. This orthogonal view ensures that the drill is contained between the inner and outer tables of the ilium and is not plunging into the true pelvis (endangering the external iliac vessels and internal organs) or exiting laterally into the gluteal musculature.
The drill is advanced to a depth of approximately 50-60 mm, and a 5.0 mm or 6.0 mm Schanz pin is inserted.
This process is repeated on the contralateral side.


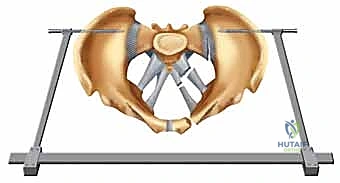
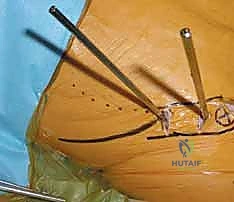
Frame Construction and Reduction
Once the pins are securely placed, the external frame is constructed. The configuration of the frame depends on the patient's body habitus and the required stability. A simple single-bar construct may suffice for provisional stabilization, while a double-bar or A-frame construct provides enhanced rigidity for definitive management.

Carbon fiber rods are cut to the appropriate length and connected to the pins using multi-pin clamps or pin-to-rod couplings.


The reduction maneuver is the critical final step. For an "open book" (APC) injury, the goal is to internally rotate the hemipelves to close the symphyseal diastasis and reduce pelvic volume.

This is achieved by applying manual compression across the greater trochanters while simultaneously tightening the clamps on the external fixator rod.
The surgeon must be careful not to over-compress, which can lead to overlapping of the symphysis pubis and iatrogenic internal rotation deformities.

Fluoroscopy (AP and Inlet views) must be used to confirm the adequacy of the reduction before final tightening of all connections.


The final construct should be rigid, allowing the nursing staff to log-roll the patient without loss of reduction.

Clearance between the frame and the abdomen must be verified to allow for abdominal distension and to prevent pressure necrosis, particularly in obese patients.











Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, pelvic external fixation is associated with a specific profile of complications. Recognizing these risks early and implementing appropriate salvage strategies is crucial for optimizing patient outcomes. The most ubiquitous complication is pin tract infection, which occurs in a significant percentage of cases, particularly when the fixator is used definitively over several weeks.
Superficial pin tract infections typically present with erythema, serous discharge, and localized pain. These are generally managed successfully with intensified local pin care and oral antibiotics covering common skin flora (e.g., first-generation cephalosporins). However, deep infections or osteomyelitis can occur, presenting with purulent drainage, systemic signs of infection, and radiographic evidence of bone resorption around the pin. Deep infections require immediate hardware removal, aggressive surgical debridement of the pin tract, and intravenous antibiotics.
Aseptic loosening of the pins is another frequent complication, often secondary to micromotion at the pin-bone interface or placement in osteoporotic bone. Loosening compromises the stability of the construct, leading to loss of reduction and recurrent pelvic volume expansion. Clinically, this presents as a palpable toggle of the pins or increasing pain with mobilization. Salvage involves removing the loose pins and either replacing them in a different osseous corridor (e.g., switching from iliac crest to supra-acetabular) or expediting conversion to definitive internal fixation if the patient's physiological status permits.
Iatrogenic neurovascular injury, while less common, carries devastating consequences. Injury to the Lateral Femoral Cutaneous Nerve (LFCN) during iliac crest pin placement
