Optimize Twopart Surgical Neck Fracture Fixation with IM Nailing
Key Takeaway
Here are the crucial details you must know about Optimize Twopart Surgical Neck Fracture Fixation with IM Nailing. A twopart surgical neck fracture is a common type of proximal humerus fracture, classified by Neer, where the humeral head and tuberosities remain attached, separated from the shaft. Displaced, unstable twopart surgical neck fractures often require operative management, including reduction and internal fixation. Intramedullary nails, such as the Aequalis system, are effectively used to stabilize these fractures, optimizing tuberosity and head fixation.
Comprehensive Introduction and Patho-Epidemiology
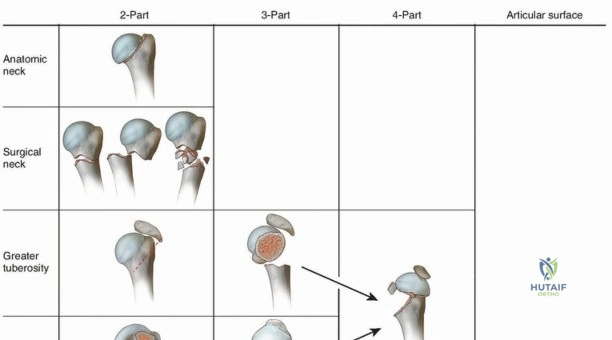
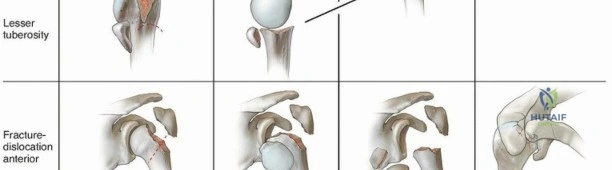
Fractures of the proximal humerus represent a significant and growing proportion of orthopedic trauma, particularly within the aging demographic. According to the foundational Neer classification system, these fractures are categorized into two-, three-, or four-part patterns based on the displacement of the four major anatomic segments: the humeral head, the greater tuberosity, the lesser tuberosity, and the humeral shaft. Epidemiological data indicate that 50% to 80% of all proximal humerus fractures present as nondisplaced or minimally displaced and possess inherent osseous stability. For this majority, non-operative management—typically consisting of a short period of immobilization in neutral rotation to prevent malunion, followed by a rigorously structured early mobilization protocol—is sufficient to yield satisfactory clinical and functional outcomes. However, the remaining 20% to 50% of these injuries involve displaced, highly unstable two-, three-, or four-part fracture patterns that profoundly disrupt shoulder biomechanics.
For patients presenting with unstable two-part surgical neck fractures—or more complex three- and four-part variants where a vascularized, attached articular head fragment remains viable—operative management via open reduction and internal fixation (ORIF) or intramedullary (IM) nailing is strongly indicated. Historically, the surgical management of these fractures has been fraught with high complication rates. Extensive surgical dissection, coupled with inadequate biomechanical fixation in the context of severe localized soft tissue trauma, advanced osteopenia, and iatrogenic devascularization, are the most commonly cited etiologies for the mechanical failure of internal fixation devices. The delicate balance between achieving rigid osseous stability and preserving the tenuous vascular supply to the humeral head remains the central challenge in proximal humerus fracture surgery.
In recent years, the orthopedic community has seen highly encouraging reports regarding the utilization of modern locked intramedullary nails for the treatment of two-, three-, and select four-part proximal humerus fractures. Newer generations of intramedullary devices have been meticulously engineered to permit stable, load-sharing fixation of the humeral head to the diaphyseal shaft while simultaneously maximizing the biomechanical capture and fixation of the tuberosities. By utilizing a minimally invasive, rotator cuff-splitting or superior transdeltoid approach, surgeons can effectively bypass the extensive soft-tissue stripping traditionally associated with standard deltopectoral plating. Implants such as the Aequalis intramedullary nail (Tornier, Inc., Bloomington, MN) exemplify this modern design philosophy. This specific intramedullary stabilization device is tailored specifically to optimize tuberosity fragment fixation, provide unyielding subchondral support for the humeral head, and dramatically improve proximal humeral reconstruction in osteoporotic bone.

The pathogenesis of proximal humerus fractures typically involves either a direct blow to the anterior, lateral, or posterolateral aspect of the shoulder, or, more commonly in the osteoporotic population, an axial load transmitted vertically through the humerus during a fall onto an outstretched hand. This axial load frequently results in a valgus-impacted fracture pattern. In younger cohorts, high-energy trauma dominates the etiologic spectrum. Furthermore, violent, uncoordinated muscle contractures—such as those experienced during grand mal seizures or severe electrical shock—are classically associated with posterior fracture-dislocations and severe impaction injuries, driven by the overpowering force of the internal rotators and adductors. Regardless of the mechanism, minor losses in humeral length or alterations in the critical length-tension relationship of the deltoid and rotator cuff musculature can precipitate profound functional deficits.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
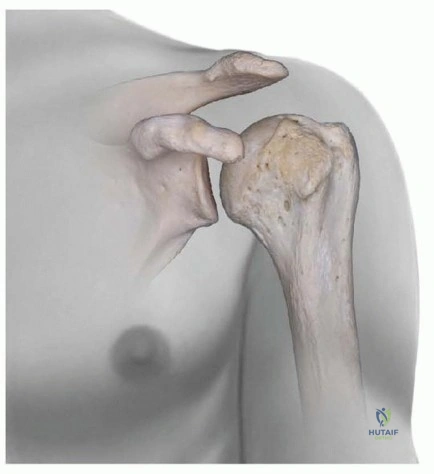
A profound understanding of the complex osteology of the proximal humerus is an absolute prerequisite for successful intramedullary nailing. The proximal humerus is composed of four distinct anatomic regions: the articular humeral head, the lesser tuberosity (LT), the greater tuberosity (GT), and the proximal humeral metaphysis. In a native, uninjured shoulder, the superior articular surface of the humeral head sits anatomically higher than the superior margins of the tuberosities. Any iatrogenic or post-traumatic alteration in this delicate spatial relationship will inevitably result in subacromial impingement and severely compromised biomechanical function. Morphologically, the center of the humeral head is offset slightly medial (approximately 3 mm) and posterior (approximately 7 mm) in relation to the central axis of the humeral diaphysis. Furthermore, the articular surface is retroverted approximately 30 degrees (with a normal population variance ranging from 20 to 60 degrees) relative to the epicondylar axis of the distal humerus. The bicipital groove, housing the long head of the biceps tendon, acts as the primary anatomic landmark separating the lesser and greater tuberosities. Notably, the densest and hardest bone in the proximal humerus is located directly within the floor and walls of the bicipital groove, dictating that most fractures of the greater tuberosity occur just posterior to this robust bony strut.
Vascular Supply of the Proximal Humerus
The vascular anatomy of the proximal humerus is notoriously precarious and is the primary determinant of post-traumatic humeral head viability. The anterior and posterior humeral circumflex arteries, both vital branches of the axillary artery, provide the dominant arterial inflow. Historically, the arcuate artery—the terminal intraosseous continuation of the ascending branch of the anterior humeral circumflex artery—was considered the primary blood supply to the humeral head. Avascular necrosis (AVN) was thought to be an almost inevitable consequence if this specific vessel was disrupted, particularly in true anatomic neck fractures. However, contemporary microvascular studies have definitively demonstrated that the posterior humeral circumflex artery plays a far more critical role, often serving as the primary source of intraosseous blood supply to the fractured humeral head in the majority of clinical scenarios. Consequently, meticulous surgical care must be taken to prevent iatrogenic devascularization of the posterior capsule and the attached tuberosity fragments. While the initial traumatic vascular insult cannot be undone, the implementation of well-planned, minimally invasive intramedullary nailing techniques drastically reduces the risk of secondary iatrogenic damage, thereby mitigating the incidence of delayed union, nonunion, and catastrophic avascular necrosis.
Neurologic Considerations
The proximity of the brachial plexus and its terminal branches places the neurologic integrity of the upper extremity at significant risk during both the initial traumatic event and subsequent operative interventions. A thorough, meticulously documented preoperative neurologic evaluation is mandatory for every patient presenting with a proximal humerus fracture. The axillary nerve is particularly vulnerable; it courses posteriorly through the quadrilateral space, placing it at high risk for traction neuropraxia or complete transection during severe fracture-dislocations. Furthermore, during intramedullary nailing, the lateral entry site utilized for distal locking screw fixation—typically located 4 to 5 cm distal to the lateral edge of the acromion—places the descending branches of the axillary nerve at direct iatrogenic risk. Surgeons must utilize blunt dissection techniques and protective soft-tissue sleeves when drilling and inserting these distal interlocking screws to prevent devastating denervation of the deltoid muscle.
Biomechanics of Deforming Forces
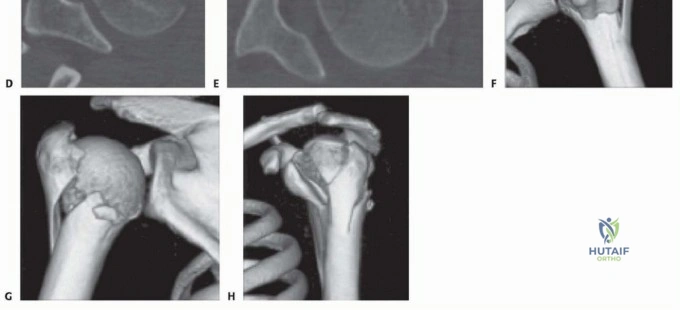
In unstable two-, three-, and four-part proximal humerus fractures, the predictable patterns of fragment displacement are dictated entirely by the unopposed pull of the rotator cuff musculature inserting onto the tuberosities. In a classic surgical neck fracture, the pectoralis major exerts a powerful anteromedial pull on the humeral shaft, displacing it medially. Concurrently, in fractures where the tuberosities are separated from the articular segment, the greater tuberosity is violently retracted posteromedially and superiorly by the combined forces of the supraspinatus, infraspinatus, and teres minor muscles. Conversely, the lesser tuberosity is forcefully pulled anteromedially by the robust subscapularis muscle. In four-part proximal humerus fractures, advanced 3D imaging has demonstrated that the primary vertical fracture plane separating the tuberosities is almost universally located posterior to the bicipital groove, and that the principal displacement of these fragments occurs primarily in the transverse (horizontal) plane. Failure to anatomically reduce and rigidly fix the greater tuberosity inevitably leads to definitive retraction, fatty infiltration, and irreversible atrophy of the external rotators, culminating in a pseudoparalyzed, deeply dysfunctional shoulder. Therefore, modern intramedullary nailing techniques prioritize the anatomic reduction and absolute stability of the tuberosities over the perfect restoration of the articular segment, as a healed tuberosity complex can often compensate for mild articular incongruity or partial avascular necrosis.


Exhaustive Indications and Contraindications
The decision algorithm for treating proximal humerus fractures must be highly individualized, taking into account fracture morphology, bone quality, patient age, functional demands, and medical comorbidities. Intramedullary nailing is primarily indicated for displaced or highly unstable two-part surgical neck fractures where the humeral head remains attached to the tuberosities but is displaced from the diaphyseal shaft. Nailing is particularly advantageous in cases exhibiting medial calcar comminution, where standard lateral locking plates often fail due to excessive varus bending moments. Furthermore, modern straight intramedullary nails are heavily indicated for select three-part and valgus-impacted four-part fractures, provided the surgeon possesses the advanced technical proficiency required to capture and secure the tuberosity fragments to the proximal nail body using heavy non-absorbable sutures.
Conversely, there are strict absolute and relative contraindications to the use of intramedullary nails in this anatomic region. Absolute contraindications include true head-splitting fractures where the articular surface is severely comminuted into multiple un-reconstructable fragments, as well as scenarios involving a completely devascularized, extruded humeral head fragment devoid of any soft tissue attachments (the classic "anatomical neck" fracture). Active local or systemic infection is an absolute contraindication to any internal implant. Relative contraindications include severe, end-stage osteoporosis where the proximal cancellous bone is virtually absent, making screw purchase within the humeral head impossible. In such extreme osteoporotic cases, particularly in elderly, low-demand patients with complex four-part fractures, primary reverse total shoulder arthroplasty (RTSA) is often the more reliable and definitive surgical option.
When evaluating a patient for surgical intervention, a comprehensive history and physical examination are paramount. Associated injuries are exceedingly common and can drastically alter the surgical plan. The surgeon must maintain a high index of suspicion for concomitant rotator cuff tears, glenohumeral dislocations, ipsilateral forearm fractures (constituting a "floating arm"), and occult brachial plexus or axillary nerve injuries, which are documented in 5% to 30% of complex proximal humerus fractures. Additionally, entrapment or subluxation of the long head of the biceps tendon within the fracture site is a frequent occurrence that must be addressed intraoperatively, typically via tenodesis, to prevent chronic postoperative anterior shoulder pain.
Below is a comprehensive summary of the indications and contraindications for intramedullary nailing of proximal humerus fractures:
| Category | Specific Clinical Scenarios |
|---|---|
| Primary Indications | - Displaced 2-part surgical neck fractures (>1cm translation or >45° angulation) - Unstable 2-part fractures failing conservative management - Select 3-part fractures (especially with intact medial hinge) - Valgus-impacted 4-part fractures in physiologically young/active patients - Fractures with severe medial calcar comminution |
| Relative Contraindications | - Severe, unremitting osteopenia (cortical thickness < 3mm) - Pre-existing advanced glenohumeral osteoarthritis - Concomitant massive, irreparable rotator cuff arthropathy - Uncooperative patient incapable of following postoperative rehab |
| Absolute Contraindications | - True head-splitting articular fractures - Extruded, completely devascularized anatomic neck fractures - Active local soft tissue or glenohumeral joint infection - Pathologic fractures secondary to active primary bone malignancy |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive Imaging Protocols
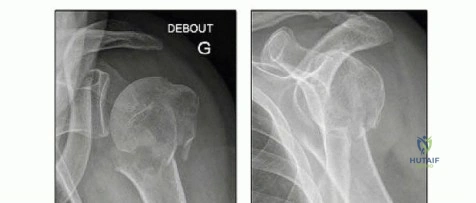
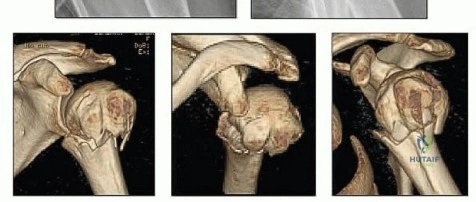
The foundation of a successful intramedullary nailing procedure lies in exhaustive preoperative imaging and meticulous surgical templating. A standard trauma radiographic series is mandatory, comprising a true anteroposterior (AP) view of the scapula (Grashey view), a trans-scapular Y-view, and an axillary lateral view. The axillary view is absolutely critical for evaluating the spatial relationship of the humeral head to the glenoid, ruling out subtle posterior or anterior dislocations, and assessing the degree of tuberosity displacement in the transverse plane. Due to the complex, multi-planar nature of these injuries, a high-resolution Computed Tomography (CT) scan with 3D reconstructions is now considered the standard of care for all three- and four-part fractures. The 3D CT scan allows the surgeon to definitively characterize the fracture geometry, assess the exact volume of the articular segment, identify the presence of medial calcar comminution, and preoperatively map the trajectory of the deforming muscular forces.


Digital Templating and Implant Selection
Once optimal imaging is obtained, rigorous digital templating must be performed. The surgeon must determine the appropriate nail diameter by measuring the narrowest point of the humeral diaphysis on the AP and lateral radiographs, ensuring the selected nail will pass without causing iatrogenic hoop stresses or diaphyseal fracture. Nail length is calculated to ensure the distal locking screws bypass the fracture site by at least two cortical diameters, terminating in healthy, structurally sound diaphyseal bone. The entry point for modern straight nails is typically located at the apex of the humeral head, slightly medial to the greater tuberosity and directly in line with the intramedullary canal. Precise preoperative identification of this entry point on the 3D CT scan is crucial, as an eccentric starting hole will inevitably lead to varus or valgus malalignment of the proximal segment during nail insertion.
Patient Positioning and Operating Room Setup
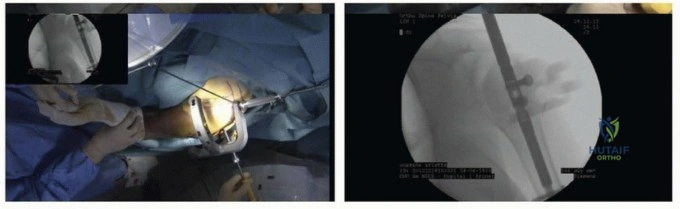
Successful intramedullary nailing of the proximal humerus is highly dependent on flawless integration between the surgical team, the fluoroscopy technician, and patient positioning. The patient is placed supine in the beach-chair position on a fully radiolucent operating table. The torso is elevated to an angle of 60 to 70 degrees. It is imperative that the patient is shifted laterally so that the operative shoulder extends completely off the edge of the radiolucent table, allowing unrestricted access for the C-arm and the surgeon. A small bolster or rolled towel is placed beneath the medial border of the ipsilateral scapula to protract the shoulder girdle and elevate it from the table.
Intraoperative Fluoroscopy Management
The C-arm fluoroscopy unit must be positioned at the head of the bed, coming in from the contralateral side, or positioned parallel to the patient on the operative side, depending on the specific base geometry of the C-arm. The setup must allow the surgeon to obtain perfect, orthogonal AP and axillary views without having to dramatically manipulate the fractured extremity. Extension of the shoulder is frequently required to gain unrestricted access to the superior entry site in the humeral head; therefore, the draping and positioning must accommodate at least 30 degrees of unobstructed shoulder extension. When treating patients with complex, borderline reconstructable fractures, the surgeon must obtain documented preoperative consent for a possible conversion to a hemiarthroplasty or reverse shoulder arthroplasty, and the appropriate arthroplasty sets must be sterilized and available in the operating room prior to incision.
Step-by-Step Surgical Approach and Fixation Technique
Selection of the Surgical Approach
Each specific pattern of proximal humerus fracture—be it a simple two-part surgical neck fracture or a complex valgus-impacted four-part variant—presents unique pathophysiologic challenges and requires a tailored surgical approach. Three primary surgical approaches are utilized for intramedullary nailing, dictated by the fracture morphology and the necessity for direct tuberosity manipulation. The percutaneous approach, involving a blunt split of the deltoid and supraspinatus through a minimal 1-cm superior incision, is reserved exclusively for un-comminuted two-part fractures that do not require independent tuberosity fixation. The deltopectoral approach is occasionally utilized for three-part fractures involving the lesser tuberosity, allowing excellent anterior visualization. However, for complex cases involving the greater tuberosity, such as a valgus-impacted four-part fracture, the superior transdeltoid approach is the gold standard. This approach permits direct, orthogonal access to the intramedullary canal while simultaneously providing excellent visualization of the rotator cuff insertions for meticulous tuberosity reduction and suture fixation.
The Superior Transdeltoid Approach
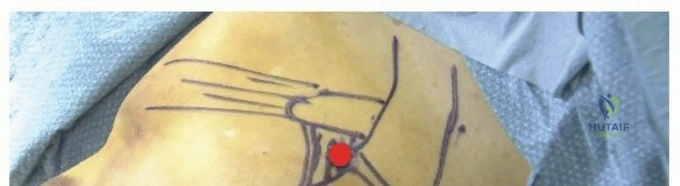
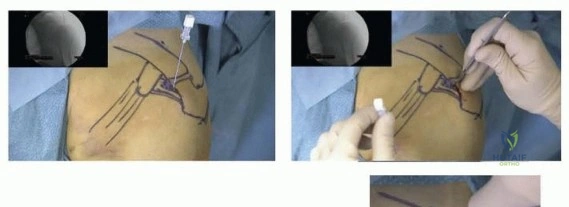
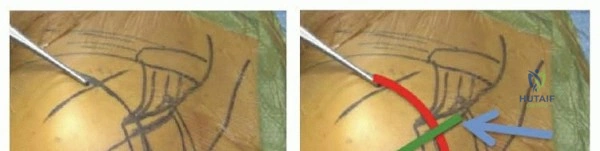
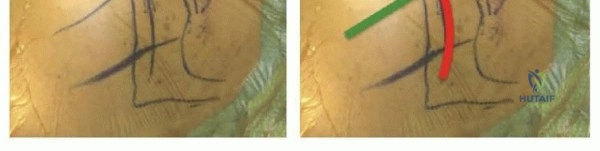
To execute the superior transdeltoid approach, a saber incision is meticulously planned in line with Langer’s lines, centered over the palpable division between the anterior and middle thirds of the deltoid muscle. This raphe is typically located just lateral to the anterolateral corner of the acromion. The skin and subcutaneous tissues are incised, and full-thickness flaps are developed. With the arm held in slight abduction to relieve resting tension on the deltoid, a precise split is developed between the anterior and middle deltoid fibers using electrocautery. It is absolutely critical that this deltoid split extends no more than 4 cm distal to the lateral edge of the acromion to strictly avoid devastating iatrogenic injury to the traversing axillary nerve. To facilitate optimal exposure of the superior rotator cuff without compromising the deltoid insertion, a small, controlled osteotomy of the anterior acromion can be performed using an oscillating saw and completed with a fine osteotome.
Fracture Reduction and Joint Preparation
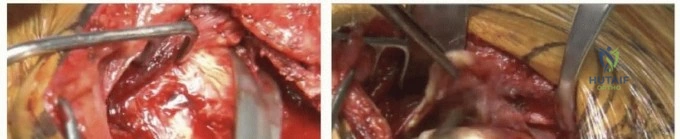
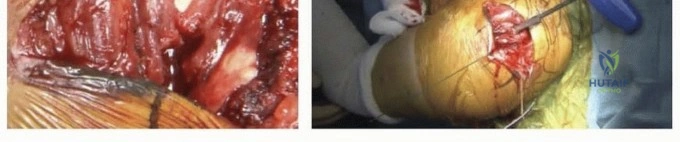
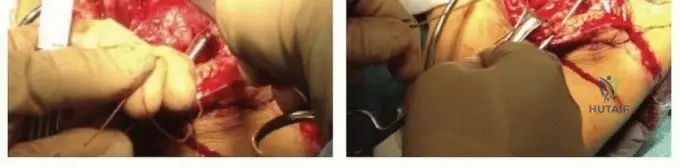
Once the subacromial space is accessed, Gelpi self-retaining retractors are carefully deployed to maintain exposure. A blunt Hohmann retractor is gently placed over the coracoid process to assist in the complete resection of the hypertrophic subacromial bursa. Meticulous bursectomy is essential to visualize the fracture fragments, specifically the greater tuberosity, lesser tuberosity, and the articular head. The surgeon must operate strictly deep to the deltoid fascia to ensure the axillary nerve branches remain undisturbed. At this stage, the long head of the biceps tendon is identified within the bicipital groove. Because the biceps tendon is frequently entrapped within the fracture hematoma or interposed between fragments, it is routinely tenodesed to the superior border of the pectoralis major tendon or the conjoint tendon, and the intra-articular portion is sharply excised. This prevents chronic postoperative biceps tenosynovitis and removes a major barrier to anatomic reduction. Heavy, non-absorbable traction sutures (e.g., #2 or #5 FiberWire) are then placed through the osseotendinous junctions of the supraspinatus/infraspinatus (for the GT) and the subscapularis (for the LT) to act as joysticks for fragment manipulation.
Nail Insertion and Tuberosity Fixation
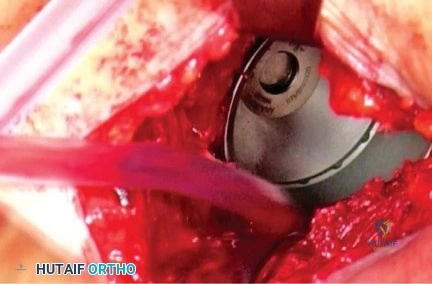
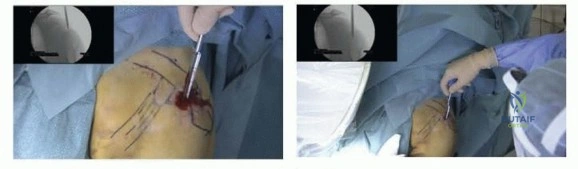
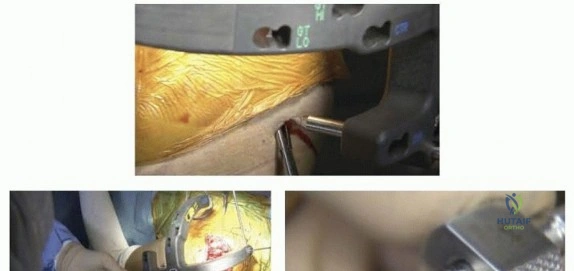
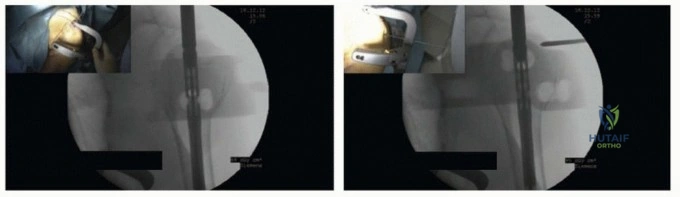
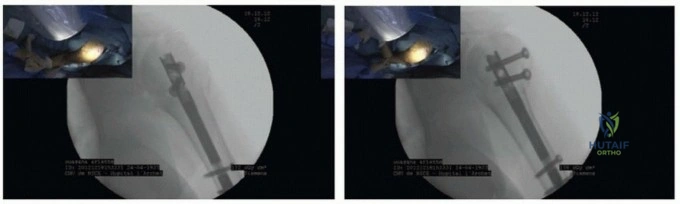
For all approaches utilizing a modern straight intramedullary nail, the entry portal must be established medially, either directly through the muscular fibers of the supraspinatus or slightly anteriorly through the rotator interval. Under live, orthogonal fluoroscopic guidance, a sharp awl or guide pin is introduced at the absolute apex of the humeral head, strictly avoiding the lateral greater tuberosity footprint to prevent varus malalignment. The entry portal is subsequently enlarged with a rigid cannulated reamer. The fracture is then reduced using manual traction, closed manipulation, and the previously placed tuberosity stay sutures. The selected intramedullary nail is passed across the fracture site into the diaphysis. Proximal locking screws are inserted through the nail, intentionally designed to capture and compress the tuberosity fragments against the central articular segment. Crucially, the heavy non-absorbable sutures previously passed through the rotator cuff are now systematically tied through the dedicated suture eyelets located on the proximal aspect of the nail. This creates a biomechanically robust, load-sharing construct that neutralizes the deforming forces of the rotator cuff and guarantees absolute stability of the tuberosities during the critical early phases of bone healing. Finally, distal interlocking screws are placed using a radiolucent targeting guide, employing blunt dissection to protect the axillary and radial nerves.
Complications, Incidence Rates, and Salvage Management
Despite significant advancements in implant design and surgical technique, intramedullary nailing of proximal humerus fractures carries a distinct profile of potential postoperative complications. The surgeon must be acutely aware of these risks, actively employ techniques to minimize their occurrence, and possess the requisite skill set to manage them when they inevitably arise. Complications can be broadly categorized into biologic failures (such as avascular necrosis and nonunion), mechanical/hardware-related failures (such as screw cut-out, nail prominence, and loss of reduction), and iatrogenic neurovascular injuries.
Avascular necrosis (AVN) of the humeral head remains a dreaded complication, particularly in three- and four-part fractures where the delicate posterior humeral circumflex artery is compromised. While modern nailing techniques minimize secondary soft-tissue stripping, the initial traumatic insult dictates the baseline risk. AVN rates following nailing of complex fractures range from 4% to 15%. Interestingly, if the tuberosities heal anatomically to the shaft, partial AVN is often surprisingly well-tolerated clinically, provided there is no secondary screw penetration into the glenohumeral joint. Hardware prominence is another frequent issue; if the nail is left proud (protruding above the articular surface), it will cause severe subacromial impingement, rotator cuff attrition, and intractable pain, necessitating premature hardware removal.
Mechanical failure, specifically varus collapse of the humeral head and subsequent superior cut-out of the proximal locking screws, occurs most frequently in patients with profound osteoporosis or when the surgeon fails to achieve adequate medial calcar reduction. Iatrogenic neurologic injury, particularly to the axillary nerve during distal locking screw insertion or excessive distal extension of the deltoid split, occurs in approximately 1% to 3% of cases. When primary intramedullary nailing fails catastrophically—due to deep infection, painful AVN with joint collapse, or severe tuberosity nonunion—salvage management is exceedingly complex. In the elderly or low-demand patient, the definitive salvage procedure is conversion to a Reverse Total Shoulder Arthroplasty (RTSA). RTSA bypasses the need for a functioning rotator cuff and provides predictable pain relief and functional restoration, though the management of the malunited tuberosities during the revision surgery remains technically demanding.
| Complication Type | Estimated Incidence | Primary Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Avascular Necrosis (AVN) | 4% - 15% | Disruption of posterior humeral circumflex; initial trauma severity | Observation if asymptomatic; Conversion to RTSA or Hemiarthroplasty if painful joint collapse occurs |
| Hardware Prominence / Impingement | 1 |
Clinical & Radiographic Imaging Archive