Intramedullary Nailing of Proximal Humerus Fractures: An Intraoperative Masterclass
Key Takeaway
Step into the operating room for a detailed masterclass on intramedullary nailing of proximal humerus fractures. This guide covers comprehensive anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution. Learn critical techniques for K-wire placement, fragment reduction, guidewire insertion, and reaming, emphasizing neurovascular protection and optimal hardware placement. We also discuss pearls, pitfalls, and postoperative management, ensuring a holistic understanding of this complex procedure.
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a comprehensive exploration of a common yet technically demanding injury: the proximal humerus fracture, specifically focusing on its definitive management utilizing advanced intramedullary nailing techniques. This procedure, when executed with meticulous precision, offers exceptional clinical outcomes, particularly for two-part, three-part, and meticulously selected four-part fractures in younger, active patients. Our overarching objective is to achieve rigid, stable fixation, restore precise anatomical alignment, and critically, preserve the delicate soft tissue envelope and the precarious vascularity of the humeral head.
Comprehensive Introduction and Patho-Epidemiology
Understanding the Injury Burden and Demographics
Proximal humerus fractures represent a massive and growing burden in orthopedic traumatology, accounting for approximately 4% to 5% of all fractures presenting to the emergency department. They currently stand as the third most common fracture in the elderly population, trailing only proximal femur and distal radius fractures. There is a striking bimodal distribution, with a pronounced 4:1 female-to-male ratio in patients over the age of 50. This demographic skew is intrinsically linked to post-menopausal osteoporosis, rendering the proximal humerus highly susceptible to failure under low-energy mechanisms, such as a simple fall from standing height.
Conversely, in younger, physiologically robust patients, these fractures typically result from high-energy trauma mechanisms. Motor vehicle collisions, contact sports injuries, and falls from significant heights generate the immense force required to fracture dense, healthy cortical bone. In this younger cohort, the fracture patterns are often more complex, with a higher incidence of severe comminution, significant displacement, and concomitant soft tissue trauma, demanding a highly aggressive and precise surgical strategy to restore maximal function.
Functional Implications of Pathoanatomy
The clinical significance of these fractures extends far beyond the mere mechanical disruption of osseous integrity. The proximal humerus serves as the critical fulcrum for the shoulder girdle, and even minor alterations in its geometry can precipitate profound functional deficits. Specifically, losses in humeral length between the articular head and the deltoid tuberosity insertion can drastically alter the deltoid's length-tension ratio. A shortened humerus leaves the deltoid mechanically disadvantaged, leading to significant, often permanent, active forward elevation weakness and accelerated fatigue.
Furthermore, the displacement of the greater and lesser tuberosities directly compromises the rotator cuff force couples. The supraspinatus, infraspinatus, and subscapularis rely on precise anatomical insertion points to maintain dynamic glenohumeral stability. When these tuberosities heal in a malunited position, the resulting kinematic imbalance leads to subacromial impingement, restricted range of motion, and early-onset secondary osteoarthritis. Therefore, anatomical restoration is not merely an aesthetic radiographic goal; it is a strict biomechanical necessity.
The Evolution of Surgical Management
Historically, 50% to 80% of proximal humerus fractures were deemed non-displaced or minimally displaced and managed non-operatively, relying on brief periods of sling immobilization followed by aggressive, early range of motion protocols. While conservative management remains the gold standard for truly stable, non-displaced patterns, the remaining 20% to 50% of fractures present with displacement that necessitates operative intervention to prevent catastrophic functional loss.
The surgical paradigm has shifted dramatically over the past two decades. While laterally based locking plates revolutionized the treatment of these injuries, they brought their own unique set of complications, including varus collapse, screw penetration into the joint space, and significant soft tissue stripping leading to avascular necrosis. Intramedullary nailing has experienced a massive resurgence, driven by advanced, anatomically contoured nail designs and multi-planar locking screw trajectories. By acting as a load-sharing device positioned directly along the mechanical axis of the humerus, the modern intramedullary nail provides superior biomechanical stability in osteoporotic bone while minimizing soft tissue disruption.
Detailed Surgical Anatomy and Biomechanics
Osteology and Morphologic Relationships
Before we make our initial incision, a profound understanding of the complex three-dimensional osteology of the proximal humerus is mandatory. The proximal humerus comprises four distinct anatomical segments: the humeral head (articular surface), the greater tuberosity, the lesser tuberosity, and the proximal humeral shaft (diaphysis). The transition zone between these segments—the surgical neck—is the most frequent site of mechanical failure.
The geometry of the humeral head is highly specific and must be respected during reconstruction. The articular surface is oriented slightly higher than the apices of the tuberosities. Crucially, the center of the humeral head is offset approximately 3 mm medially and 7 mm posteriorly in relation to the central axis of the humeral diaphysis. Furthermore, the humeral head is retroverted approximately 30 degrees (with a normal physiological range spanning 20 to 60 degrees) relative to the epicondylar axis of the distal humerus.

Failure to recognize and restore this specific retroversion and medial/posterior offset during intramedullary nailing will inevitably lead to altered glenohumeral kinematics, severe subacromial impingement, and restricted internal or external rotation. The entry point for the nail must perfectly account for this offset to avoid iatrogenic malalignment of the fracture fragments during nail insertion.
Vascular Supply and the Risk of Ischemia
The vascular supply to the proximal humerus is notoriously precarious, and its disruption is the primary catalyst for avascular necrosis (AVN). Historically, the anterior humeral circumflex artery (AHCA) and its ascending branch, the arcuate artery, were considered the dominant blood supply to the humeral head. The arcuate artery enters the bone at the bicipital groove and perfuses the vast majority of the articular segment. Disruption of this vessel, particularly in anatomical neck fractures, was thought to almost guarantee ischemia.
However, contemporary microvascular studies have revolutionized our understanding, demonstrating that the posterior humeral circumflex artery (PHCA) provides a massive, and often dominant, contribution to the perfusion of the humeral head via rich intraosseous anastomoses. This paradigm shift is critical for the operating surgeon. If the anterior circulation is compromised by the initial trauma, the posterior circumflex artery becomes the sole lifeline for the fractured head.

Therefore, meticulous, gentle soft tissue handling—particularly avoiding aggressive posterior dissection or excessive traction—is paramount to prevent iatrogenic devascularization. The minimally invasive nature of intramedullary nailing is specifically designed to respect this delicate vascular envelope, preserving the critical medial hinge and the soft tissue attachments that harbor these life-saving vessels.
Neuromuscular Anatomy and Deforming Forces
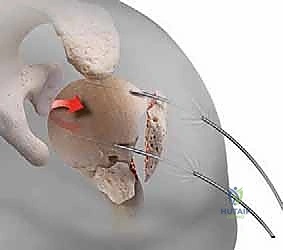
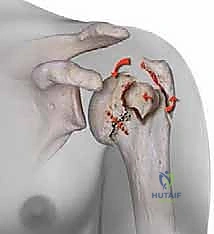
Understanding the specific muscular forces acting upon the fracture fragments is the absolute key to achieving and maintaining an anatomical reduction. The proximal humerus is subjected to massive, multi-directional deforming forces. The greater tuberosity serves as the insertion site for the supraspinatus, infraspinatus, and teres minor. When fractured, these powerful tendons pull the greater tuberosity fragment superiorly and posteriorly.
Conversely, the lesser tuberosity is the sole insertion site for the subscapularis tendon. When isolated, the subscapularis will forcefully internally rotate and medially displace the lesser tuberosity fragment. Meanwhile, the humeral shaft is subjected to the proximal pull of the deltoid and the medializing force of the pectoralis major. The humeral head, devoid of tendinous attachments, will passively follow whichever tuberosity remains in continuity with it, leading to classic valgus-impacted or varus-angulated deformities.

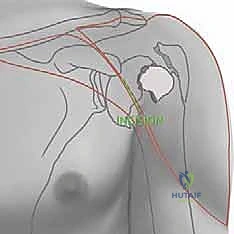
Neurologically, the axillary nerve is of paramount concern. Coursing through the quadrilateral space, it wraps anteriorly around the surgical neck of the humerus, typically lying 4 to 7 centimeters distal to the lateral edge of the acromion. During intramedullary nailing, the lateral percutaneous entry sites for the proximal locking screws place the axillary nerve at direct, significant risk. A meticulous, blunt dissection technique down to the bone, utilizing protective drill sleeves, is an absolute, non-negotiable requirement to prevent catastrophic denervation of the deltoid.
Exhaustive Indications and Contraindications
Patient Selection and Operative Indications
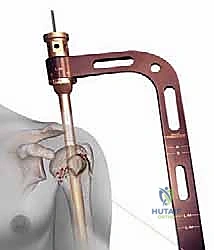
The decision to proceed with intramedullary nailing requires a nuanced understanding of fracture morphology, bone quality, and patient physiology. The ideal indication for this technique is the unstable, displaced two-part surgical neck fracture. In these patterns, the nail acts as an internal splint, providing rigid, load-sharing stability that far surpasses laterally based plates, particularly in osteoporotic bone where the risk of varus collapse is exceptionally high.
Three-part proximal humerus fractures also represent a strong indication for nailing, provided the surgeon possesses the advanced technical skill required to meticulously reduce and secure the displaced tuberosity fragment. Modern nail designs feature specific proximal suture holes, allowing the surgeon to pass heavy, non-absorbable sutures through the rotator cuff tendon-bone interface and tie them directly to the nail or the humeral shaft, neutralizing the deforming forces and integrating the tuberosity into the construct.
Select four-part fractures can be managed with intramedullary nailing, but this is reserved strictly for younger, high-demand patients where preservation of the native humeral head is paramount. Specifically, classic "valgus-impacted" four-part fractures, where the medial periosteal hinge remains intact, carry a significantly lower risk of avascular necrosis and are highly amenable to joint-preserving intramedullary fixation.
Absolute and Relative Contraindications
Despite its advantages, intramedullary nailing is not a panacea, and recognizing its contraindications is critical to avoiding catastrophic failures. Absolute contraindications include true "head-splitting" fractures, where the articular surface is severely comminuted and structurally destroyed. In these scenarios, anatomical reconstruction is impossible, and primary prosthetic arthroplasty (hemiarthroplasty or reverse total shoulder arthroplasty) is the only viable definitive treatment.
Severe comminution of the surgical neck combined with gross displacement of the humeral head, particularly when the medial calcar hinge is completely disrupted (calcar length < 8mm), represents a massive risk for avascular necrosis. If the humeral head fragment is entirely devoid of soft tissue attachments, it is effectively a dead piece of bone. Attempting internal fixation in this setting will almost certainly result in AVN, hardware cutout, and early failure.
Relative contraindications include active systemic or local infection, which precludes the implantation of any hardware. Additionally, patients with pre-existing, severe rotator cuff arthropathy or advanced glenohumeral osteoarthritis are poor candidates for internal fixation, as preserving a degenerated, painful joint serves no clinical benefit. In such older patients with complex fractures and poor baseline joint function, a primary reverse total shoulder arthroplasty provides superior, predictable pain relief and functional restoration.
Quick Reference: Indications and Contraindications
| Category | Specific Conditions | Rationale / Notes |
|---|---|---|
| Primary Indications | Displaced 2-part surgical neck fractures | Ideal load-sharing biomechanics, prevents varus collapse. |
| 3-part fractures (GT or LT involvement) | Requires meticulous suture fixation of tuberosities to the nail. | |
| Valgus-impacted 4-part fractures | Medial hinge often intact, lower AVN risk, joint preservation possible. | |
| Pathologic/Impending fractures | Allows prophylactic stabilization of the entire diaphysis. | |
| Absolute Contraindications | Head-splitting articular fractures | Joint surface destroyed; requires primary arthroplasty. |
| Gross devascularization (Hertel criteria) | Calcar <8mm, disrupted medial hinge = >90% AVN risk. Arthroplasty preferred. | |
| Active local or systemic infection | High risk of deep implant infection and osteomyelitis. | |
| Relative Contraindications | Pre-existing cuff arthropathy / severe OA | Fixing a broken, arthritic joint yields poor outcomes. Favor RTSA. |
| Extreme physiological frailty | Unable to comply with postoperative rehabilitation protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Templating Strategies
Flawless execution in the operating room begins days before the incision, rooted in exhaustive preoperative planning. The standard radiographic trauma series—a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view—is mandatory. However, plain radiographs frequently underestimate the degree of comminution and tuberosity displacement.
Therefore, a fine-cut Computed Tomography (CT) scan with three-dimensional (3D) reconstructions is considered the standard of care for all complex three- and four-part fractures. The CT scan allows the surgeon to precisely map the fracture lines, assess the volume and integrity of the humeral head, map the exact location of the tuberosity fragments, and evaluate the bone stock available for screw purchase. This 3D spatial awareness is critical for formulating a step-by-step reduction strategy.
Digital templating is a critical, yet often overlooked, step. Using calibrated radiographs of the contralateral, uninjured shoulder, the surgeon must template the anticipated nail diameter, overall implant length, and the precise trajectory of the proximal interlocking screws. This ensures that the appropriate inventory is available in the suite and prevents intraoperative delays. Specifically, the surgeon must anticipate the need for "calcar screws"—inferomedially directed locking screws that provide crucial structural support to the medial column and prevent postoperative varus collapse.
Operating Room Setup and Patient Positioning
Patient positioning is arguably the most critical step in the entire procedure; a poor setup will doom the operation before it begins. The patient is placed supine on a fully radiolucent operating table and transitioned into the "beach chair" position, with the backrest elevated to precisely 60 to 70 degrees. This upright orientation utilizes gravity to assist in reducing the humeral shaft relative to the head.

Crucially, a firm bolster or folded blanket must be placed under the medial border of the ipsilateral scapula. This elevates the shoulder girdle away from the table, allowing for unrestricted extension of the arm. If the arm cannot be fully extended, the acromion will block access to the optimal entry point on the apex of the humeral head, forcing an errant, anteriorly translated starting hole that will inevitably lead to malreduction and anterior hardware cutout.
The C-arm fluoroscopy unit is positioned on the contralateral side of the patient, entering parallel to the head of the bed. The monitor must be positioned directly in the surgeon's line of sight. Before prepping and draping, a "dry run" with the C-arm is mandatory. The radiology technician must demonstrate the ability to obtain perfect, unobstructed AP and true axillary lateral views of the proximal humerus simply by rotating the C-arm, without requiring the surgeon to move the fractured, unstable arm.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Soft Tissue Management, and the Entry Point
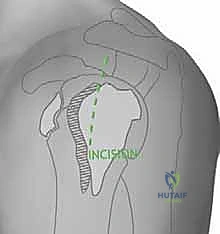
With the patient perfectly positioned and prepped, we begin our minimally invasive approach. A 3 to 5-centimeter anterolateral incision is made extending distally from the anterior edge of the acromion. We bluntly split the anterior and middle thirds of the deltoid muscle, strictly respecting the raphe to minimize bleeding. A self-retaining retractor is placed, taking extreme care not to plunge distally, which would jeopardize the axillary nerve crossing the operative field just a few centimeters below.
The subdeltoid bursa is excised to expose the underlying rotator cuff. We identify the supraspinatus tendon and make a longitudinal, 2-centimeter split directly in line with its fibers, precisely at the musculotendinous junction. This split exposes the articular cartilage of the superior humeral head. Heavy, non-absorbable traction sutures (e.g., #2 FiberWire) are immediately passed through the anterior and posterior leaflets of the supraspinatus and the attached greater tuberosity. These sutures serve as vital "joysticks" to manipulate the proximal fragments without grasping them with crushing instruments.
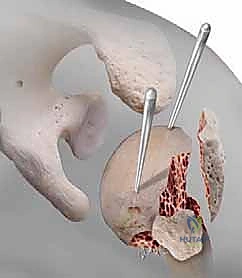
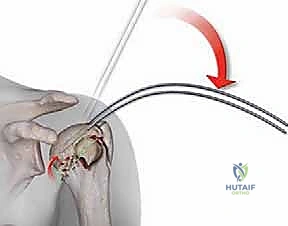
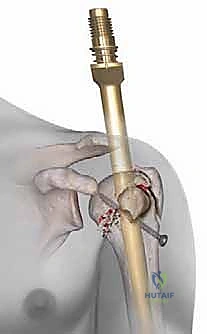
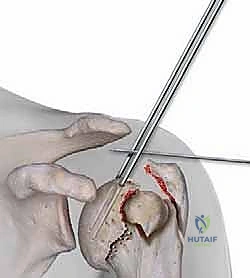
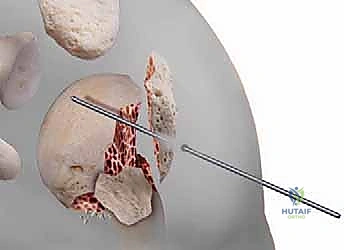
Establishing the correct entry point is the most critical technical step of the operation. The starting guidewire must be placed at the absolute apex of the humeral head, slightly medial to the footprint of the greater tuberosity, and perfectly aligned with the central axis of the medullary canal in both the AP and lateral planes. If the entry point is too lateral (on the tuberosity itself), nail insertion will wedge the fracture into varus. If it is too anterior, the nail will cut out through the bicipital groove. We confirm this entry point exhaustively with orthogonal fluoroscopy before opening the cortex with a cannulated awl or reamer.
Fracture Reduction and Canal Preparation
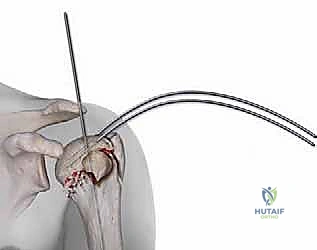
Once the entry portal is established, attention turns to fracture reduction. For two-part surgical neck fractures, longitudinal traction combined with gentle flexion and abduction of the arm is often sufficient to align the shaft with the head. For more complex patterns, we utilize the previously placed rotator cuff sutures to pull the tuberosities into anatomical position. If a fragment is particularly recalcitrant, a smooth 2.0mm Kirschner wire can be used percutaneously as a joystick to lever the fragment into place.

With provisional reduction achieved, a ball-tipped guide wire is passed
Clinical & Radiographic Imaging Archive