Mastering O.R.I.F. for Displaced Proximal Humeral Fractures

Key Takeaway
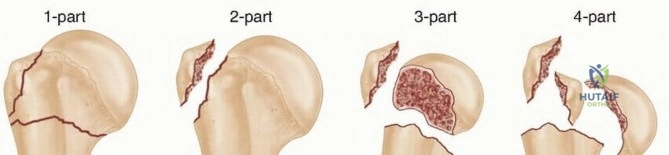
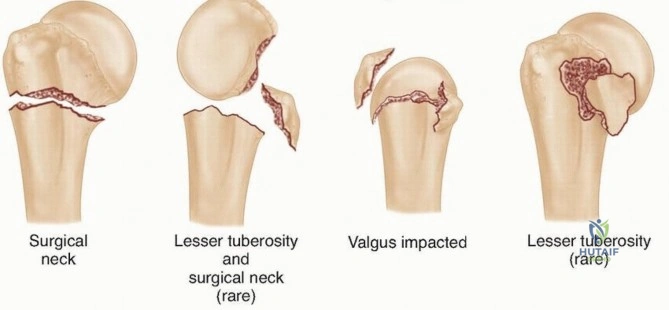
Discover the latest medical recommendations for Mastering O.R.I.F. for Displaced Proximal Humeral Fractures. Displaced proximal humeral fractures involve the surgical neck, greater tuberosity, or lesser tuberosity, where fragments are displaced by 1 cm or angulated 45 degrees. The Neer classification categorizes these based on the number of displaced segments, including the articular surface and humeral shaft, guiding treatment decisions for patients.
Comprehensive Introduction and Patho-Epidemiology
Proximal humerus fractures represent one of the most common fragility fractures encountered by orthopedic surgeons, accounting for approximately 5% to 6% of all adult fractures and ranking as the third most common fracture in patients over the age of 65. The epidemiology of these injuries demonstrates a classic bimodal distribution. In the elderly population, these fractures typically result from low-energy mechanisms, such as a fall from a standing height, and are intimately associated with underlying osteopenia or osteoporosis. Conversely, in younger cohorts, proximal humerus fractures are generally the result of high-energy trauma, such as motor vehicle collisions, falls from significant heights, or extreme sports injuries. In these high-energy scenarios, the orthopedic surgeon must maintain a high index of suspicion for concomitant injuries, including glenohumeral dislocations, scapulothoracic dissociation, and neurovascular compromise.
The classification of proximal humerus fractures is paramount for both prognosticating outcomes and guiding surgical decision-making. The Neer classification system remains the most universally recognized and utilized framework. Neer conceptualized the proximal humerus as four distinct anatomic segments: the articular surface (humeral head), the greater tuberosity, the lesser tuberosity, and the humeral shaft. Crucially, a segment is only considered a "part" if it is displaced by more than 1 centimeter or angulated by more than 45 degrees relative to its native anatomical position. This distinction is critical; a fracture may have multiple distinct fracture lines, but if the fragments remain undisplaced according to these strict criteria, it is clinically treated as a one-part fracture. Despite its widespread use, multiple studies have demonstrated that the interobserver and intraobserver reliability of the Neer classification is notoriously low, highlighting the inherent complexity of these fracture patterns.
In contrast, the AO/ASIF (Arbeitsgemeinschaft für Osteosynthesefragen) classification system provides a more comprehensive, albeit complex, morphological categorization. It broadly divides proximal humerus fractures into three overarching types: Type A (unifocal extra-articular), Type B (bifocal extra-articular), and Type C (intra-articular). Each type is subsequently subdivided into groups and subgroups based on the specific fracture geometry and degree of comminution. The AO/ASIF system places a profound emphasis on the vascular supply to the humeral head. Intra-articular fracture patterns (Type C), particularly those with anatomical neck involvement, are recognized as having the highest risk of post-traumatic avascular necrosis (AVN). While comprehensive, the AO/ASIF system suffers from similar reliability issues as the Neer classification when applied in standard clinical practice without the aid of advanced three-dimensional imaging.
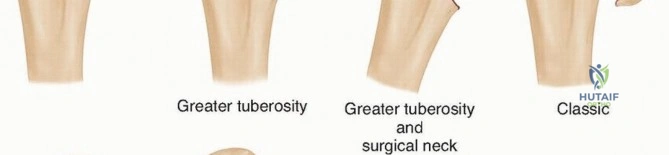
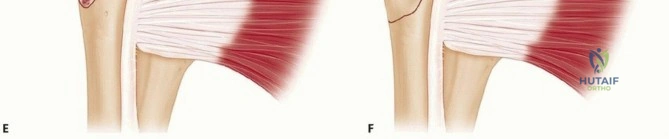
A unique and clinically significant entity that warrants special attention is the valgus impacted four-part fracture. Although not explicitly detailed in Neer's original classification framework, this pattern is critical to recognize due to its distinct pathoanatomy and favorable prognosis. In a valgus impacted fracture, the humeral articular surface is driven down and impacted into the metaphyseal bone of the humeral shaft in a valgus alignment. This impaction increases the angle between the humeral shaft and the articular surface. Because the medial periosteal hinge often remains intact and the rotator cuff attachments frequently prevent severe lateral displacement of the tuberosities, the critical blood supply to the humeral head is often preserved. Consequently, these fractures have a demonstrably lower incidence of avascular necrosis compared to classic displaced four-part fractures, making them highly amenable to joint-preserving open reduction and internal fixation (ORIF) rather than primary arthroplasty.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the osseous and soft tissue anatomy of the proximal humerus is the absolute foundation of successful surgical management. The proximal humerus consists of the articular surface of the humeral head, the greater tuberosity, and the lesser tuberosity, which transition distally into the surgical neck and humeral shaft. The bicipital groove (intertubercular sulcus) lies between the greater and lesser tuberosities, housing the long head of the biceps tendon, which serves as a critical surgical landmark for identifying the interval between the tuberosities and guiding the placement of osteosynthesis plates. The anatomical neck demarcates the articular cartilage from the metaphyseal bone, and fractures through this region carry a grave prognosis for the viability of the humeral head.
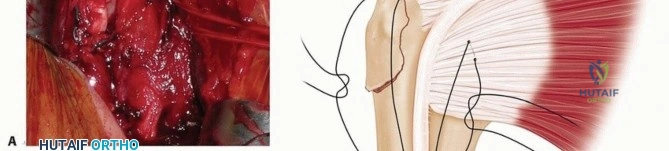
The deforming forces acting upon the proximal humerus dictates the characteristic displacement patterns seen in these fractures. The muscular attachments act predictably on the isolated fracture fragments. The pectoralis major, inserting on the lateral lip of the bicipital groove, acts as a powerful deforming force on the humeral shaft, pulling it anteromedially. The rotator cuff musculature exerts force on the tuberosities. The supraspinatus, infraspinatus, and teres minor insert onto the superior, middle, and inferior facets of the greater tuberosity, respectively. In a two-part greater tuberosity fracture, these tendons pull the fragment superiorly and posteriorly. The subscapularis inserts onto the lesser tuberosity; in isolation, it pulls the lesser tuberosity medially. In a three-part fracture involving the surgical neck and greater tuberosity, the unopposed pull of the subscapularis on the intact lesser tuberosity internally rotates the articular segment. Conversely, if the lesser tuberosity is fractured (three-part lesser tuberosity fracture), the intact greater tuberosity attachments externally rotate the head segment, causing the articular surface to face anteriorly.

The vascular anatomy of the proximal humerus has been the subject of extensive anatomical study and paradigm shifts. Historically, based on the classic dye injection studies by Laing and later Gerber, the anterolateral ascending (arcuate) branch of the anterior circumflex humeral artery was considered the primary blood supply to the humeral head. This branch ascends lateral to the bicipital groove and enters the head at the junction of the greater tuberosity and the articular surface. However, contemporary quantitative perfusion studies, particularly those by Hettrich et al., have revolutionized our understanding. It is now established that the posterior circumflex humeral artery (PCHA) provides the predominant blood supply (up to 64%) to the humeral head, specifically perfusing the superior, inferior, and lateral aspects. The PCHA branches from the axillary artery, travels posteriorly through the quadrangular space alongside the axillary nerve, and arborizes extensively over the posterior aspect of the proximal humerus.
The relationship between fracture morphology and this vascular network is the primary determinant of post-traumatic avascular necrosis. Hertel's seminal work identified specific radiographic predictors of ischemia. Fractures that disrupt the medial hinge—specifically, those with a metaphyseal head extension (calcar length) of less than 8 mm and disruption of the medial periosteum—carry a critically high risk of AVN. The integrity of the medial calcar is not only vital for vascular preservation but also for the biomechanical stability of the construct. Without medial cortical contact, the construct is subjected to massive bending moments, leading to varus cantilever bending, screw cutout, and catastrophic failure of the internal fixation. Therefore, anatomical reduction of the medial cortex and restoration of the calcar are non-negotiable goals during ORIF.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative versus nonoperative management of proximal humerus fractures is nuanced and must be highly individualized. Historically, conservative management was the gold standard for the vast majority of these fractures, particularly those that were minimally displaced. However, the advent of pre-contoured, periarticular locking plate technology has significantly expanded the indications for surgical intervention, allowing for stable fixation even in osteoporotic bone. Despite these advancements, nonoperative management remains the treatment of choice for truly undisplaced fractures, stable impacted fractures, and in patients whose medical comorbidities preclude safe administration of anesthesia.
Operative intervention is strongly indicated for displaced two-part, three-part, and select four-part fractures where the physiological age and functional demands of the patient justify the surgical risks. Isolated greater tuberosity fractures represent a unique subset with very low tolerance for displacement. McLaughlin originally posited that displacement greater than 5 mm results in significant subacromial impingement, altered rotator cuff kinematics, and profound functional deficits. Therefore, surgical fixation is routinely indicated for greater tuberosity fractures displaced more than 5 mm, and in high-performance athletes, even 3 mm of superior displacement may warrant intervention. Furthermore, any fracture associated with a glenohumeral dislocation that cannot be concentrically reduced, or fractures with associated vascular injuries, represent absolute indications for urgent surgical exploration and stabilization.
Contraindications to ORIF must be carefully weighed to avoid devastating surgical failures. Absolute contraindications include active local or systemic infection, severe medical comorbidities rendering the patient unfit for surgery, and non-ambulatory patients with minimal pain who have no functional use of the extremity. Relative contraindications include profound osteoporosis where screw purchase is deemed impossible, severe pre-existing glenohumeral osteoarthritis, and massive, irreparable rotator cuff arthropathy. In older patients with complex four-part fractures, particularly head-split variants or those with a disrupted medial hinge and high AVN risk, primary hemiarthroplasty or reverse total shoulder arthroplasty (RTSA) may be more appropriate than ORIF, as these arthroplasty options provide more predictable pain relief and functional restoration without the risk of nonunion or AVN.
Indications and Contraindications for ORIF
| Parameter | Indications for O.R.I.F. | Contraindications / Alternative Tx |
|---|---|---|
| Displacement | >1 cm displacement or >45° angulation | Minimally displaced (<1 cm, <45°) |
| Tuberosity | Greater tuberosity >5 mm displaced | Undisplaced tuberosity fractures |
| Fracture Type | Displaced 2-part, 3-part, valgus impacted 4-part | Head-split fractures, severe comminution (Favor Arthroplasty) |
| Patient Profile | Physiologically young, high functional demand | Severe dementia, non-ambulatory, extreme medical risk |
| Bone Quality | Adequate bone stock for screw purchase | Profound osteoporosis (Favor RTSA) |
| Associated Injury | Open fractures, vascular compromise, irreducible dislocation | Active local infection (Absolute Contraindication) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful ORIF for proximal humerus fractures. The clinical evaluation must begin with a comprehensive history, elucidating the mechanism of injury, the patient's hand dominance, occupation, and baseline functional status. A thorough neurovascular examination is mandatory. The axillary nerve is particularly vulnerable, with studies indicating injury rates approaching 40% in patients under 50 years of age who sustain surgical neck fractures or fracture-dislocations. Vascular injuries, while rare, are limb-threatening; a high index of suspicion must be maintained for fractures exhibiting severe medial displacement of the humeral shaft, which can tether and injure the axillary artery. Diminished radial or ulnar pulses require immediate vascular consultation and advanced imaging.
Standard radiographic evaluation consists of a complete trauma series of the shoulder: a true anteroposterior (Grashey) view, a scapular Y view, and an axillary view. The axillary view is non-negotiable, as it is the only reliable plain radiograph to assess glenohumeral concentricity and the anteroposterior relationship of the tuberosities. If plain radiographs are insufficient to delineate the fracture morphology, a non-contrast Computed Tomography (CT) scan with 3D reconstructions is highly recommended. While CT scanning may only minimally improve interobserver reliability of classification systems, it is invaluable for surgical planning. It allows the surgeon to accurately assess articular surface involvement, the degree of tuberosity comminution, and the presence of associated injuries such as bony Bankart or Hill-Sachs lesions. Magnetic Resonance Imaging (MRI) is rarely indicated in the acute trauma setting unless there is a high suspicion of a concomitant massive rotator cuff tear that would alter the surgical plan.
Pre-operative templating utilizing digital software is critical for anticipating implant size, optimal plate positioning, and required screw lengths. The surgeon must evaluate the integrity of the medial calcar on the templating software to determine if structural allograft augmentation (such as a fibular strut) will be necessary to prevent varus collapse. Once the plan is established, patient positioning in the operating room must be executed flawlessly. The beach-chair position is universally preferred for proximal humerus ORIF. The patient is positioned with the hips and knees flexed, and the backrest elevated to approximately 45 to 60 degrees. The patient is lateralized on the table so that the operative shoulder extends completely off the edge, allowing for unobstructed extension and rotation of the arm.

Fluoroscopic positioning is just as critical as patient positioning. The C-arm image intensifier should be brought in from the contralateral side or positioned posterior to the patient's head, parallel to the floor. Before the patient is prepped and draped, the surgeon must obtain orthogonal fluoroscopic views (AP and axillary) to ensure that the entire proximal humerus, including the humeral head and the diaphysis, can be visualized without interference from the table or radiopaque positioning devices. A sterile Mayo stand or a specialized arm positioner (e.g., Spider arm) is utilized to control the extremity during the procedure, allowing the surgeon to manipulate the arm to aid in fracture reduction.

Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the proximal humerus is dictated by the fracture pattern and the surgeon's familiarity. The deltopectoral approach is the workhorse for proximal humerus ORIF, offering excellent extensile exposure and utilizing a true internervous plane between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves). The incision begins at the tip of the coracoid process and extends distally and laterally toward the deltoid tuberosity. The cephalic vein is identified and typically retracted laterally with the deltoid to preserve its venous drainage, although medial retraction is acceptable if the vein is intimately adherent to the pectoralis. The clavipectoral fascia is incised, and the conjoined tendon is retracted medially. The subdeltoid and subacromial spaces are bluntly developed to mobilize the proximal humerus.
Alternatively, a deltoid-splitting (anterolateral) approach can be utilized, particularly for isolated greater tuberosity fractures or valgus impacted patterns where extensive medial exposure is unnecessary. The incision extends distally from the anterolateral tip of the acromion. The deltoid is split precisely in line with its fibers. The critical limitation of this approach is the axillary nerve, which traverses the deep surface of the deltoid approximately 5 to 7 cm distal to the acromion. To prevent catastrophic denervation of the anterior deltoid, the split must never extend beyond 5 cm, and a stay suture is routinely placed at the distal apex of the split to prevent inadvertent distal propagation during retraction.

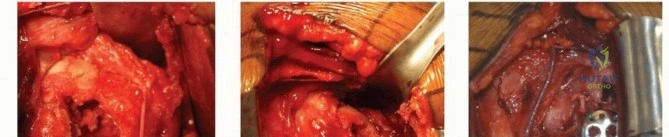
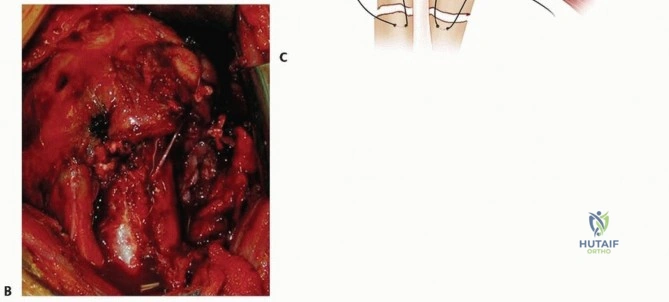
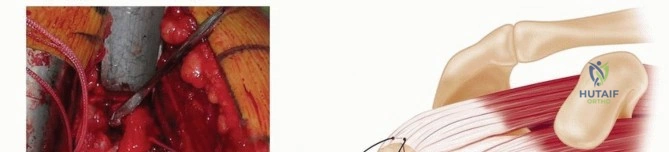
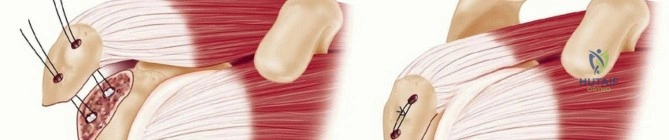
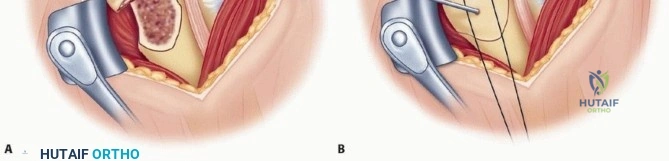
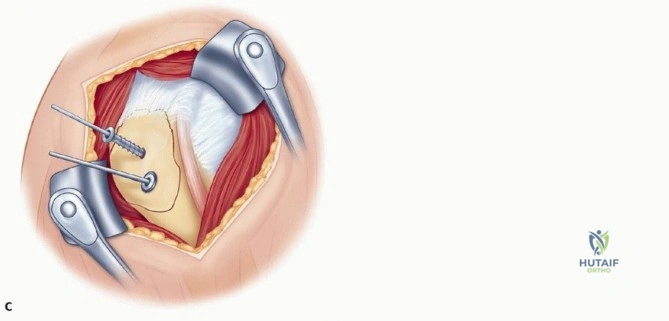
Once the fracture is exposed, the initial step is the evacuation of the fracture hematoma to allow visualization of the fracture lines. In complex multi-part fractures, heavy non-absorbable traction sutures (e.g., #2 or #5 FiberWire) are placed through the tendon-bone interface of the supraspinatus, infraspinatus, and subscapularis. These traction sutures are indispensable; they serve as "joysticks" to control the tuberosity fragments, neutralize the deforming forces of the rotator cuff, and facilitate anatomical reduction without crushing the osteoporotic bone with traditional reduction forceps.
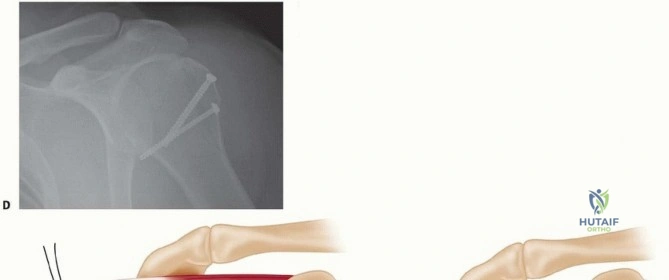
For isolated greater tuberosity fractures, once anatomical reduction is achieved via the traction sutures and arm positioning (abduction and external rotation), provisional fixation is obtained with smooth Kirschner wires. Definitive fixation can then be achieved using multiple techniques depending on fragment size and bone quality. Large, robust fragments may be secured with 4.5-mm or 3.5-mm partially threaded cannulated screws equipped with washers to maximize compression. However, in osteoporotic bone or highly comminuted fragments, screw fixation often fails. In these scenarios, a heavy suture construct (suture cerclage or double-row equivalent techniques) utilizing the previously placed traction sutures passed through drill holes in the intact humeral shaft provides superior biomechanical fixation.
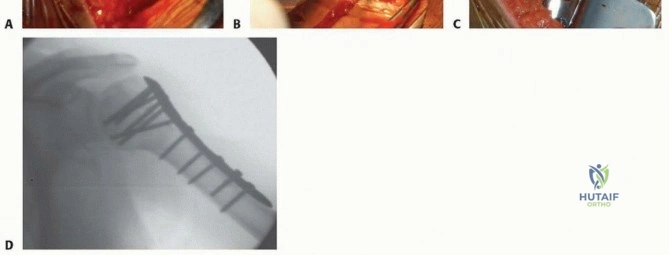
For fractures requiring a locking plate, the articular segment is first reduced to the humeral shaft. If the medial hinge is comminuted, an intramedullary fibular strut allograft may be inserted into the shaft and impacted into the humeral head to provide a biological and
Clinical & Radiographic Imaging Archive