Proximal Humerus Fractures: An Intraoperative Masterclass in OR/IF

Key Takeaway
This masterclass provides an exhaustive, real-time guide to open reduction and internal fixation of proximal humerus fractures. We delve into comprehensive surgical anatomy, meticulous preoperative planning, and precise intraoperative execution. Fellows will learn step-by-step techniques, critical pearls to avoid pitfalls, and strategies for managing complex scenarios, ensuring optimal patient outcomes through detailed surgical directives and post-operative care.
Comprehensive Introduction and Patho-Epidemiology
Proximal humerus fractures represent a significant and expanding challenge within the realm of orthopedic trauma, accounting for approximately 5% to 6% of all adult fractures. As the global population continues to age, the incidence of these injuries is rising exponentially, presenting a bimodal epidemiological distribution. In younger demographics, these fractures are typically the result of high-energy trauma, such as motor vehicle collisions or falls from significant heights, often presenting with severe comminution, soft tissue compromise, and concomitant injuries. Conversely, the vast majority of proximal humerus fractures occur in elderly patients following low-energy mechanisms, primarily ground-level falls, where compromised bone mineral density (osteoporosis) plays a definitive role in the fracture pattern and subsequent fixation challenges.
The overarching philosophy in managing proximal humerus fractures has evolved dramatically over the past two decades. Historically, conservative management was the mainstay of treatment, accepting a degree of malunion in exchange for avoiding the high complication rates associated with early generation internal fixation devices. However, the advent of locking plate technology has fundamentally shifted the treatment paradigm. The modern orthopedic surgeon is no longer merely attempting to "put bone back together"; the objective is the meticulous restoration of intricate shoulder mechanics, the strict preservation of the delicate vascular supply to the humeral head, and the establishment of a biomechanically stable construct that permits early, aggressive rehabilitation.
Achieving these goals requires a profound understanding of the unique pathoanatomy of the shoulder girdle. The proximal humerus is a complex, multi-planar osseous structure suspended by a highly dynamic muscular envelope. When a fracture occurs, the harmonious balance of the rotator cuff is disrupted, leading to predictable, yet formidable, deforming forces. Furthermore, the tenuous blood supply to the articular segment places the patient at a significant risk for avascular necrosis (AVN), a devastating complication that can compromise even the most perfectly executed osteosynthesis.
Therefore, mastering the open reduction and internal fixation (ORIF) of proximal humerus fractures demands more than just technical proficiency with a drill and a plate. It requires a comprehensive, masterclass-level approach encompassing rigorous preoperative templating, a nuanced understanding of internervous surgical planes, meticulous soft-tissue handling, and the strategic deployment of biomechanical fixation principles. This chapter will exhaustively detail this approach, providing the orthopedic surgeon with the cognitive and technical armamentarium required to transform complex proximal humerus trauma into excellent, long-lasting functional outcomes.
Detailed Surgical Anatomy and Biomechanics
Osseous Anatomy and Classification Systems
Before any surgical intervention is contemplated, an exhaustive comprehension of the fracture morphology and the underlying osseous anatomy is paramount. The proximal humerus is anatomically divided into four distinct segments: the articular surface (humeral head), the greater tuberosity, the lesser tuberosity, and the humeral diaphysis (shaft). The spatial relationship between these segments dictates both the classification of the injury and the surgical strategy required for reconstruction. The bicipital groove, housing the long head of the biceps tendon, serves as a critical anatomical landmark separating the greater and lesser tuberosities, and acts as a constant reference point during surgical exploration.
We primarily rely on the Neer classification system, a foundational framework that categorizes fractures based on the number of displaced "parts." Neer astutely defined a fragment as "displaced" only if it has translated by 1 centimeter or more, or if it is angulated by 45 degrees or more relative to its anatomical position. Therefore, a fracture line may exist, but if it does not meet these criteria, it remains a "one-part" fracture. The classification progresses from two-part fractures (typically surgical neck or isolated greater tuberosity) to highly complex three-part and four-part fractures, which involve significant displacement of the tuberosities and the humeral shaft relative to the articular segment.

While not explicitly detailed in Neer's original manuscript, the valgus impacted fracture pattern is a distinct clinical entity that demands specific recognition. In these injuries, the humeral diaphysis is driven into the humeral head, forcing it into a valgus alignment. Crucially, the medial periosteal hinge often remains intact, and the tuberosities, while fractured, are frequently held in relative position by the intact rotator cuff. This unique configuration preserves a significant portion of the blood supply, resulting in a substantially lower rate of avascular necrosis compared to standard four-part fractures, thereby influencing the decision toward joint-preserving fixation rather than arthroplasty.
The AO/ASIF classification system provides an alternative, highly detailed morphological categorization. It divides proximal humerus fractures into Type A (unifocal, extra-articular), Type B (bifocal, extra-articular), and Type C (intra-articular). This system places a strong emphasis on the integrity of the vascular supply, recognizing that Type C anatomical neck fractures carry the highest inherent risk of ischemia. While both the Neer and AO systems are indispensable for academic communication and research, it is well-documented that interobserver reliability can be suboptimal. Therefore, the surgeon must synthesize the classification with advanced three-dimensional imaging to formulate a definitive preoperative plan.
Muscular Deforming Forces
The osseous anatomy provides the scaffolding, but it is the muscular attachments that dictate the displacement patterns of proximal humerus fractures. The shoulder is a highly mobile joint governed by powerful muscular forces that act as dynamic tethers. When osseous continuity is disrupted, these muscles contract unopposed, resulting in classic, predictable deformities that the surgeon must actively overcome during reduction. Understanding these vectors is the key to successful intraoperative manipulation and provisional fixation.
The subscapularis muscle, innervated by the upper and lower subscapular nerves, inserts broadly onto the lesser tuberosity. Its primary function is internal rotation of the humerus. In the setting of a three-part fracture involving the greater tuberosity (where the greater tuberosity is detached), the intact subscapularis exerts an unopposed internal rotation force on the articular segment, causing the articular surface to rotate posteriorly and face the glenoid in a distorted manner. Conversely, if the lesser tuberosity is fractured and displaced, the subscapularis will pull the fragment medially.
The posterosuperior rotator cuff—comprising the supraspinatus, infraspinatus, and teres minor—inserts onto the superior and posterior facets of the greater tuberosity. These muscles act to abduct and externally rotate the shoulder. In a two-part greater tuberosity fracture, or a three-part fracture involving the lesser tuberosity, this muscle group pulls the greater tuberosity fragment superiorly and posteriorly. This superior migration is critical to recognize, as failure to anatomically reduce the greater tuberosity will inevitably lead to subacromial impingement and severe functional deficits.
Finally, the powerful pectoralis major muscle, inserting on the lateral lip of the bicipital groove, acts as a massive deforming force on the humeral shaft. In a standard two-part surgical neck fracture, the pectoralis major pulls the distal shaft fragment anteromedially. The surgeon will frequently encounter the proximal aspect of the humeral shaft buried deep within the deltopectoral interval, tethered medially by the pectoralis. Overcoming this anteromedial displacement requires strategic traction, leverage, and a deep understanding of the soft-tissue releases necessary to mobilize the diaphysis.
Vascular Anatomy and the Risk of Avascular Necrosis
The vascular anatomy of the proximal humerus is perhaps the most critical factor determining the long-term viability of the joint following trauma. The arterial supply is a delicate, intricate network that is highly susceptible to disruption from both the initial injury and subsequent surgical dissection. Historically, the anterolateral ascending branch of the anterior humeral circumflex artery (AHCA) was considered the primary blood supply to the humeral head. This vessel runs vertically, lateral to the bicipital groove, and penetrates the bone at the proximal extent of the groove to become the arcuate artery, supplying the majority of the epiphysis.
However, landmark anatomical and perfusion studies (such as those by Hettrich et al.) have fundamentally revised our understanding of this vascular network. It is now widely accepted that the posterior humeral circumflex artery (PHCA) provides the predominant blood supply to the humeral head, accounting for approximately 64% of the intraosseous vascularity. The PHCA enters the posterior aspect of the proximal humerus through multiple anastomotic vessels. This paradigm shift underscores the critical importance of preserving the posterior soft-tissue hinge and avoiding aggressive posterior dissection during surgical exposure.
The risk of avascular necrosis (AVN) is directly proportional to the degree of vascular disruption. Hertel's criteria provide invaluable radiographic predictors for ischemia. The most significant risk factors include a metaphyseal head extension (calcar length) of less than 8 millimeters, disruption of the medial periosteal hinge, and complex fracture patterns (anatomical neck fractures or four-part fractures). When these criteria are present, the surgeon must exercise extreme caution. Surgical approaches must be meticulously planned to avoid stripping the remaining soft-tissue attachments, particularly the inferior and posterior capsular vessels, to maximize the chances of head survival.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a proximal humerus fracture is rarely binary; it requires a complex calculus balancing the patient's physiological age, functional demands, bone quality, and the specific fracture morphology. While nonoperative management remains appropriate for minimally displaced fractures, the threshold for surgery has lowered with the advent of anatomically contoured locking plates. The primary objective of surgery is to prevent malunion, mitigate stiffness, and restore the biomechanical levers of the rotator cuff, which are frequently compromised in displaced fracture patterns.
Operative indications generally encompass fractures that meet or exceed Neer's criteria for displacement (>1 cm translation or >45 degrees angulation). Specifically, displaced two-part surgical neck fractures are prime candidates for ORIF, particularly when the shaft is translated significantly, as conservative management often leads to a varus malunion and subsequent impingement. Displaced greater tuberosity fractures are highly intolerant of conservative management; displacement greater than 5 millimeters (and in high-demand patients, even 3 millimeters) is a strong indication for surgery to prevent superior migration and subacromial impingement. Three-part and four-part fractures in physiologically active patients are almost universally treated operatively, either with ORIF or arthroplasty, depending on bone stock and head viability.
Contraindications to ORIF are equally important to recognize. Absolute contraindications include active, uncontrolled local or systemic infection, and patients who are medically unfit to tolerate general anesthesia or the physiological stress of surgery. Relative contraindications are highly nuanced. Severe dementia or an inability to comply with complex, multi-phased postoperative rehabilitation protocols strongly favors nonoperative management or a procedure with immediate stability, such as a reverse total shoulder arthroplasty (RTSA). Furthermore, in elderly patients with profound osteoporosis and highly comminuted four-part fractures where the risk of screw cut-out and AVN approaches 100%, primary RTSA is increasingly favored over attempting a doomed ORIF.
| Fracture Pattern / Clinical Scenario | Primary Management Strategy | Secondary / Alternative Strategy | Rationale / Considerations |
|---|---|---|---|
| Minimally Displaced (1-Part) | Nonoperative (Sling + Early ROM) | N/A | High success rate; early pendulum exercises prevent adhesive capsulitis. |
| Displaced 2-Part Surgical Neck | ORIF with Locking Plate | Intramedullary Nail (Select cases) | Restores medial calcar support; prevents varus malunion. |
| Displaced Greater Tuberosity (>5mm) | ORIF (Suture fixation or Plate) | Arthroscopic reduction (rare) | Prevents subacromial impingement and restores abduction power. |
| 3-Part Fracture (Young/Active) | ORIF with Locking Plate + Suture | N/A | Preservation of native joint is paramount; aggressive rotator cuff tagging required. |
| 4-Part Fracture (Young/Active) | ORIF (Joint Preserving) | Hemiarthroplasty / RTSA (if AVN high) | Attempt osteosynthesis if medial hinge/calcar >8mm is intact. |
| 4-Part Fracture (Elderly/Osteoporotic) | Reverse Total Shoulder Arthroplasty | Hemiarthroplasty | High risk of AVN and hardware failure with ORIF; RTSA provides reliable function. |
| Head-Splitting Fracture | Arthroplasty (Hemi or RTSA) | ORIF (Extremely rare, young only) | Articular incongruity guarantees rapid post-traumatic arthrosis. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Advanced Imaging
The foundation of a successful surgical outcome is laid long before the patient enters the operating theater. A meticulous preoperative assessment begins with a comprehensive history and physical examination. In the trauma bay, the orthopedic surgeon must look beyond the obvious deformity. A rigorous neurovascular examination is absolutely critical and must be documented meticulously. The axillary nerve is particularly vulnerable as it courses through the quadrilateral space and wraps around the surgical neck. Axillary nerve palsy is present in up to 40% of displaced proximal humerus fractures and dislocations. The surgeon must assess sensation over the lateral deltoid and, if pain permits, isometric deltoid contraction. Furthermore, the radial, median, and ulnar nerves, as well as distal pulses, must be evaluated to rule out catastrophic brachial plexus or axillary artery injuries.
Standard radiographic evaluation requires a dedicated trauma series of the shoulder: a true anteroposterior (Grashey) view, a Scapular Y (lateral) view, and an axillary view. The axillary view is non-negotiable, as it is the only reliable method to assess glenohumeral joint concentricity and rule out a locked posterior or anterior fracture-dislocation. If the patient is in too much pain to abduct the arm for a standard axillary view, a Velpeau axillary view can be obtained with the patient remaining in the sling.
While plain radiographs provide the initial diagnosis, a non-contrast Computed Tomography (CT) scan with 3D reconstructions has become the gold standard for preoperative planning in complex proximal humerus fractures. The CT scan allows the surgeon to precisely delineate the fracture lines, quantify the degree of tuberosity displacement, assess the volume and density of the humeral head bone stock, and identify subtle articular step-offs or head-splitting components that may be invisible on plain films. It is crucial to note that while CT scans dramatically improve the surgeon's ability to plan the trajectory of locking screws and anticipate the need for bone grafting, literature suggests they do not significantly improve the interobserver reliability of the Neer classification. Thus, the CT is a tool for execution, not merely categorization.
Operating Theater Setup and the Beach Chair Position
Optimal patient positioning is a critical determinant of intraoperative success, directly impacting visualization, reduction capability, and fluoroscopic access. For the vast majority of proximal humerus ORIF procedures, the beach chair (or modified Fowler) position is the gold standard. The patient is placed in a semi-seated posture, typically flexed between 45 and 60 degrees at the hips, with the knees slightly flexed to reduce sciatic nerve tension.

Crucially, the patient must be translated as far laterally on the operating table as safely possible. The medial border of the scapula should be supported, but the entire shoulder girdle must be free and unobstructed. This lateralized positioning allows the surgeon to fully extend and adduct the humerus, a maneuver that is frequently necessary to expose the greater tuberosity and apply the locking plate to the lateral cortex without the table impeding the drill or screwdriver. A lateral buttress or specialized beach chair attachment is utilized to secure the torso and prevent the patient from shifting during aggressive manipulation of the arm.

Fluoroscopy setup in the beach chair position requires specific coordination with the radiology technician. The C-arm base should be positioned at the head of the bed, posterior to the patient's shoulder. The arc of the C-arm is brought over the patient's chest and abdomen. This specific configuration allows the C-arm to rotate freely between a true AP view and a Scapular Y view without striking the sterile field or requiring the surgeon to alter the position of the reduced fracture. The surgeon must confirm adequate fluoroscopic visualization of the entire proximal humerus, including the articular surface and the diaphysis, before making the incision.

Step-by-Step Surgical Approach and Fixation Technique
The Deltopectoral Approach
The deltopectoral approach is the absolute workhorse for the internal fixation of proximal humerus fractures. It utilizes a true internervous plane between the deltoid muscle (innervated by the axillary nerve) and the pectoralis major muscle (innervated by the medial and lateral pectoral nerves). This approach provides unparalleled, extensile exposure to the anterior, lateral, and medial aspects of the proximal humerus without denervating any musculature.

The incision begins at the tip of the coracoid process and extends distally and slightly laterally, following the deltopectoral groove, for approximately 10 to 15 centimeters. Subcutaneous dissection reveals the deltopectoral fascia. The key superficial landmark is the cephalic vein. While there is debate regarding its management, the standard orthopedic teaching is to retract the cephalic vein laterally with the deltoid muscle. This preserves the numerous deltoid venous tributaries, minimizing postoperative deltoid edema and potential muscle necrosis.
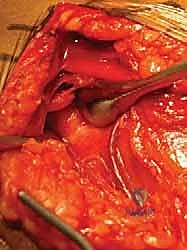
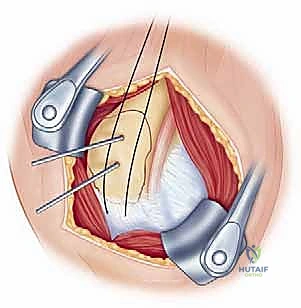
Once the internervous plane is developed, the surgeon retracts the deltoid laterally and the pectoralis major medially. The clavipectoral fascia is then incised vertically, lateral to the conjoined tendon (short head of the biceps and coracobrachialis). Care must be taken not to dissect medial to the conjoined tendon to avoid injury to the musculocutaneous nerve and the axillary neurovascular bundle. Deep to the clavipectoral fascia, the fracture hematoma will be encountered. Meticulous evacuation of this hematoma is essential; not only does it clear the visual field, but it also removes inflammatory mediators and allows for accurate identification of the fracture fragments and the bicipital groove.

Fracture Reduction and Provisional Fixation
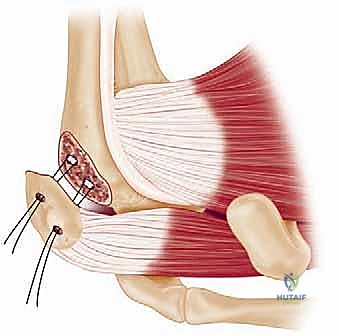
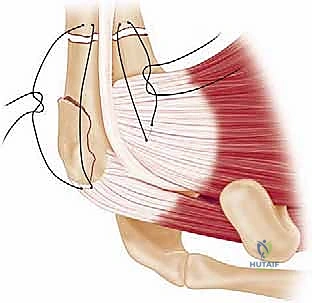
Reduction of a proximal humerus fracture is a complex spatial puzzle that must be solved before any definitive hardware is applied. The first and most critical step in reduction is gaining control of the tuberosities. Heavy, non-absorbable sutures (typically #2 or #5 FiberWire or Ethibond) are passed through the tendon-bone interface of the rotator cuff. Specifically, sutures are placed into the supraspinatus and infraspinatus tendons superiorly/posteriorly (controlling the greater tuberosity) and the subscapularis tendon anteriorly (controlling the lesser tuberosity).

These traction sutures act as "joysticks," allowing the surgeon to neutralize the muscular deforming forces discussed earlier. By pulling laterally and inferiorly on the greater tuberosity sutures, the superior migration caused by the supraspinatus is corrected. Simultaneously, the humeral shaft, which is often displaced anteromedially by the pectoralis major, must be mobilized. This is achieved by applying longitudinal traction, gentle external rotation, and using a blunt elevator or a bone hook to lever the shaft laterally and posteriorly into alignment with the articular segment.
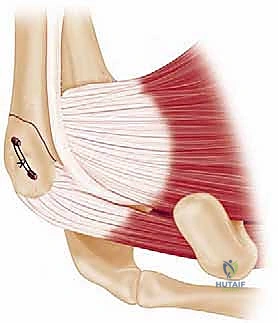
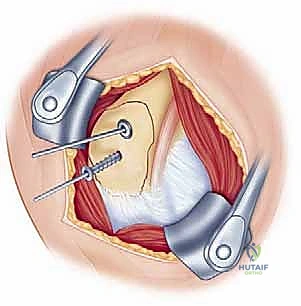
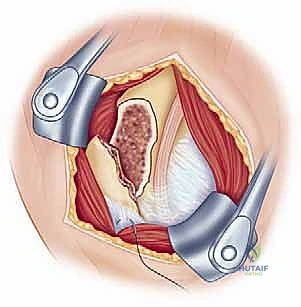
Once the tuberosities are reduced to the head and the shaft is aligned, provisional fixation is achieved using multiple 2.0mm or 2.5mm Kirschner wires (K-wires). These wires should be placed strategically so as not to interfere with the subsequent placement of the locking plate. Typically, wires are driven from the lateral cortex of the shaft, across the fracture site, and into the humeral head. Fluoroscopy in both the AP and axillary planes is absolutely mandatory at
Clinical & Radiographic Imaging Archive