Mastering Percutaneous Pinning for Proximal Humerus Fractures

Key Takeaway
This topic focuses on Mastering Percutaneous Pinning for Proximal Humerus Fractures, Proximal humerus fractures affect the upper humerus near the shoulder joint, classified by the Neer system into two-, three-, or four-part fractures based on displacement. Surgical decision-making for these, including options like **percutaneous pinning for proximal** humerus fractures, considers fracture type, displacement, osteonecrosis risk, and patient factors. These fractures involve the humeral head, greater and lesser tuberosities, and shaft.
Comprehensive Introduction and Patho-Epidemiology
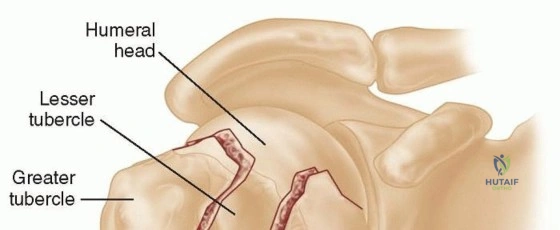
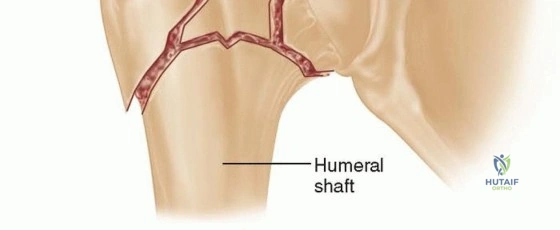
Proximal humerus fractures represent a significant and increasingly prevalent challenge in orthopedic traumatology, defined anatomically as disruptions of the proximal portion of the humerus that inherently involve the shoulder joint capsule and its complex ligamentous and tendinous attachments. The foundational understanding of these fractures is rooted in the early work of Codman, who astutely observed that fracture lines reliably divide the proximal humerus into distinct "parts" defined by the anatomic structures arising from early centers of ossification. This seminal observation paved the way for the development of the Neer classification system, which remains the universally accepted standard for categorizing these injuries today. The four fundamental parts identified by Codman and Neer include the articular head of the humerus, the greater tuberosity, the lesser tuberosity, and the humeral shaft. According to the Neer classification, proximal humerus fractures are categorized as two-, three-, or four-part fractures based not merely on the presence of fracture lines, but strictly on the degree of displacement of these specific segments.
Classically, displacement of a "part" is rigorously defined as greater than 1 centimeter of translation or greater than 45 degrees of angulation relative to its native anatomical position. It is critical for the orthopedic surgeon to recognize that displacement is a criterion for classification rather than an absolute indication for surgical intervention. The overarching surgical decision-making process is highly multifactorial, taking into account the specific fracture morphology, the degree and direction of displacement, the inherent risk of osteonecrosis (avascular necrosis), and a myriad of patient-specific considerations including physiologic age, functional demands, and medical comorbidities. The natural history of proximal humerus fractures dictates that approximately eighty-five percent of these injuries can be managed successfully with nonoperative modalities. Displacement at the surgical neck is generally better tolerated than displacement of the tuberosities; the shoulder's vast, multi-planar range of motion allows the upper extremity to functionally compensate for mild to moderate translational displacement or angulation at the surgical neck.
The pathogenesis of proximal humerus fractures demonstrates a classic bimodal epidemiological distribution. The vast majority of these injuries are considered "fractures of senescence," occurring in older individuals afflicted with age-related osteopenia or severe osteoporosis. In this demographic, fractures typically result from low-energy trauma, such as a simple mechanical fall from a standing height onto an outstretched hand or directly onto the lateral shoulder. Conversely, in the younger, physiologically robust population, proximal humerus fractures are almost exclusively the result of high-energy mechanisms, including motor vehicle collisions, motorcycle accidents, or significant falls from a height. These high-energy injuries are frequently associated with severe soft tissue trauma, concomitant upper extremity fractures, and neurological deficits. Axillary nerve neurapraxia is the most frequently encountered neurological complication, though it typically resolves spontaneously over a period of weeks to months with conservative management.
In the context of complex fracture patterns, particularly four-part fractures, the natural history is heavily influenced by the disruption of the tenuous vascular supply to the humeral head. Neer's classic series demonstrated an exceptionally high incidence of avascular necrosis—up to 45%—in standard four-part fractures. However, a critical exception exists in the form of the valgus-impacted four-part fracture. In this specific configuration, the incidence of avascular necrosis plummets to approximately 11%. This dramatic reduction in ischemic risk is attributed to the preservation of the medial periosteal hinge, which maintains critical blood supply to the articular segment via ascending branches of the posterior humeral circumflex artery. Understanding this patho-epidemiological distinction is paramount when selecting patients for percutaneous pinning, as valgus-impacted patterns with an intact medial hinge are uniquely amenable to this minimally invasive technique.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the surgical anatomy and biomechanics of the proximal humerus is the absolute prerequisite for successful percutaneous pinning. The proximal humerus arises embryologically from four distinct centers of ossification, which directly correspond to the functional "parts" of the bone: the humeral head (articular surface), the greater tuberosity, the lesser tuberosity, and the proximal humeral shaft. The greater tuberosity serves as the critical insertion site for the superior and posterior aspects of the rotator cuff, featuring three distinct anatomical facets for the insertion of the supraspinatus (superior facet), the infraspinatus (middle facet), and the teres minor (inferior facet) muscles. Biomechanically, these muscles exert a powerful superior and posterior deforming force on the greater tuberosity when fractured.
The lesser tuberosity serves as the singular insertion site for the subscapularis muscle, which acts as the primary internal rotator of the shoulder. When the lesser tuberosity is fractured and displaced, the subscapularis exerts a strong medial and internal deforming force. Between the upper border of the subscapularis and the anterior border of the supraspinatus lies the rotator interval, a complex anatomical space bridged by the coracohumeral and superior glenohumeral ligaments. The long head of the biceps tendon runs deep to the rotator interval tissue, lying in a shallow bicipital groove on the anterior aspect of the proximal humerus before entering the glenohumeral joint intra-articularly. The proximal 3 cm of the long head of the biceps tendon is a critical surgical landmark; notably, the fracture line separating the greater and lesser tuberosities invariably propagates just posterior to the bicipital groove.
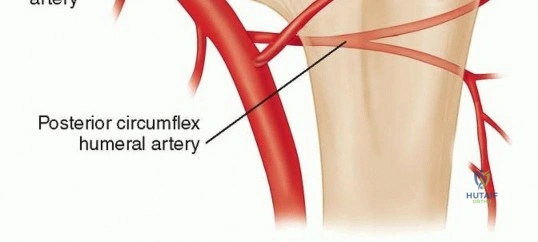
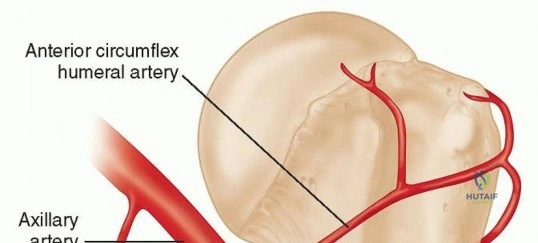
The vascular anatomy of the proximal humerus is notoriously precarious and dictates the survivability of the articular segment following trauma. The anterior humeral circumflex artery (AHCA) courses laterally along the inferior border of the subscapularis muscle. It gives rise to the critical anterolateral branch (also known as the ascending branch of the AHCA), which travels superiorly along the lateral aspect of the bicipital groove. This vessel enters the humeral head at the proximal-most aspect of the groove and has historically been cited as providing approximately 85% of the blood supply to the humeral head. However, more recent microvascular injection studies have highlighted the equally vital role of the posterior humeral circumflex artery (PHCA). The PHCA gives off several small, robust branches that run adjacent to the inferior capsule of the shoulder, providing substantial intraosseous perfusion to the inferior and medial quadrants of the humeral head.
In the setting of valgus-impacted fractures, the integrity of the medial periosteal hinge is the lifeline of the humeral head. The blood supply is maintained in most valgus-impacted fractures by the ascending branches from the PHCA traveling along this intact medial periosteal sleeve. Disruption of this medial hinge, particularly when the calcar segment is displaced laterally or comminuted, exponentially increases the risk of avascular necrosis. Furthermore, the biomechanical forces exerted by the pectoralis major and latissimus dorsi must be counteracted during closed reduction. The pectoralis major inserts on the proximal shaft lateral to the biceps groove, pulling the humeral shaft anteriorly and medially, while the latissimus dorsi inserts medial to the groove, contributing to the adduction and internal rotation deformity of the shaft relative to the proximal fragments.
Exhaustive Indications and Contraindications
The decision to proceed with percutaneous pinning of a proximal humerus fracture requires meticulous patient selection, balancing the biomechanical stability of the fracture pattern against the biological quality of the patient's bone. A comprehensive history and physical examination are the first steps in this algorithm. The surgeon must differentiate between low-energy fragility fractures and high-energy traumatic injuries. Elderly individuals sustaining low-energy falls often present with fracture patterns that are highly amenable to minimally invasive fixation; the displacement is frequently manageable, and the periosteal sleeve between fracture fragments—as well as the rotator cuff itself—often remains intact as a contiguous sleeve. These biological factors greatly facilitate closed reduction and percutaneous stabilization.

Conversely, younger patients with high-energy injuries frequently exhibit severe fracture fragment displacement, traumatic rotator cuff tears propagating between the tuberosities, and complete disruption of the periosteal sleeve. While these factors do not absolutely preclude percutaneous pinning, they render the technique exponentially more challenging and significantly increase the risk of loss of fixation. Physical examination must rigorously assess skin integrity, the presence of ecchymosis (which often tracks down the arm and across the chest wall over subsequent days), and any deformity consistent with concomitant glenohumeral dislocation. A meticulous neurological exam is mandatory, paying particular attention to the axillary nerve by testing sensation over the lateral deltoid and assessing isometric deltoid contraction, recognizing that pain will severely limit this assessment.
Indications for percutaneous pinning include two-part surgical neck fractures, select three-part fractures, and valgus-impacted four-part fractures, provided the patient possesses adequate bone stock to afford purchase for the pins. The ideal candidate has substantial fracture fragments with minimal comminution of the tuberosities and, critically, minimal or no comminution at the medial calcar region. Historically, 1 cm of displacement was the threshold for operative intervention of the greater tuberosity; however, contemporary literature supports operative fixation for even 5 mm of superior displacement, as this severely alters the biomechanics of the rotator cuff and leads to devastating subacromial impingement.
Contraindications to percutaneous pinning must be strictly respected to avoid catastrophic failure. Poor bone quality (severe osteoporosis) is a primary contraindication, as the cancellous bone of the humeral head will fail to provide adequate pull-out strength for smooth or threaded pins, necessitating a more stable construct such as a locking plate or arthroplasty. Comminution of the greater tuberosity precludes pin fixation, as the fragmented bone cannot be captured by a wire; these injuries require open suture fixation through the tendon-bone junction. Furthermore, percutaneous pinning is absolutely contraindicated in noncompliant patients, patients with severe cognitive impairment, or those unreliable for close postoperative follow-up, given the inherent risks of pin tract infection and catastrophic pin migration.
| Parameter | Indications for Percutaneous Pinning | Contraindications for Percutaneous Pinning |
|---|---|---|
| Fracture Pattern | 2-part surgical neck, select 3-part, valgus-impacted 4-part | Head-split fractures, anatomical neck fractures, highly comminuted 4-part |
| Bone Quality | Good to moderate bone stock | Severe osteoporosis (cortical thinning, cystic head) |
| Medial Calcar | Intact medial hinge, no calcar comminution | Severe medial calcar comminution (unstable base) |
| Tuberosities | Large, intact fragments | Highly comminuted tuberosities requiring suture fixation |
| Patient Profile | Compliant, reliable for frequent follow-up | Non-compliant, severe dementia, substance abuse |
Pre-Operative Planning, Templating, and Patient Positioning
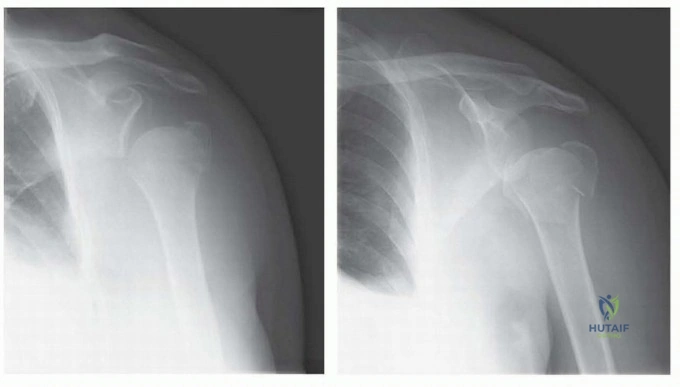
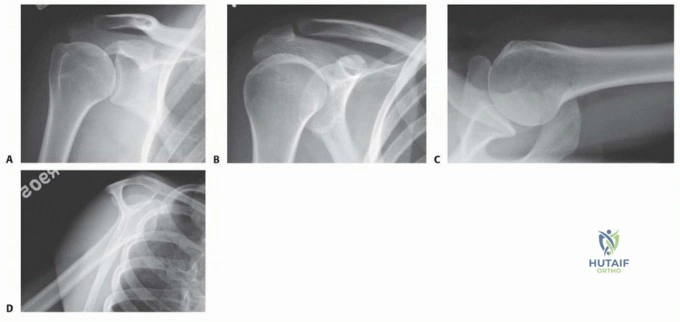
Preoperative planning is the cornerstone of successful percutaneous pinning, beginning with an exhaustive review of a dedicated orthopedic trauma radiographic series. The standard series must include a true anteroposterior (AP) view of the glenohumeral joint (Grashey view), a scapular Y lateral view, and an axillary lateral view. The standard AP view of the shoulder can be highly misleading, particularly in the case of surgical neck fractures, as the anterior displacement of the humeral shaft driven by the pectoralis major may not be appreciated. The axillary view is non-negotiable; it is the definitive study for assessing the relationship of the humeral head to the glenoid (ruling out subtle dislocations) and for evaluating the anterior-posterior displacement of the tuberosities.
In the modern era, a computed tomography (CT) scan with three-dimensional (3D) reconstructions is highly recommended, and arguably standard of care, for all complex proximal humerus fractures. The CT scan provides invaluable information regarding the exact extent of articular involvement, the degree of tuberosity comminution, and the precise length of the intact medial calcar. During the templating phase, the surgeon must mentally map the trajectories of the proposed pins. Standard constructs typically require two to three pins driven from the lateral shaft into the humeral head (directed inferior to superior) and one to two pins securing the greater tuberosity to the head and shaft (directed superior-lateral to inferior-medial).

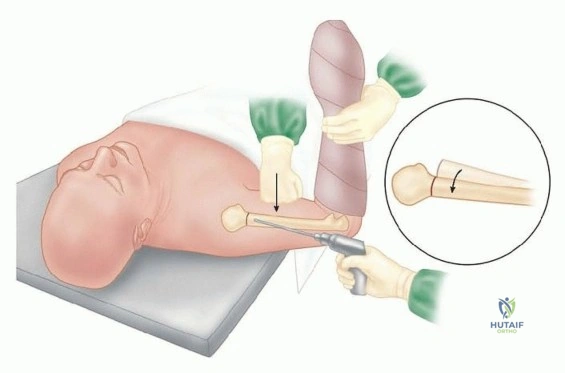
Patient positioning is critical to facilitate both the surgical approach and unimpeded intraoperative fluoroscopy. The procedure is universally performed with the patient in the 45-degree beach-chair position. This semi-upright posture utilizes gravity to assist in reducing the proximally migrated humeral shaft. The patient must be positioned far laterally on the operating table, or ideally on a specialized radiolucent shoulder surgery positioning device, ensuring that the entire shoulder girdle is clear of metallic table components. The operative arm must be draped completely free to allow for dynamic manipulation, traction, and rotation during the closed reduction maneuvers.

The C-arm fluoroscope is brought in parallel to the patient, entering from the cephalad direction (over the head of the bed). This specific orientation leaves the lateral and anterior aspects of the shoulder completely accessible for instrumentation and pin insertion. Before formal prepping and draping, the surgeon must perform a fluoroscopic "dry run." It is imperative to confirm that perfect orthogonal views (true AP and true axillary) can be obtained seamlessly without moving the patient or compromising the sterile field. Failure to establish reliable fluoroscopic visualization prior to incision will inevitably lead to malreduction, errant pin placement, and prolonged operative times.
Step-by-Step Surgical Approach and Fixation Technique
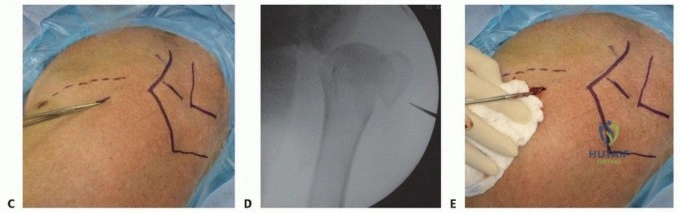
The surgical technique for percutaneous pinning relies heavily on the surgeon's ability to achieve an anatomic or near-anatomic closed reduction utilizing indirect manipulation and percutaneous leverage. The procedure begins by establishing a "reduction portal," analogous to an arthroscopic portal, typically located off the anterolateral corner of the acromion or directly over the fracture hematoma at the level of the surgical neck. This small incision allows the introduction of a blunt elevator, a periosteal freer, or a specialized reduction tool (such as a ball-spike pusher) directly into the fracture site.

To reduce a standard surgical neck fracture, longitudinal traction is applied to the arm while the shoulder is gently flexed and abducted. This maneuver counteracts the deforming forces of the pectoralis major. If the shaft remains medialized, an instrument introduced through the reduction portal can be used to manually lever the humeral shaft laterally while simultaneously pushing the humeral head medially. In the case of a valgus-impacted fracture, the lateral aspect of the humeral head is often impacted into the metaphysis. A Cobb elevator or a specialized tamp can be inserted percutaneously into the fracture plane to gently disimpact the head and elevate it into a varus, anatomically reduced position, taking extreme care not to hinge open the critical medial periosteal sleeve.

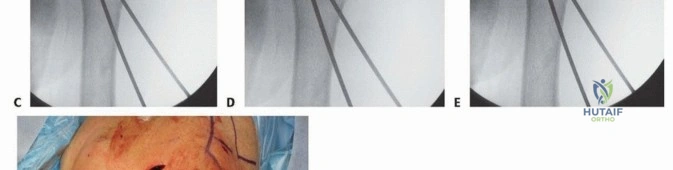
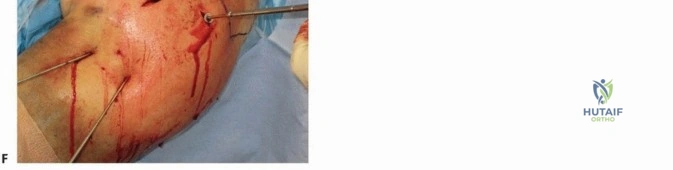
Once provisional reduction is achieved and confirmed on orthogonal fluoroscopic views, fixation is initiated. The primary construct typically involves the placement of 2.5 mm or 3.0 mm threaded terminally threaded pins (Schanz pins or heavy K-wires). The first pin is usually introduced at the lateral cortex of the humeral shaft, approximately 2 to 3 cm distal to the fracture line, and directed proximally and medially into the inferior quadrant of the humeral head. A second, parallel or slightly divergent pin is placed to secure the shaft-to-head reduction. It is critical that these pins engage the dense subchondral bone of the humeral head to maximize pull-out strength, but they must not penetrate the articular cartilage.

Following shaft-to-head fixation, the tuberosities must be addressed. If the greater tuberosity is displaced, it is reduced using a percutaneous hook or heavy suture passed through the rotator cuff, pulling the fragment anteriorly and inferiorly into its bed. It is then secured with one or two pins directed from the lateral aspect of the greater tuberosity, traversing the fracture line, and embedding into the medial articular segment of the humeral head.
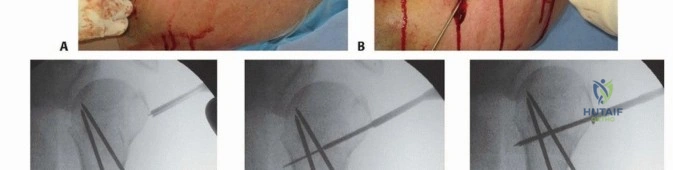
The final, and arguably most crucial, step of the procedure is pin management. After confirming perfect hardware placement and fracture reduction via live fluoroscopy in multiple planes, the pins must be cut. To prevent catastrophic inward migration, the pins are typically bent at a 90-degree angle just outside the lateral cortex of the bone, cut short, and buried beneath the deltoid muscle but superficial to the deep fascia, or left protruding through the skin for easy removal in the clinic. Leaving pins proud through the skin increases the risk of superficial tract infection but eliminates the need for a secondary surgical procedure for removal and drastically reduces the risk of intrathoracic pin migration.
Complications, Incidence Rates, and Salvage Management
Despite its minimally invasive nature, percutaneous pinning of proximal humerus fractures carries a unique and potentially severe complication profile that demands deep respect from the operating surgeon. The most feared complication is hardware migration. Because the pins are placed in cancellous, often osteoporotic bone subject to the massive dynamic forces of the shoulder girdle, they can loosen and migrate. Outward migration results in loss of fixation and prominent hardware, but inward migration can be fatal. Pins migrating medially have been reported to penetrate the thoracic cavity, causing pneumothorax, hemothorax, cardiac tamponade, and catastrophic vascular injury. To mitigate this, pins must be definitively bent or capped, and patients must be followed with weekly radiographs during the initial postoperative period.

Infection is another significant concern, particularly when pins are left protruding through the skin. Superficial pin tract infections occur in approximately 5% to 10% of cases and can usually be managed successfully with oral antibiotics and local wound care. However, deep infections tracking into the glenohumeral joint or the fracture hematoma require immediate operative debridement, pin removal, and conversion to an external fixator or antibiotic spacer. Avascular necrosis (AVN) remains a biological threat, particularly in three- and four-part fractures. While the percutaneous technique minimizes iatrogenic soft tissue stripping, the initial trauma may have already irreversibly damaged the anterior and posterior humeral circumflex arterial supply.
Loss of reduction and subsequent malunion or nonunion are complications directly related to patient selection and bone quality. In patients with severe osteoporosis, the cancellous bone may simply fail to hold the pins, leading to varus collapse of the humeral head and superior migration of the greater tuberosity. When percutaneous pinning fails, salvage management is highly complex. In younger patients with adequate bone stock, revision to open reduction and internal fixation (ORIF) with a locking plate and structural bone grafting may be attempted. However, in the elderly population, salvage almost universally dictates conversion to arthroplasty.
Historically, hemiarthroplasty was the salvage procedure of choice, but outcomes were heavily dependent on tuberosity healing, which is notoriously poor in the revision setting. Today, reverse total shoulder arthroplasty (RTSA) is the gold standard for salvage of failed proximal humerus fracture fixation in the elderly. RTSA bypasses the need for rotator cuff integrity and tuberosity healing, relying instead on the deltoid to power the shoulder, providing reliable pain relief and functional restoration even in the face of catastrophic tuberosity resorption or nonunion.
| Complication | Estimated Incidence | Prevention
Clinical & Radiographic Imaging Archive