Crucial Positioning for General Anaesthesia in Pediatric Orthopaedics

Key Takeaway
Learn more about Crucial Positioning for General Anaesthesia in Pediatric Orthopaedics and how to manage it. Epiphysiodesis is a pediatric orthopedic procedure that destroys the physis to equalize leg length discrepancies, primarily targeting growth plates around the knee. Indications include true LLD of 2–5 cm or greater than 7 cm. Preoperative planning involves determining LLD at maturity. Proper **positioning general anaesthesia** is crucial for surgical success and patient safety, mitigating risks like neurovascular injury and infection.
You are managing a 14-year-old patient who presents with a symptomatic unstable Slipped Capital Femoral Epiphysis (SCFE). Describe your approach to positioning this patient for theatre and explain the rationale for your choice, specifically regarding the use of a fracture table.
Candidate: I would place the patient supine on a radiolucent flat table. I would avoid using a fracture table with traction because it is contraindicated in unstable SCFE as it risks further disruption of the already compromised retinacular blood supply, leading to avascular necrosis (AVN). I would use a bump under the ipsilateral sacrum to correct the external rotation and improve fluoroscopic access.
Failing to distinguish between "stable" and "unstable" SCFE. Candidates often reflexively reach for the fracture table (standard for adult hip fractures) without considering the pediatric vascular anatomy (Medial Circumflex Femoral Artery) or the extreme vulnerability of the capital femoral physis to longitudinal traction.
The candidate explicitly identifies that longitudinal traction and forced internal rotation on a fracture table are absolute contraindications for an unstable SCFE. They highlight the "unstable" nature (Loder criteria) as a medical emergency. They structure the response by: (1) Confirming the patient must be on a flat radiolucent table, (2) Emphasizing the Medial Circumflex Femoral Artery (MFCA) is the primary risk, and (3) Explaining that the "sacral bump" technique is the safe method to manipulate the extremity into the desired position for orthogonal (AP/Lateral) fluoroscopy without applying dangerous distracting forces.
You are performing a percutaneous epiphysiodesis to manage a limb length discrepancy. What specific fluoroscopic precautions are necessary, and why is "perfecting the arc" essential before the skin incision?

Candidate: I need perfect AP and lateral views of the physis. The C-arm should be positioned to allow rotation around the knee without moving the leg. If the positioning is not orthogonal, I risk off-center drilling, which could lead to an incomplete epiphysiodesis, continued angular deformity, or hardware failure.
Overlooking the "C-arm around the patient, not patient around the C-arm" rule. A failing candidate might imply that moving the patient's leg into different positions to find the view is acceptable—this is incorrect, as it increases the risk of contamination and loses the spatial orientation required for precise central drilling.
A high-scoring answer emphasizes orthogonality as the key to preventing "physeal drift." The candidate should state that the drill path must target the absolute center of the physis on both views. They should mention the Green-Anderson or Paley Multiplier as the basis for the plan, and note that ensuring the C-arm can sweep 90 degrees without sterile field compromise is a prerequisite for surgical safety.
During an open reduction of DDH, you notice the femoral head is difficult to reduce. What are the common intra-articular obstacles to concentric reduction, and how do you manage them?

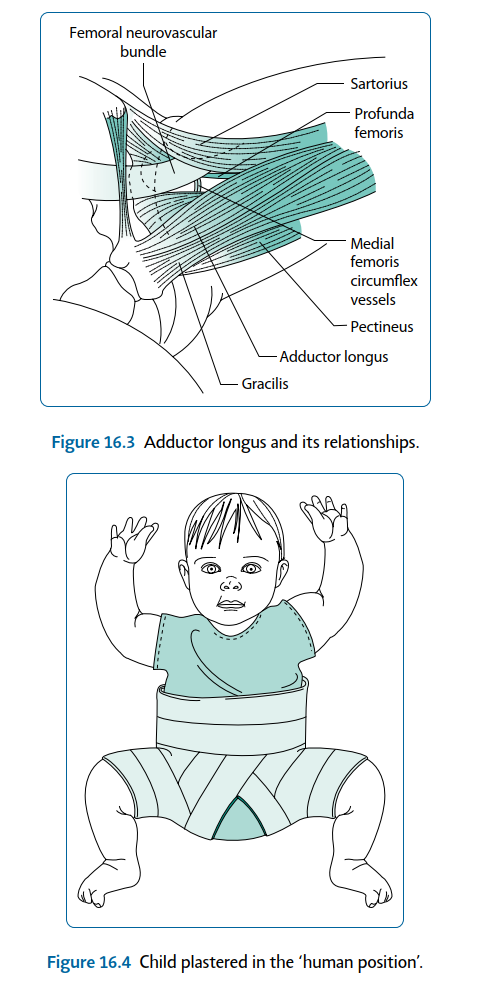
Candidate: Obstacles include the ligamentum teres, the pulvinar (fibrofatty tissue), the inverted limbus (labrum), and the transverse acetabular ligament. I would release the iliopsoas, perform a T-shaped arthrotomy, excise the ligamentum teres and pulvinar, and incite the transverse acetabular ligament to achieve a stable, concentric reduction.
Listing the obstacles but failing to mention the transverse acetabular ligament. Many candidates forget that the labrum is often inverted (limbus) and that simple reduction will fail if this is not addressed.
The candidate provides a systematic, sequential surgical checklist: 1) Release the iliopsoas (the primary dynamic tether), 2) Clear the pulvinar and excise the hypertrophied ligamentum teres, 3) Identify and release the transverse acetabular ligament, and 4) Check for stability. They must link this to the "safe zone" of abduction, warning against excessive abduction (>60°) to avoid iatrogenic AVN of the femoral head.
