Pediatric Cervical Spine: Odontoid Anomalies & Surgery
Key Takeaway
Congenital anomalies of the pediatric cervical spine, particularly os odontoideum, present significant risks of atlantoaxial instability and compressive myelopathy. This comprehensive guide details the embryology, vascular anatomy, and radiographic evaluation of odontoid anomalies. It provides step-by-step surgical techniques for atlantoaxial and occipitocervical fusion, emphasizing biomechanical principles, preoperative traction, and precise graft placement to ensure optimal neurological outcomes in pediatric patients.
Comprehensive Introduction and Patho-Epidemiology
Although congenital anomalies of the pediatric cervical spine—specifically those involving the odontoid process (dens)—are relatively rare in the general population, they represent a critical diagnostic and therapeutic challenge for the orthopedic surgeon and neurosurgeon alike. These structural anomalies can precipitate profound atlantoaxial instability, leading to catastrophic neurological consequences, including compressive myelopathy, vertebral artery compression, vertebrobasilar insufficiency, or sudden death from minor trauma. The inherent hypermobility of the pediatric cervical spine, combined with the disproportionately large head-to-body ratio in children, exacerbates the biomechanical stresses placed upon a structurally deficient craniovertebral junction. Consequently, a comprehensive understanding of these anomalies is non-negotiable for clinicians managing pediatric spinal deformities.
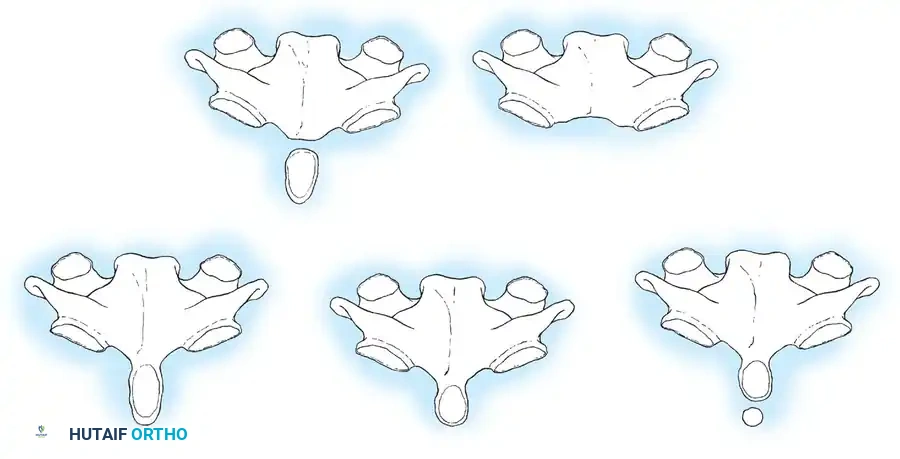
Congenital anomalies of the odontoid are broadly categorized into three distinct morphological groups: aplasia (agenesis), hypoplasia, and os odontoideum. Aplasia is the complete absence of the odontoid process, an exceedingly rare condition that results in profound and immediate C1-C2 instability. Hypoplasia involves the partial development of the odontoid, where the osseous structure varies from a diminutive, peg-like projection to a slightly undersized dens. By far the most clinically significant and frequently encountered anomaly is the os odontoideum. In this condition, the odontoid presents as an independent, oval or round ossicle with a smooth, sclerotic cortical border. It is separated from the body of the axis (C2) by a transverse gap, leaving the apical segment devoid of structural support and rendering the transverse ligament functionally incompetent.

The etiology of os odontoideum remains a subject of intense academic debate, with evidence supporting both congenital and acquired (post-traumatic) origins. The congenital theory proposes a failure of fusion of the apex (ossiculum terminale) or a failure of fusion of the odontoid to the axis. However, this theory fails to explain why the gap in os odontoideum typically occurs at the level of the superior articulating facets of C2, rather than below the facets where the neurocentral synchondrosis is anatomically located. Conversely, the acquired theory, heavily championed by Fielding and others, suggests that an unrecognized fracture at the base of the odontoid in early childhood is the most common cause. The distraction force exerted by the intact alar ligaments pulls the fractured tip away from its base, while the tenuous blood supply leads to osteonecrosis and subsequent nonunion. Acquired os odontoideum has also been well-documented following iatrogenic interventions, such as halo-pelvic traction, where excessive distraction forces compromise the apical arcade.
Epidemiologically, odontoid anomalies exhibit a markedly higher prevalence in patients with specific syndromic conditions. Children with Down syndrome (Trisomy 21) frequently present with generalized ligamentous laxity and osseous anomalies of the upper cervical spine, necessitating rigorous screening protocols. Similarly, osteochondrodysplasias such as Morquio syndrome (Mucopolysaccharidosis Type IV) and spondyloepiphyseal dysplasia congenita are notorious for producing severe odontoid hypoplasia and resultant atlantoaxial subluxation due to defective endochondral ossification. Klippel-Feil syndrome, characterized by congenital fusion of cervical vertebrae, often places exaggerated biomechanical stress on the unfused adjacent segments, frequently unmasking or exacerbating instability at a dysplastic craniovertebral junction. A high index of suspicion must be maintained when evaluating these vulnerable populations, as insidious neurological decline can easily be misattributed to the underlying syndrome rather than a treatable spinal deformity.
Detailed Surgical Anatomy and Biomechanics
Knowledge of the embryological development and vascular supply of the odontoid is paramount to understanding the etiology of these anomalies and formulating safe surgical strategies. The odontoid process is phylogenetically derived from the mesenchyme of the first cervical vertebra (atlas). During normal embryogenesis, the centrum of C1 separates from the neural arches of the atlas and migrates caudally to fuse with the body of the axis (C2). A vestigial disc space between C1 and C2 forms a synchondrosis within the body of the axis, well below the level of the superior articular facets. The apex (tip) of the odontoid is derived from the most caudal occipital sclerotome, known as the proatlas. This separate ossification center, the ossiculum terminale, appears at approximately 3 years of age and typically fuses with the main body of the dens by age 12. Anomalies isolated strictly to this terminal portion rarely cause clinical instability, as the primary transverse ligament remains competent.
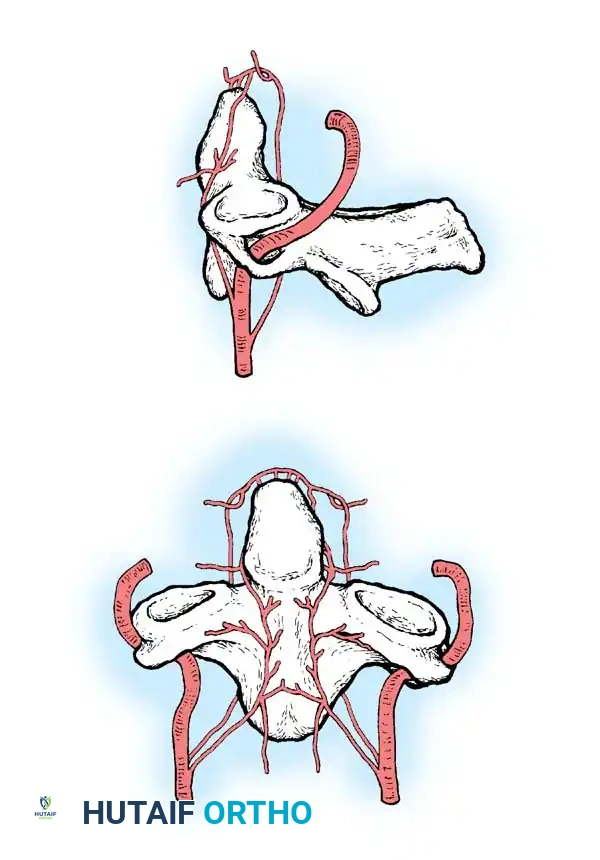
The arterial blood supply to the odontoid is highly specialized, tenuous, and derived from both the vertebral and carotid arterial systems. The vertebral artery gives off anterior and posterior ascending arteries that originate at the level of C3. These vessels ascend anterior and posterior to the odontoid, anastomosing superiorly to form a critical vascular network known as the apical arcade. Furthermore, the most rostral portion of the extracranial internal carotid artery provides "cleft perforators" that supply the superior pole of the odontoid. This peculiar vascular arrangement creates a biomechanical and ischemic vulnerability. The synchondrosis prevents direct vascularization of the odontoid from the C2 body, and the surrounding synovial joint cavity of the atlantoaxial articulation prevents vascular ingrowth from C1. This watershed vascularity heavily predisposes the odontoid to nonunion, osteonecrosis, and resorption following even minor trauma, strongly supporting the acquired theory of os odontoideum.
Biomechanically, the craniovertebral junction is the most complex articulation in the human axial skeleton, designed to sacrifice intrinsic osseous stability for a massive range of motion. The atlantoaxial joint is responsible for approximately 50% of the total axial rotation of the cervical spine. In the absence of interlocking facet joints, stability relies entirely on a robust ligamentous complex. The transverse ligament, a thick band of collagen spanning the medial tubercles of the C1 lateral masses, acts as the primary restraint against anterior translation of C1 on C2. It securely pins the odontoid against the anterior arch of the atlas. The alar ligaments, originating from the superolateral aspects of the dens and inserting onto the medial aspects of the occipital condyles, act as secondary restraints, limiting axial rotation and lateral bending.
In the setting of aplasia, hypoplasia, or os odontoideum, the structural keystone (the dens) is absent or unmoored. Consequently, the transverse ligament has no solid osseous structure to purchase against, rendering it functionally incompetent. This permits gross, multidirectional atlantoaxial instability. During flexion, the anterior arch of C1 translates anteriorly, dragging the free ossicle (in os odontoideum) with it, while the intact posterior arch of C1 acts as a guillotine against the spinal cord. During extension, the anterior arch of C1 can subluxate posteriorly over the deficient dens, compressing the cord between the anterior arch of C1 and the posterior body of C2. Furthermore, the chronic, repetitive microtrauma induced by this instability frequently incites a hypertrophic inflammatory response behind the dens—the retrodental pannus—which further narrows the spinal canal and exacerbates compressive myelopathy.
Exhaustive Indications and Contraindications
The clinical presentation of pediatric odontoid anomalies is notoriously variable, ranging from asymptomatic incidental findings to acute tetraplegia. Consequently, the decision to proceed with operative stabilization requires a meticulous synthesis of clinical symptomatology, dynamic radiographic parameters, and advanced neuroimaging. The primary objective of surgical intervention is to stabilize the abnormal atlantoaxial joint, preventing catastrophic subluxation that could lead to permanent spinal cord injury, while simultaneously attempting to preserve as much functional motion as possible. Prophylactic stabilization of asymptomatic patients with minimal radiographic instability remains a topic of spirited debate; however, given the unpredictable nature of pediatric trauma and the devastating consequences of cord injury, the threshold for surgical intervention in this demographic is generally lower than in adults.

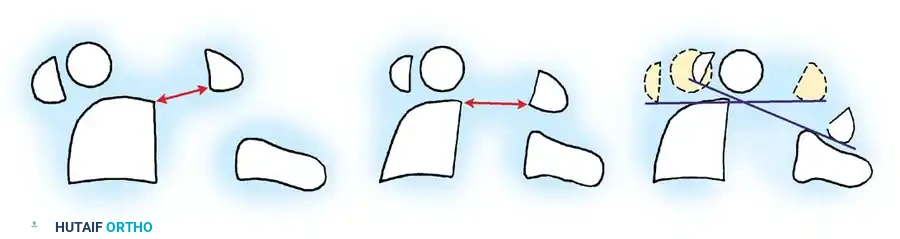
Surgical indications are heavily predicated on precise radiographic metrics. Lateral flexion and extension radiographs are mandatory to document the extent of dynamic instability. In children with os odontoideum, the free ossicle is typically fixed to the anterior arch of C1 via intact synovial and ligamentous attachments, moving in unison with it. Therefore, the traditional Atlantodental Interval (ADI) is rendered useless. Instead, instability is measured by projecting a line superiorly from the posterior body of the axis and measuring the distance to the posterior border of the anterior arch of the atlas. Translation exceeding 4 to 5 mm in the pediatric population is generally considered an absolute indication for stabilization. Furthermore, the Space Available for the Cord (SAC), measured from the posterior aspect of the odontoid or C2 body to the nearest posterior structure (usually the posterior arch of C1), is a critical prognosticator. A SAC of less than 13 mm is highly predictive of imminent neurological injury and mandates urgent surgical decompression and fusion.
Contraindications to isolated posterior C1-C2 fusion must be carefully evaluated to prevent disastrous intraoperative complications. An absolute contraindication to standard posterior wiring or screw constructs is an irreducible anterior spinal cord compression caused by a fixed, posteriorly displaced os odontoideum or a massive, fibrotic retrodental pannus that fails to reduce with preoperative skeletal traction. Fusing the spine in situ in this scenario would permanently lock the cervical spine in a critically stenotic state, guaranteeing progressive myelopathy. In such cases, an anterior transoral or endoscopic endonasal decompression must precede posterior stabilization. Furthermore, incomplete development, assimilation, or fracture of the posterior arch of C1 precludes the use of traditional sublaminar wiring techniques (e.g., Gallie or Brooks-Jenkins) and necessitates either rigid screw fixation or extension of the fusion construct to the occiput.
| Category | Indications for Surgical Intervention | Contraindications to Isolated Posterior Fusion |
|---|---|---|
| Clinical | - Progressive neurological deficit (myelopathy, weakness, hyperreflexia) - Transient paresis or paresthesias following minor trauma - Intractable mechanical neck pain or torticollis refractory to conservative care - Vertebrobasilar insufficiency (drop attacks, vertigo, visual disturbances) |
- Active systemic infection or severe localized osteomyelitis - Medically unstable patient unfit for general anesthesia - Asymptomatic patient with < 3mm translation and no high-risk activities (Relative) |
| Radiographic | - Atlantoaxial translation > 4-5 mm on dynamic flexion/extension views - Space Available for the Cord (SAC) < 13 mm - Sagittal plane rotation angle > 20 degrees - Instability Index > 40% - Progressive instability documented on serial radiographs |
- Irreducible anterior cord compression (fixed subluxation or massive pannus) - Absent, hypoplastic, or assimilated posterior arch of C1 (Contraindicates wiring) - Aberrant vertebral artery anatomy crossing the planned screw trajectory (Relative) |
| Syndromic | - High-risk syndromic patients (Down, Morquio, SED) exhibiting any signs of progressive instability or cord signal change on MRI | - Severe concomitant cranial settling/basilar invagination requiring occipitocervical extension |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful surgical management of pediatric odontoid anomalies. The margin for error at the craniovertebral junction is measured in millimeters, and the juxtaposition of the spinal cord, vertebral arteries, and delicate venous plexuses demands exhaustive advanced imaging. High-resolution Computed Tomography (CT) with 3D reconstructions is mandatory to delineate the complex osseous anatomy. The surgeon must evaluate the integrity of the C1 posterior arch, the dimensions of the C1 lateral masses, and the morphometry of the C2 pedicles and pars interarticularis. In the pediatric population, osseous structures may be too diminutive to accommodate standard 3.5 mm cervical screws, necessitating the use of 3.0 mm or even 2.7 mm instrumentation, or dictating a shift toward wiring techniques or occipitocervical extension.
CT Angiography (CTA) or Magnetic Resonance Angiography (MRA) has become an indispensable component of the preoperative workup. The vertebral artery exhibits highly variable anatomy at the C1-C2 junction. Anomalies such as a high-riding vertebral artery, a ponticulus posticus (arcuate foramen), or an anomalous fenestrated artery can place the vessel directly in the trajectory of a C1 lateral mass or C2 pedicle screw. Magnetic Resonance Imaging (MRI) is equally critical for evaluating the soft tissue elements. T2-weighted sequences must be scrutinized for intramedullary hyperintensity (myelomalacia), which signifies irreversible cord damage and correlates with a poorer prognosis for neurological recovery. MRI is also the gold standard for identifying and quantifying the volume of retrodental pannus. Crucially, the surgeon must determine if the pannus and the subluxation reduce dynamically; if they do not, preoperative traction is required.
In patients presenting with neurological deficits, severe subluxation, or a massive pannus, preoperative skeletal traction using Gardner-Wells tongs or a pediatric halo ring is highly recommended. Traction is typically initiated at 2 to 3 pounds and gradually increased under serial radiographic and neurological monitoring. The goal of traction is to achieve gradual, controlled reduction of the atlantoaxial articulation, relieve spinal cord irritation, and allow for potential recovery of neurological function prior to surgical fusion. Achieving and maintaining anatomical reduction preoperatively is the most critical prerequisite for a successful C1-C2 fusion, as it transforms a complex reduction maneuver into a straightforward in situ stabilization. If the deformity is completely reducible, the reactive retrodental pannus will typically resorb spontaneously over several months following rigid posterior stabilization, obviating the need for morbid anterior transoral resection.
Patient positioning in the operating room is a high-risk evolution that requires seamless coordination between the orthopedic surgeon, the anesthesiologist, and the neuromonitoring team. The patient is typically positioned prone on a Jackson spinal table. The head is rigidly immobilized using a radiolucent Mayfield cranial fixator, ensuring that the neck is maintained in a neutral, anatomically reduced position. Extreme flexion must be avoided, as it can acutely exacerbate cord compression. A military tuck position is utilized, with the shoulders taped down gently to facilitate lateral fluoroscopic visualization of the lower cervical spine. Continuous intraoperative neuromonitoring, including Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is mandatory. Baseline signals must be obtained prior to positioning, immediately after turning the patient prone, and continuously throughout the exposure, instrumentation, and reduction phases to detect any impending ischemic or mechanical insult to the spinal cord.
Step-by-Step Surgical Approach and Fixation Technique
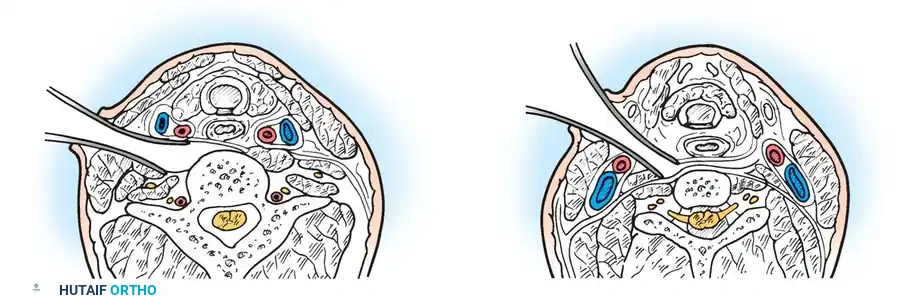
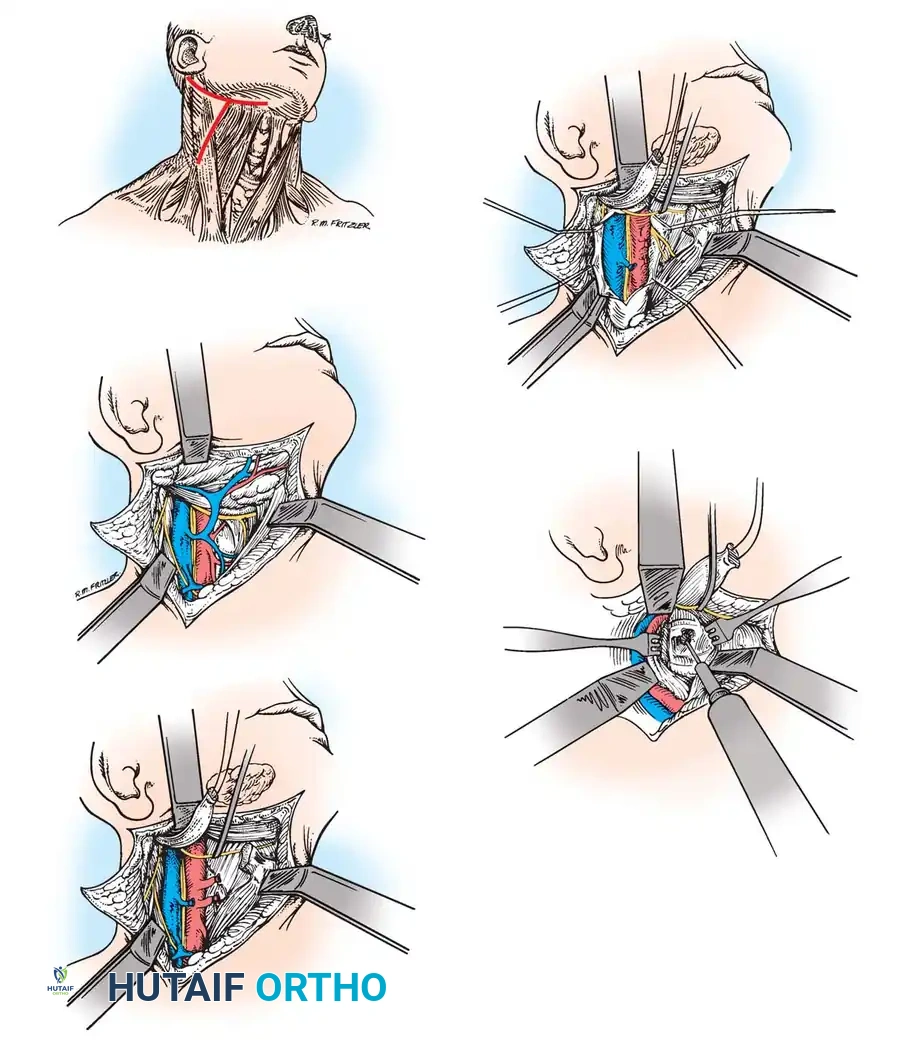
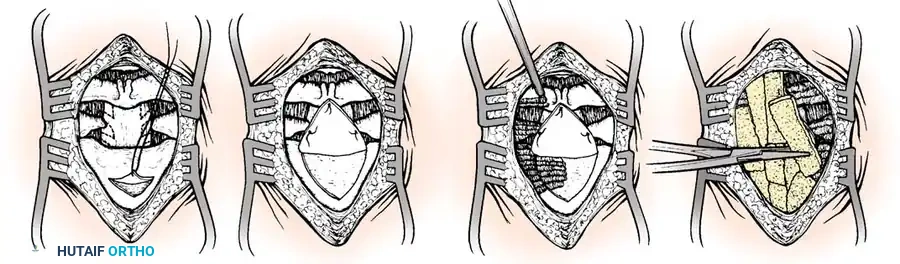
The surgical approach to the pediatric craniovertebral junction requires meticulous soft tissue dissection to minimize morbidity and preserve the vital stabilizing musculature. A standard posterior midline longitudinal incision is made from the external occipital protuberance to the spinous process of C3. The avascular ligamentum nuchae is sharply divided to expose the bifid spinous process of C2 and the posterior tubercle of C1. Subperiosteal dissection is carried out laterally. Extreme caution must be exercised when exposing the posterior arch of C1; dissection should not proceed further than 1.5 cm lateral to the midline to avoid catastrophic injury to the vertebral artery as it courses through the vertebral groove (sulcus arteriae vertebralis) on the superior surface of the C1 arch. The C2 nerve root and the surrounding venous plexus are identified and carefully managed to expose the C1-C2 facet joints for preparation.
Posterior Atlantoaxial Wiring Techniques
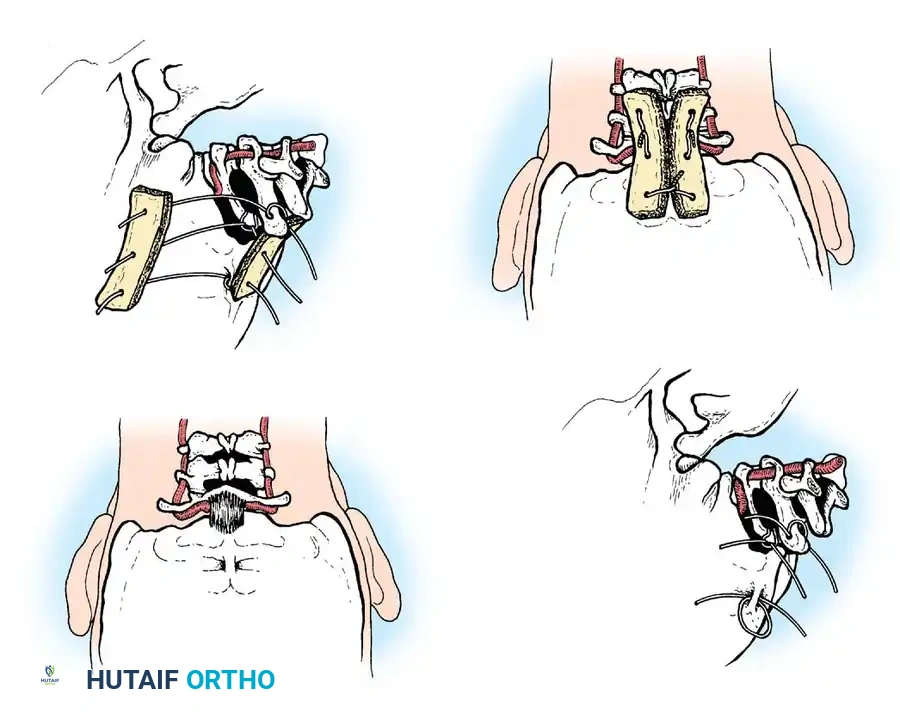
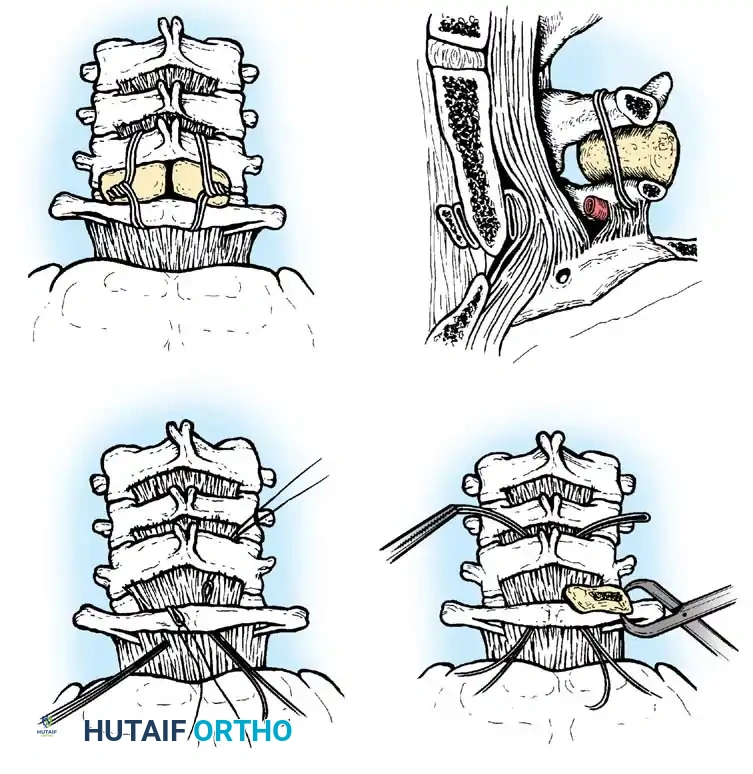
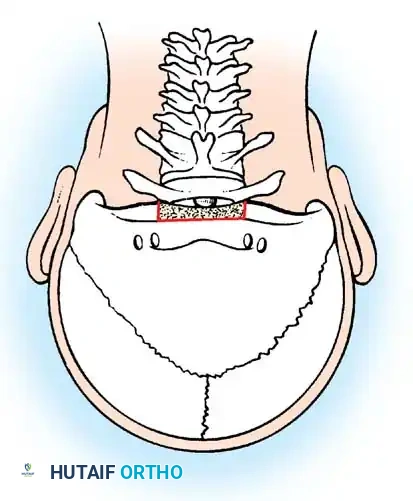
Before the advent of rigid screw fixation, sublaminar wiring techniques were the gold standard for C1-C2 arthrodesis. The structural integrity of the posterior arch of C1 must be verified via CT scan prior to utilizing these methods. The Gallie technique utilizes a single structural bone graft placed over the posterior arches of C1 and C2, secured with a single sublaminar wire passed beneath the arch of C1 and looped around the spinous process of C2. While this technique minimizes the risk of iatrogenic cord injury by requiring only one sublaminar passage, it is biomechanically inferior in controlling rotational forces. Furthermore, tightening the wire can cause the unstable C1 vertebra to translate posteriorly, potentially fusing the spine in a subluxated position.

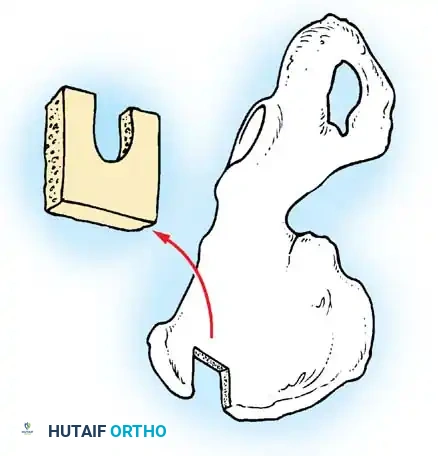
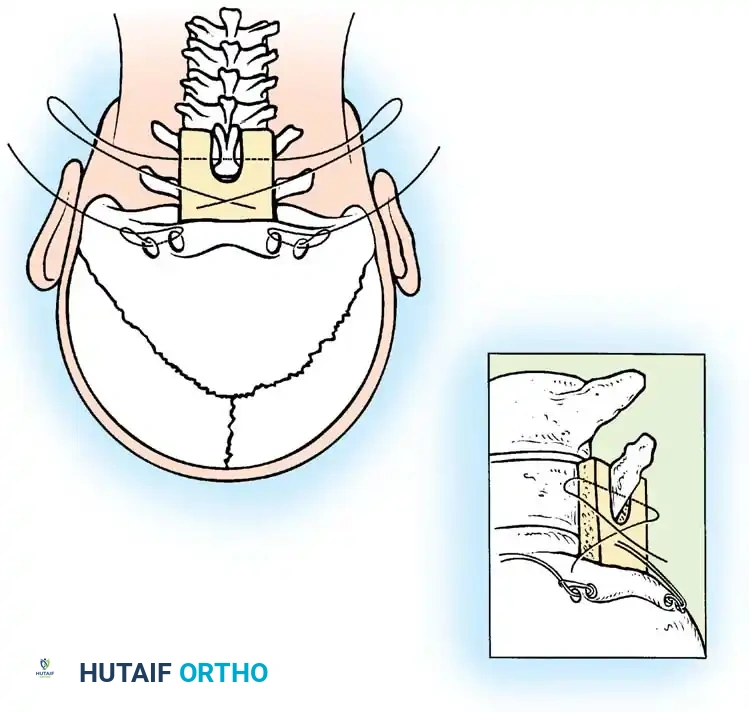
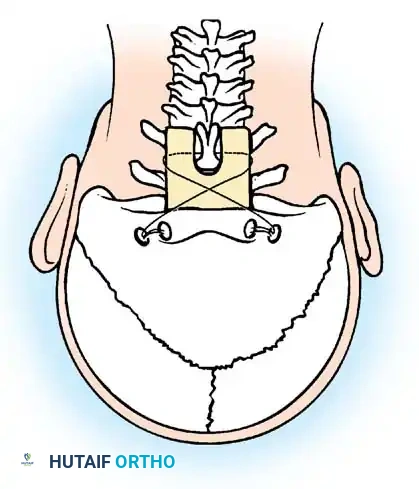
The Brooks-Jenkins technique provides superior biomechanical stability by utilizing two separate wedge-shaped bone grafts wedged between the lamina of C1 and C2. These grafts are secured by bilateral sublaminar wires passed beneath both C1 and C2.
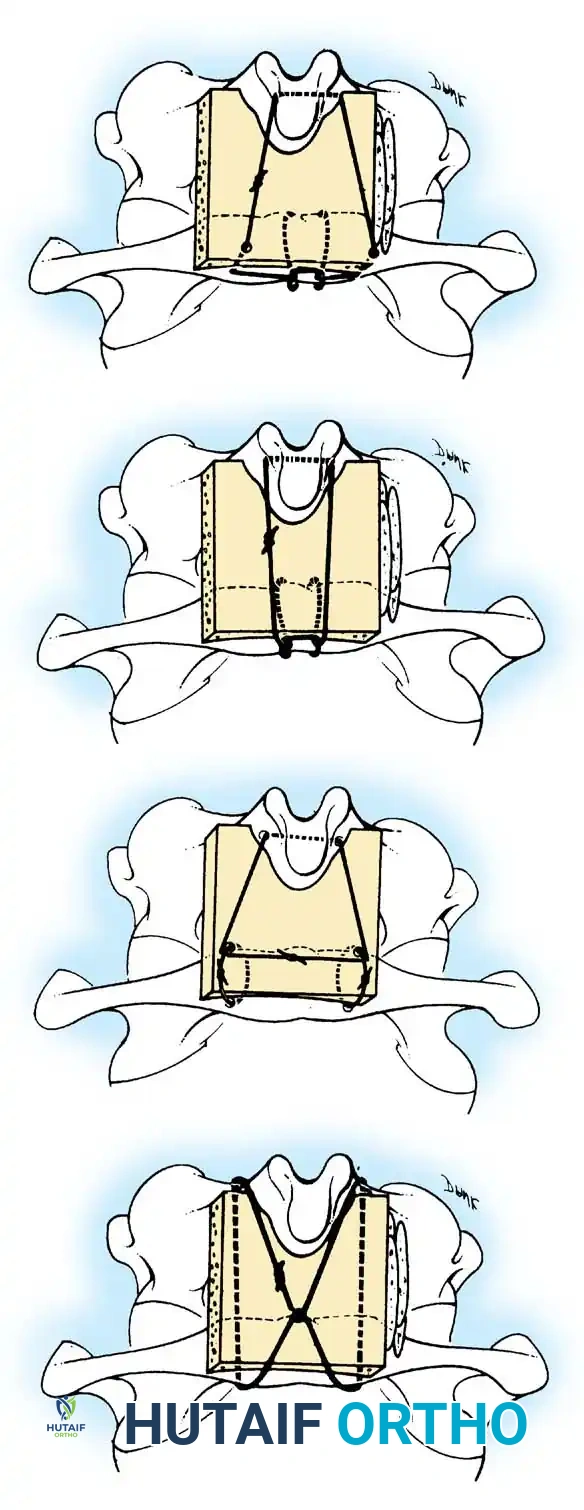
The preparation of the structural bone graft is critical; the grafts must be meticulously contoured to fit the specific anatomical dimensions of the interlaminar space, maximizing cortical contact for arthrodesis.
While the Brooks-Jenkins technique offers excellent resistance to rotational movement, lateral bending, and extension, it carries a higher risk profile. The passage of sublaminar wires beneath both C1 and C2 significantly increases the risk of dural tear or spinal cord contusion, especially in a pediatric spinal canal already compromised by instability and pannus formation.
Rigid Screw Fixation Techniques
Modern pediatric cervical spine surgery heavily favors rigid internal fixation utilizing the Harms and Goel techniques. This involves the placement of polyaxial screws into the lateral masses of C1 and the pedicles or pars interarticularis of C2, connected by bilateral titanium or cobalt-chrome rods. For C1 lateral mass screws, the C2 nerve root is mobilized inferiorly, and the entry point is identified at the junction of the C1 posterior arch and the midpoint of the lateral mass. The trajectory is strictly 10 to 15 degrees medial to avoid the vertebral artery, and aimed toward the anterior tubercle of C1 under lateral fluoroscopy.
For C2 pedicle screws, the entry point is in the cranial and lateral quadrant of the C2 isthmus. The trajectory is highly dependent on preoperative CT templating but is generally 20 to 30 degrees medial and 20 degrees cephalad. If a high-riding vertebral artery precludes safe pedicle screw placement, C2 pars screws or crossing translaminar screws provide excellent biomechanical alternatives with significantly reduced vascular risk. Following instrumentation, the C1-C2 facet joints are vigorously decorticated and packed with autologous cancellous bone graft to facilitate a robust arthrodesis.
Occipitocervical Fusion
When the posterior arch of C1 is assimilated, hypoplastic, absent, or fractured, isolated C1-C2 fusion is impossible. In these scenarios, or in cases of severe basilar invagination, the fusion construct must be extended proximally to the occiput. Historically, this was achieved using contoured rods or loops secured with sublaminar and cranial wiring, supplemented with massive autologous iliac crest bone graft.
Modern techniques favor rigid internal fixation using a midline or bilateral occipital plates secured with bicortical screws placed into the thickest portion of the occiput (the superior nuchal line), connected to cervical pedicle or lateral mass screws.
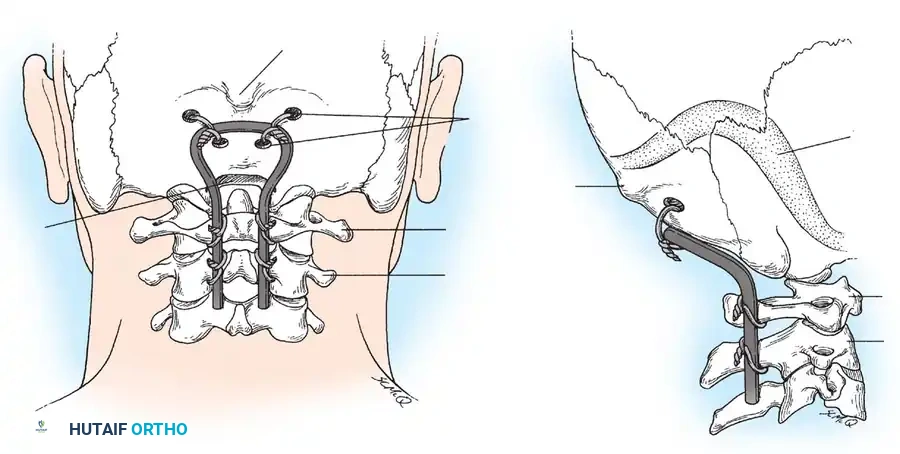
Regardless of the instrumentation used, meticulous decortication of the occiput and the posterior elements of the cervical spine, followed by the application of robust structural and cancellous autologous bone graft, is paramount for achieving long-term arthrodesis.
Anterior and Transoral Approaches
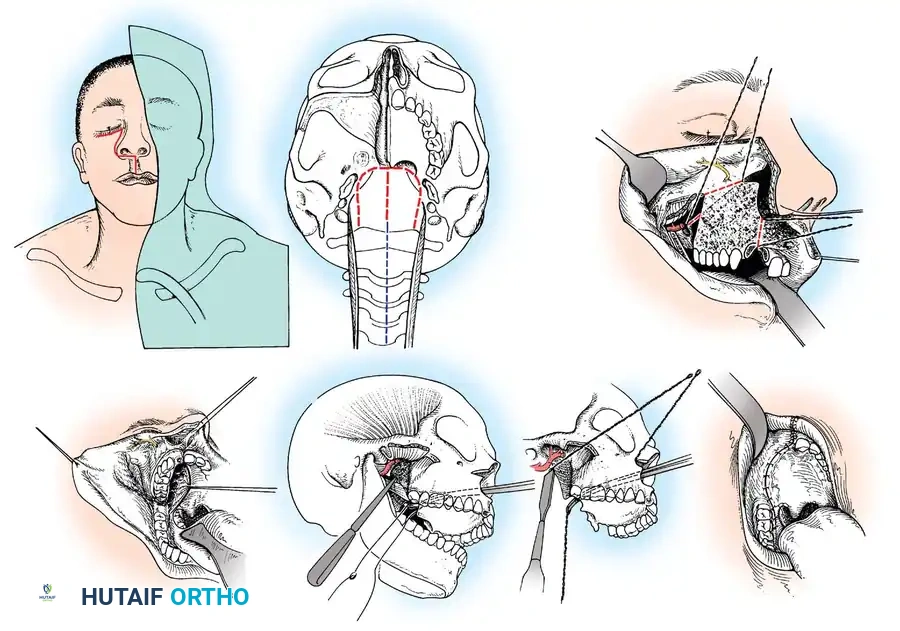
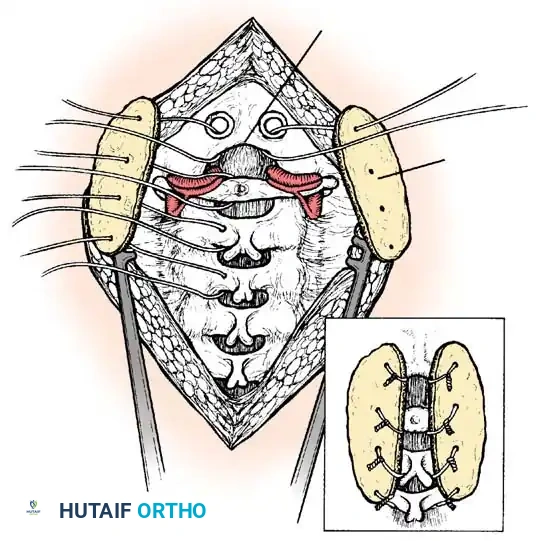
In rare instances, patients present with irreducible anterior spinal cord compression caused by a fixed, posteriorly displaced os odontoideum or a severely fibrotic retrodental pannus. An anterior decompressive approach—specifically the Transoral-Transpharyngeal Approach—is required to resect the anterior arch of C1 and the compressive odontoid/ossicle.
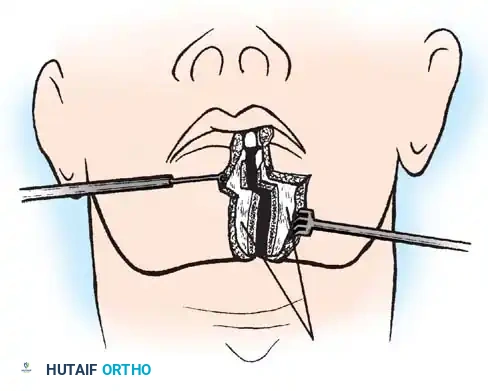
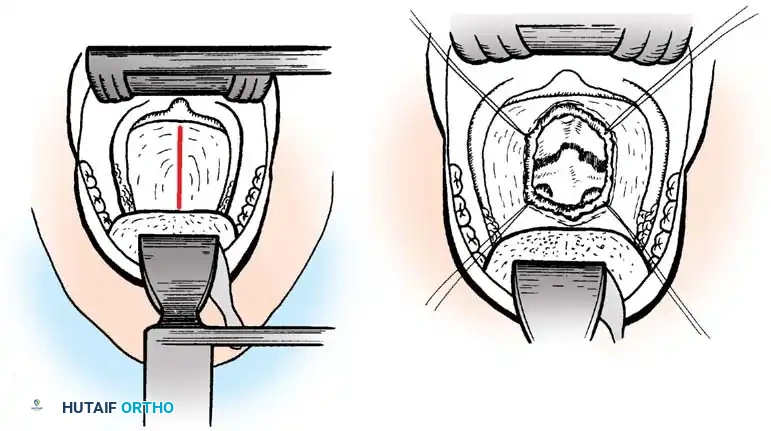
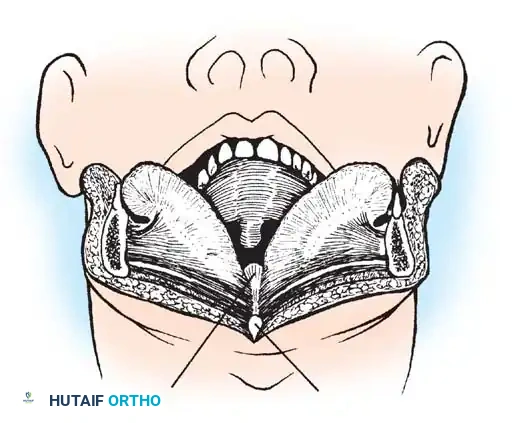
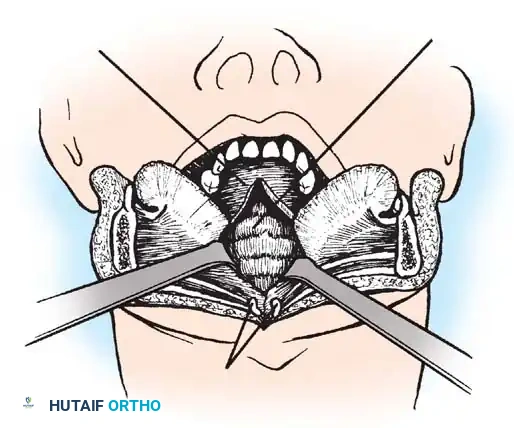
The patient is positioned supine, and a specialized transoral retractor is deployed to depress the tongue and elevate the soft palate. The posterior pharyngeal wall is incised vertically in the midline, exposing the anterior arch of C1 and the body of C2. A high-speed burr is utilized to resect the anterior arch of C1, providing access to the underlying odontoid pathology. The dens or os odontoideum is then carefully thinned with a diamond burr and removed using micro-curettes, directly decompressing the ventral dura. Because this procedure completely destroys the anterior stabilizing structures, it must invariably be followed by a staged posterior occipitocervical or C1-C2 stabilization.
Complications, Incidence Rates, and Salvage Management
Surgery of the pediatric craniovertebral junction is fraught with potential complications, owing to the diminutive osseous anatomy, the proximity of critical neurovascular structures, and the inherent challenges of achieving arthrodesis in a highly mobile segment. The surgeon must be intimately familiar with both the avoidance and the emergency management of these catastrophic events.
Vertebral artery injury (VAI) is the most feared intraoperative complication, with an incidence ranging from 1% to 4% in rigid C1-C2 screw fixation. VAI typically occurs during lateral exposure of the C1 arch, during drilling for C1 lateral mass screws, or due to medial breach during C2 pedicle screw placement. If a VAI occurs, immediate control of hemorrhage is paramount. This is usually achieved by rapid packing with hemostatic agents (e.g., Gelfoam, Surgicel) and applying direct pressure. If bleeding is controlled, the screw can sometimes be placed to tamponade the vessel
Clinical & Radiographic Imaging Archive