Congenital Upper Extremity Anomalies: Embryology and Transverse Deficiencies
Key Takeaway
The upper extremity develops between days 26 and 56 of gestation, governed by complex signaling centers including the apical ectodermal ridge and zone of polarizing activity. Disruptions in this embryological sequence can result in transverse deficiencies. Management requires a multidisciplinary approach, prioritizing early prosthetic fitting to match developmental milestones. Surgical interventions, such as the Krukenberg reconstruction, are reserved for specific functional indications, particularly in bilateral amputees with visual impairments.
Comprehensive Introduction and Patho-Epidemiology
The morphogenesis of the upper extremity is a highly orchestrated, spatiotemporally regulated process that begins early in the embryonic period, representing one of the most complex architectural achievements in human development. The upper extremity arises as a small bud of mesenchymal tissue on the lateral body wall beginning on day 26 of gestation. Notably, this precedes the formation of the lower extremity (leg bud) by approximately 24 hours, establishing a rigid cranial-to-caudal developmental gradient. Growth and differentiation proceed in a strict proximal-to-distal fashion, governed by three primary, highly conserved signaling centers that dictate the three-dimensional spatial orientation of the limb. The Apical Ectodermal Ridge (AER), located at the distal tip of the limb bud, is responsible for proximal-to-distal growth by secreting Fibroblast Growth Factors (FGFs) that maintain the underlying mesoderm in a highly proliferative state known as the progress zone. The Zone of Polarizing Activity (ZPA), situated in the posterior margin of the limb bud mesoderm, controls radioulnar (anterior-posterior) differentiation via the morphogen Sonic Hedgehog (SHH). Finally, the Wingless-Type (WNT) Signaling Center within the dorsal ectoderm secretes WNT-7a, inducing LMX1B expression to determine dorsal differentiation.
By day 31 of gestation, the hand paddle becomes morphologically distinct. Through a genetically programmed process of cellular apoptosis (programmed cell death) mediated by Bone Morphogenetic Proteins (BMPs), the fissuring of the hand paddle is completed by day 36. The central rays form first, followed rapidly by the preaxial and postaxial digits. The formation of chondral elements, endochondral ossification, and the subsequent development of joints, musculature, and vascular networks follow in rapid succession. The entire embryological formation of the upper extremity is completed by the end of the 8th week of gestation. Any disruption during this critical window results in congenital anomalies, broadly classified by the IFSSH (International Federation of Societies for Surgery of the Hand) based on the embryological failure mechanism.

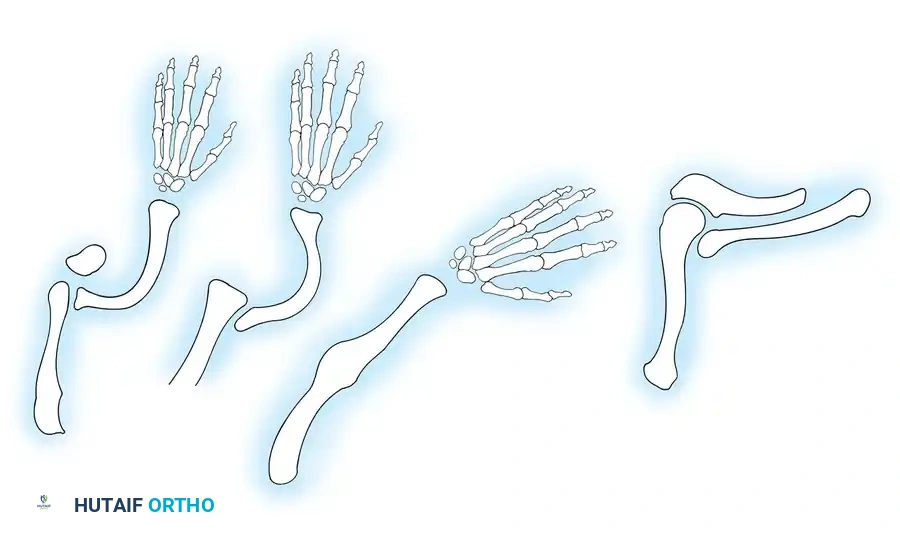
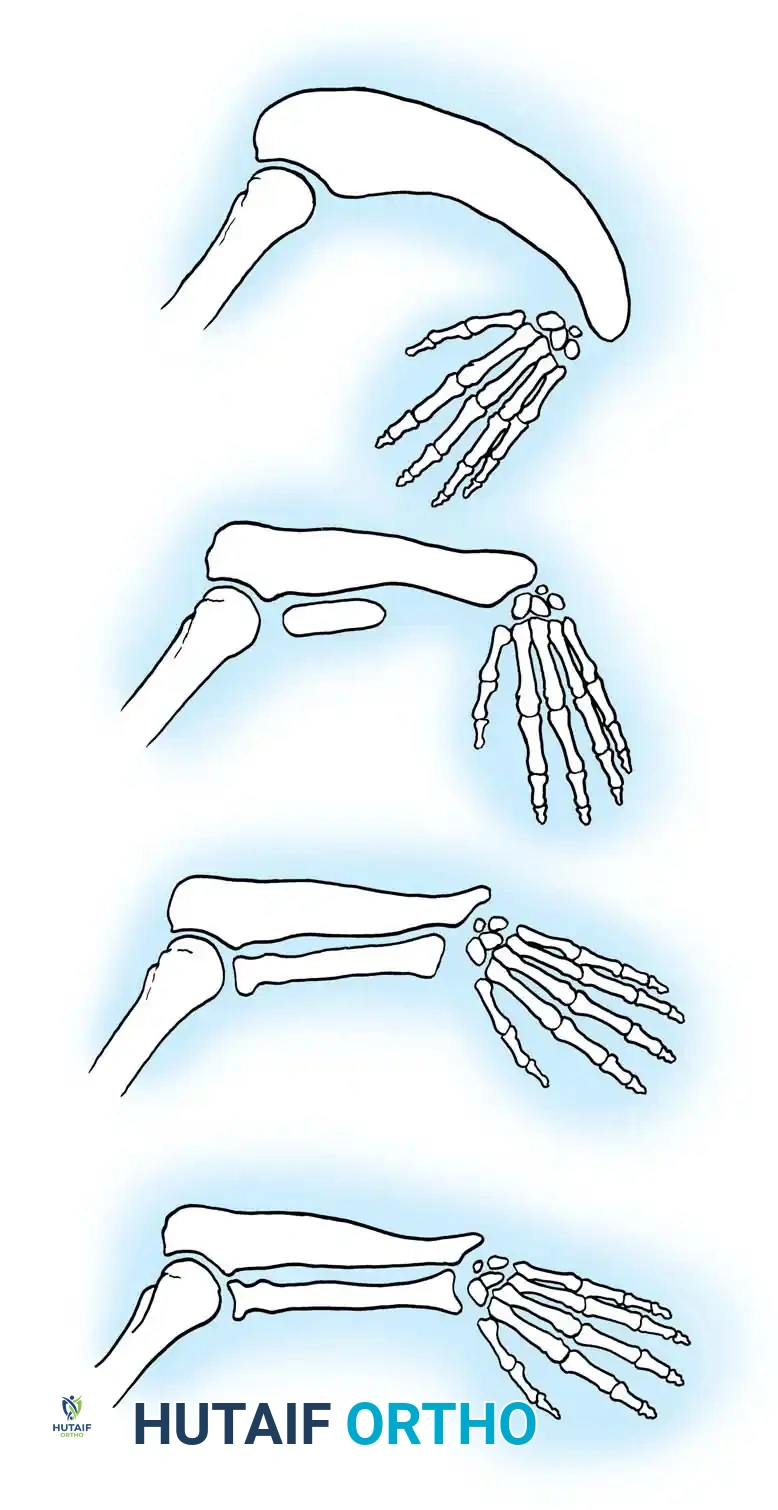
Transverse deficiencies represent a profound failure of formation characterized by the complete absence of parts distal to a specific point on the upper extremity, producing an amputation-like stump. Unlike longitudinal deficiencies (e.g., radial clubhand), where specific preaxial or postaxial rays are absent but distal elements remain, transverse deficiencies exhibit a complete transverse arrest of development. Classification is strictly anatomical, naming the level at which the remaining stump terminates (e.g., proximal third forearm deficiency, midcarpal deficiency). Wynne-Davies and Lamb reported the incidence of transverse deficiencies to be approximately 6.8 per 10,000 live births. The vast majority (98%) are unilateral, with the most common anatomical level being the upper third of the forearm. There is no established sex predilection, and the condition presents across all ethnicities with relatively uniform distribution.
The primary etiology is believed to be a failure or premature involution of the apical ectodermal ridge, likely secondary to an intrauterine vascular infarct, focal hypoxia, or mechanical disruption. Environmental and pharmacological factors have also been definitively implicated; for instance, the use of misoprostol (a prostaglandin E1 analogue) to induce abortion has been shown to cause profound vascular disruption in utero, leading to transverse deficiencies in surviving infants. In the standard unilateral transverse deficiency, there is no underlying genetic basis, and the recurrence risk for future pregnancies is negligible. However, rare bilateral or multiple transverse deficiencies may be inherited as an autosomal recessive trait or present as part of a broader syndromic constellation. These deficiencies have been reported in association with several malformation syndromes, including hydrocephalus, spina bifida, myelomeningocele, congenital talipes equinovarus (clubfoot), radial head dislocation, and radioulnar synostosis. Genetic counseling must therefore be meticulously tailored to distinguish between isolated unilateral sporadic events and syndromic or bilateral presentations.
Detailed Surgical Anatomy and Biomechanics
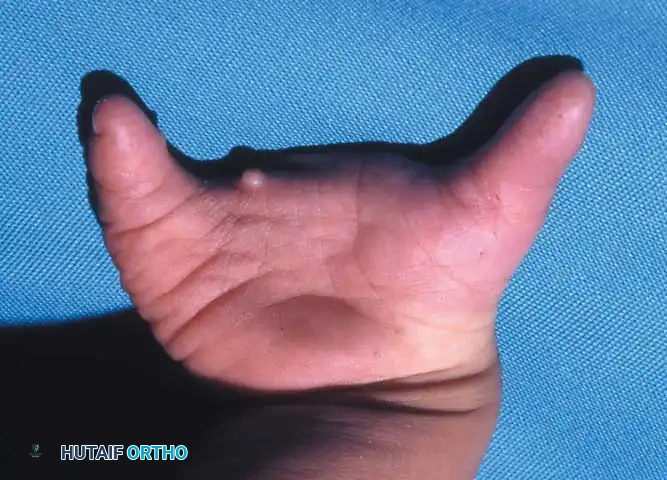
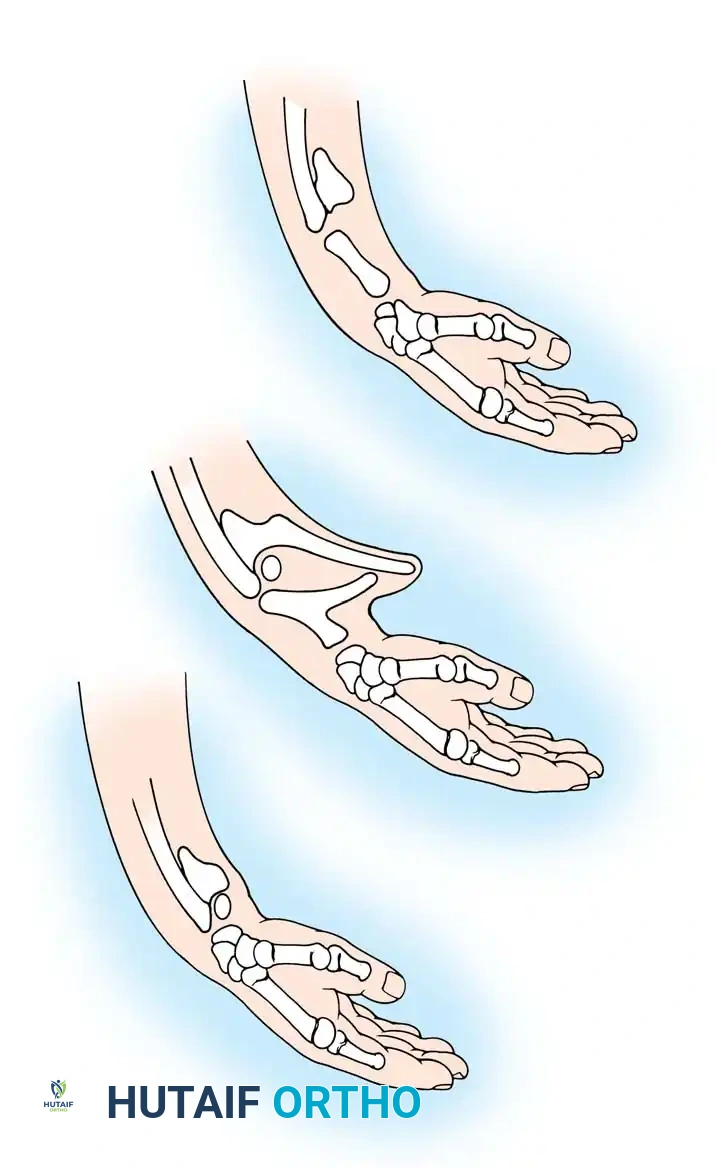
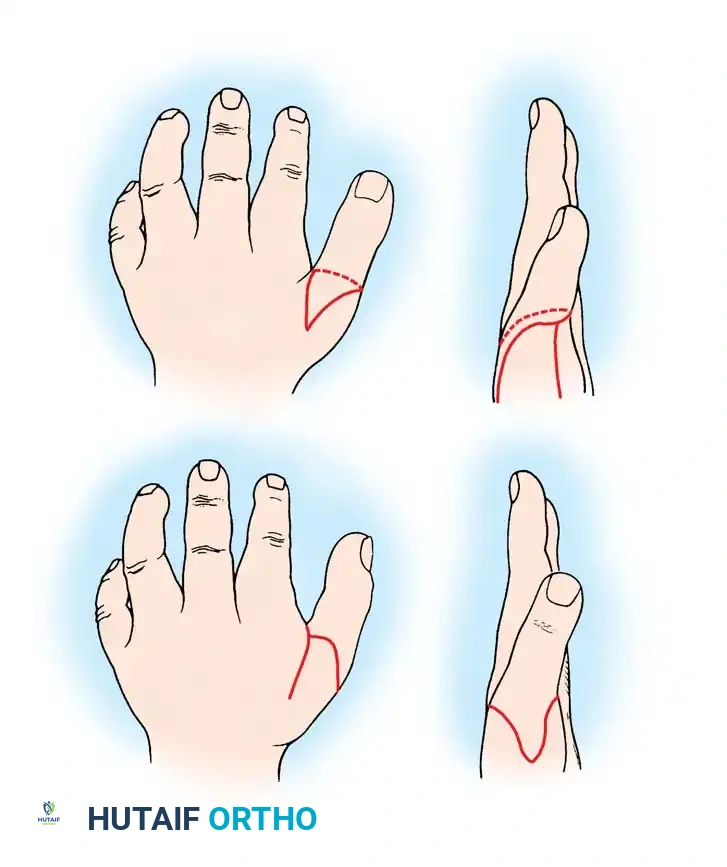
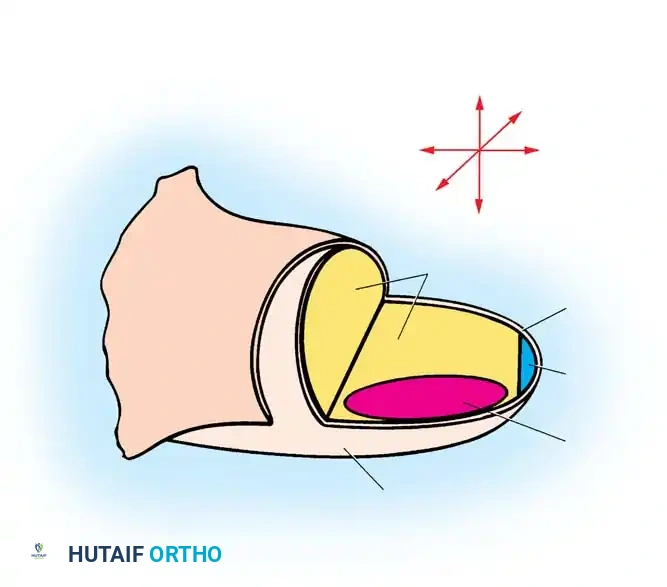
The surgical anatomy of a transverse deficiency is fundamentally distinct from that of a traumatic amputation, dictated entirely by the embryological timeline of the developmental arrest. In a true transverse deficiency, the residual limb typically presents as a slightly bulbous, well-padded stump. Because the arrest occurs during the mesenchymal condensation phase, the terminal bone ends are often rounded and capped with a robust cartilaginous or fibrous envelope, unlike the sharp, medullary-exposed bone ends seen in traumatic amputations. In more distal deficiencies, particularly at the carpal or metacarpal level, rudimentary, vestigial digital "nubbins" are frequently observed. These nubbins represent aborted attempts at digital ray formation and often contain tiny cartilaginous nodules, though they lack functional tendinous insertions or true articular joints.

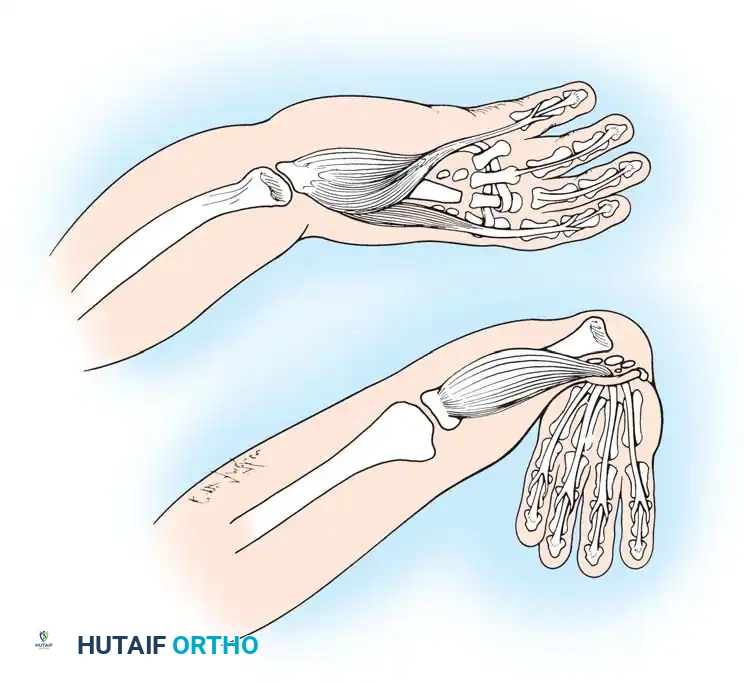
Hypoplasia of the more proximal musculature is a key clinical finding that helps differentiate true transverse deficiencies from amputations caused by congenital constriction band syndrome (amniotic band sequence). In amniotic band sequence, the proximal anatomy is typically entirely normal, as the amputation occurs mechanically after the limb has fully formed. Conversely, in a transverse deficiency, the lack of distal target organs leads to a failure of proximal muscle differentiation and bulk. In the most common presentation—the upper forearm amputation—the forearm is usually no more than 7 cm long at birth and will reach a maximum length of approximately 10 cm by skeletal maturity. The flexor and extensor muscle bellies of the forearm are rudimentary, often blending into a common aponeurotic mass over the distal end of the radius and ulna.

Biomechanically, the length of the residual limb dictates its functional capacity as a lever arm for prosthetic control. A short below-elbow stump provides limited surface area for socket suspension and a reduced mechanical advantage for elbow flexion against resistance. However, the preservation of the elbow joint is paramount, as it maintains spatial positioning of the terminal device. In midcarpal amputations (the second most frequent level), the rudimentary digital remnants are almost always nonfunctional, but the radiocarpal joint is preserved. This preservation is biomechanically invaluable; it allows for near-normal pronation and supination, as well as radiocarpal flexion and extension. This native motion provides a highly functional assisting limb that can trap objects against the body or the contralateral hand, often negating the need for a prosthesis entirely.
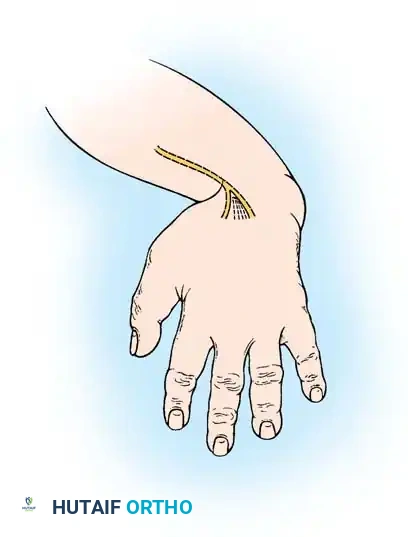
The neurovascular anatomy of the congenital stump also differs significantly from acquired amputations. Terminal neuromas, a frequent source of debilitating pain in traumatic amputees, are exceedingly rare in congenital transverse deficiencies. The peripheral nerves (median, ulnar, and radial) taper gracefully into the distal soft tissues without forming disorganized, hyperactive neural tangles. Vascularly, the major arteries often form an arborized network or a terminal plexus rather than a single abruptly ligated vessel. This unique neurovascular architecture provides excellent distal padding and robust sensory feedback, making the congenital stump highly sensate and resilient to the shear forces imposed by prosthetic sockets. Understanding this anatomy is critical when considering any surgical intervention, as preserving this native, sensate, pain-free envelope is the highest priority.
Exhaustive Indications and Contraindications
The overarching philosophy in the management of congenital transverse deficiencies is overwhelmingly non-operative. The cornerstone of care is early prosthetic fitting and occupational therapy. Surgical indications are exceedingly rare and must be approached with extreme caution, as ill-advised surgical interventions can easily downgrade a functional, pain-free residual limb into a painful, functionally inferior stump. However, there are specific, highly selected scenarios where surgical intervention is not only indicated but transformative for the patient's independence and quality of life.

Indications for surgery generally fall into three categories: optimizing the stump for prosthetic fitting, creating prehension in bilateral severe deficiencies, and addressing rare pathological complications. Stump optimization may involve the excision of redundant, flabby soft tissue that destabilizes a prosthetic socket, or the removal of prominent, non-functional digital nubbins if they are subject to recurrent trauma or impede prosthetic suspension. In cases of bilateral below-elbow deficiencies, particularly in children who are blind or visually impaired, the Krukenberg procedure is strongly indicated. This procedure separates the radius and ulna to create a sensate, pincer-like grasp, which is invaluable for patients who rely on tactile feedback for environmental navigation. More recently, Targeted Muscle Reinnervation (TMR) has emerged as an indication for older children and adolescents to create intuitive myoelectric control sites for advanced bionic prostheses.

Contraindications to surgery are far more numerous. The absolute contraindication is the performance of a Krukenberg procedure on a unilateral transverse deficiency; the cosmetic deformity is profound, and the functional gain is unnecessary given the presence of a normal contralateral limb. Another major contraindication is the amputation or "revision" of a sensate midcarpal or transcarpal stump simply to accommodate a standard prosthetic socket. The native tactile sensation and proprioception of a midcarpal stump are infinitely superior to any artificial terminal device. Sacrificing this tissue for the sake of cosmesis or easier prosthetic fitting is universally condemned in modern pediatric orthopedics. Furthermore, surgical interventions like bone lengthening (distraction osteogenesis) are relatively contraindicated in very short forearm stumps unless the predicted final length will significantly alter the class of prosthesis required (e.g., converting an above-elbow functional level to a below-elbow functional level).

Below is a comprehensive table detailing the clinical decision-making matrix for surgical and prosthetic interventions in transverse deficiencies.
| Intervention Type | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Krukenberg Procedure | Bilateral below-elbow deficiency; Bilateral deficiency with blindness | Unilateral transverse deficiency; Proximal radioulnar synostosis | Lack of psychological readiness; Poor family support |
| Targeted Muscle Reinnervation (TMR) | High-level amputations requiring multiple myoelectric signals | Severe proximal muscle hypoplasia; Cognitive inability to train | Very young age (typically deferred until adolescence) |
| Distraction Osteogenesis | Extremely short forearm stump failing prosthetic suspension | Active infection; Severe soft tissue scarring | Anticipated length gain < 3 cm; Non-compliant family |
| Digital Nubbin Excision | Recurrent trauma/ulceration; Interference with prosthetic socket | Stable, asymptomatic nubbins; Nubbins providing tactile feedback | Mild cosmetic concerns without functional deficit |
| Midcarpal Amputation Revision | Never indicated for purely cosmetic reasons | Amputation to fit standard below-elbow prosthesis | Any procedure sacrificing native terminal sensibility |
Pre-Operative Planning, Templating, and Patient Positioning
While true "pre-operative" planning is rare due to the non-operative nature of most cases, the rigorous evaluation required for prosthetic staging or the rare surgical intervention demands a meticulous, multidisciplinary approach. Clinical evaluation begins with a comprehensive assessment of the residual limb. The surgeon must evaluate the soft tissue envelope for mobility, padding, and the presence of any rudimentary digits. Range of motion of the proximal joints—specifically the shoulder and elbow—must be documented, as congenital anomalies frequently present with associated joint contractures or dysplasias. For example, a short below-elbow deficiency may be complicated by a congenital radial head dislocation or radioulnar synostosis, which drastically limits the functional workspace of the limb and alters the prosthetic prescription.
Radiographic evaluation is mandatory to define the exact skeletal anatomy. Standard orthogonal views (anteroposterior and lateral) of the residual limb and proximal joints are obtained. In infants, the lack of ossification centers can make interpretation challenging; ultrasound or MRI may be utilized if surgical intervention is contemplated early, though this is rarely necessary. If distraction osteogenesis is planned for a short forearm segment, precise templating is required to determine the size of the external fixator, the safe corridors for pin placement (avoiding the rudimentary neurovascular bundles), and the optimal site for the corticotomy. The surgeon must calculate the desired length gain, keeping in mind that the soft tissue envelope in congenital deficiencies is often less compliant than in acquired conditions.
For the rare surgical interventions, patient positioning follows standard pediatric upper extremity protocols. The patient is positioned supine with the affected limb extended on a radiolucent hand table. A pneumatic tourniquet is universally applied to the proximal arm to ensure a bloodless surgical field, which is critical for identifying the often aberrant neurovascular structures associated with congenital anomalies. In pediatric patients, strict attention must be paid to tourniquet pressures (typically 50-75 mmHg above systolic blood pressure) and inflation times to prevent ischemic injury to the already hypoplastic musculature.
Furthermore, pre-operative planning extends heavily into the psychological and developmental domains. The surgical team must work intimately with pediatric psychologists, prosthetists, and occupational therapists. If a Krukenberg procedure is planned, intensive pre-operative counseling is required to prepare the family and the child for the dramatic cosmetic alteration of the limb. The family must understand that the goal is purely functional—creating a sensate prehensile pincer—and that the resulting limb will look distinctly non-anatomical. Managing these expectations is as critical to the success of the procedure as the surgical execution itself.
Step-by-Step Surgical Approach and Fixation Technique
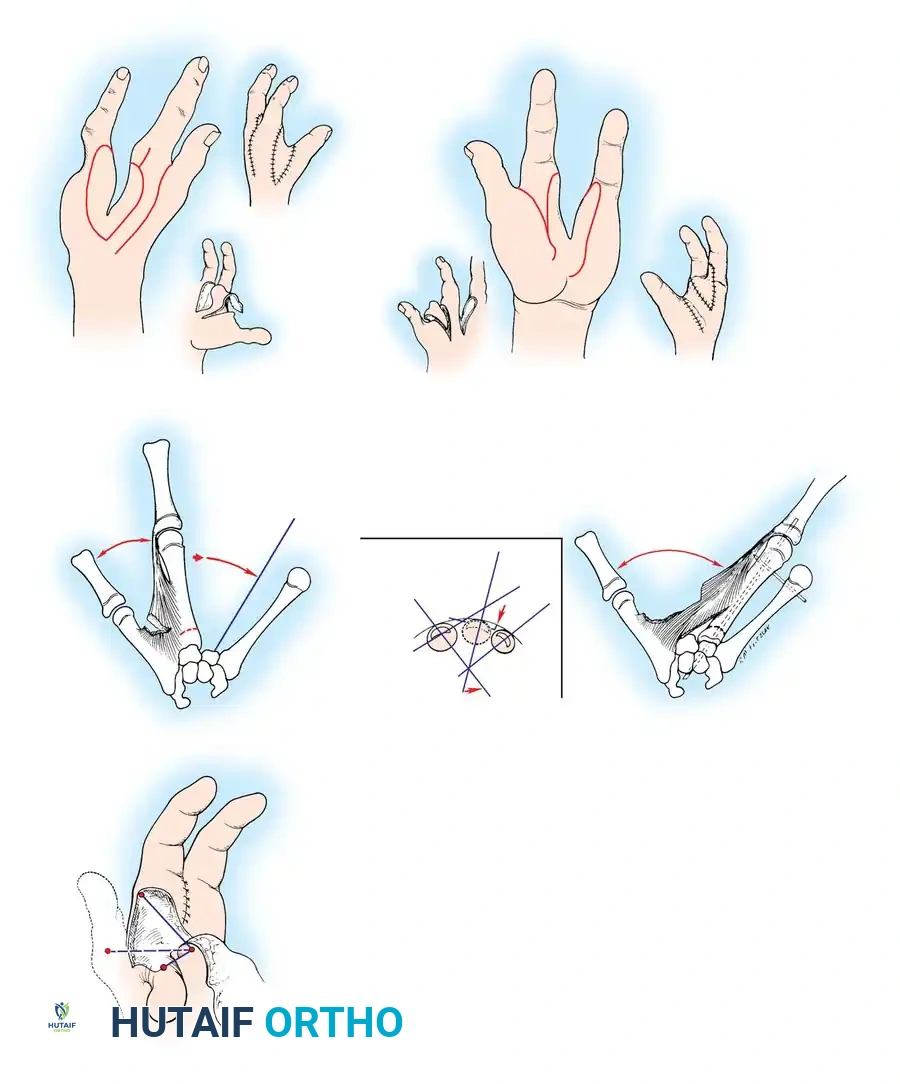
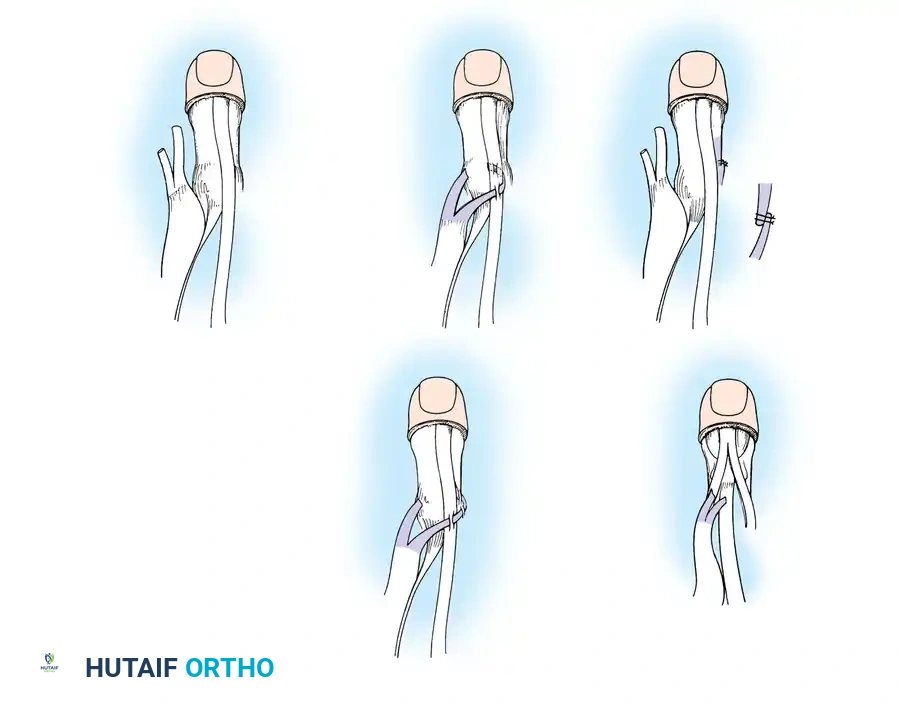
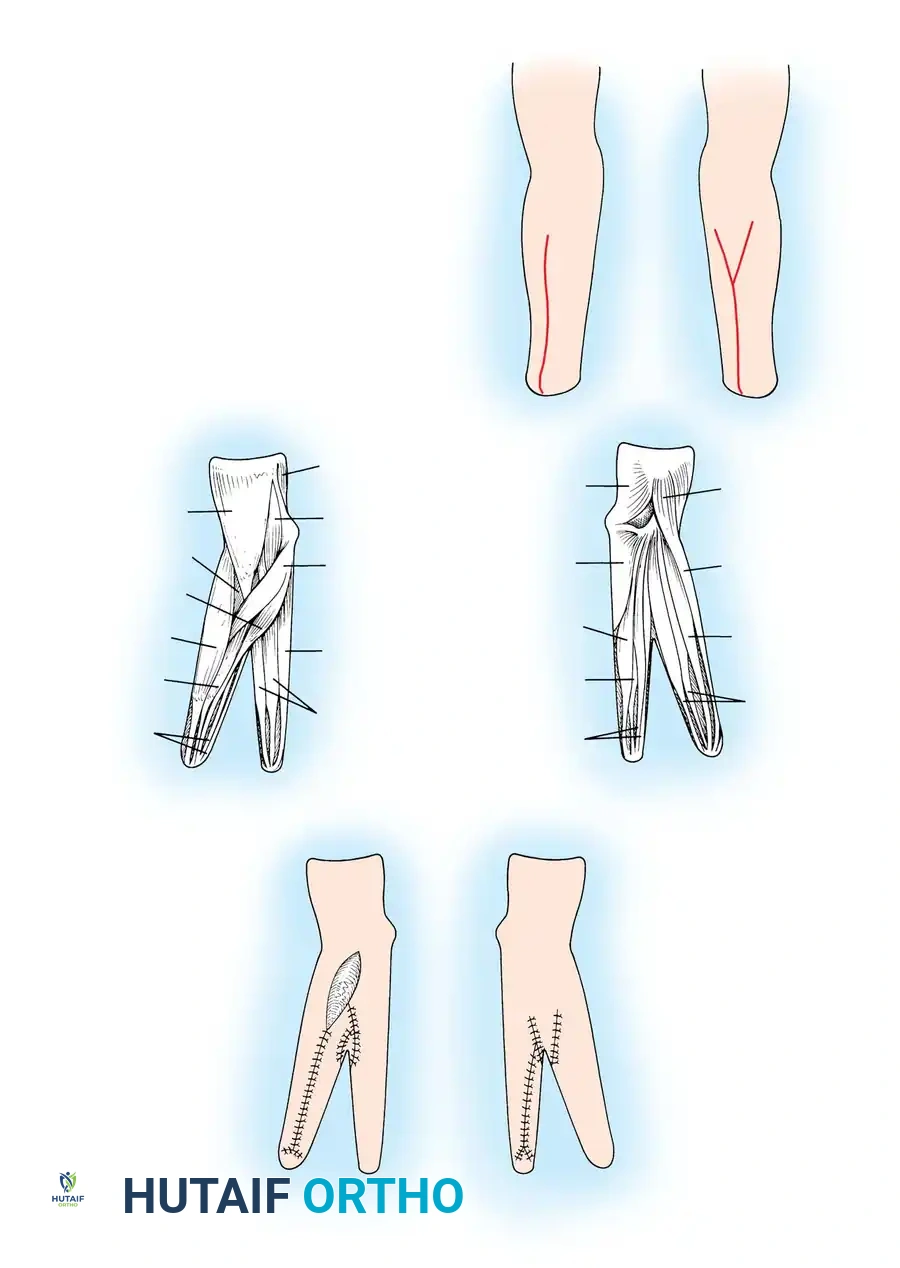
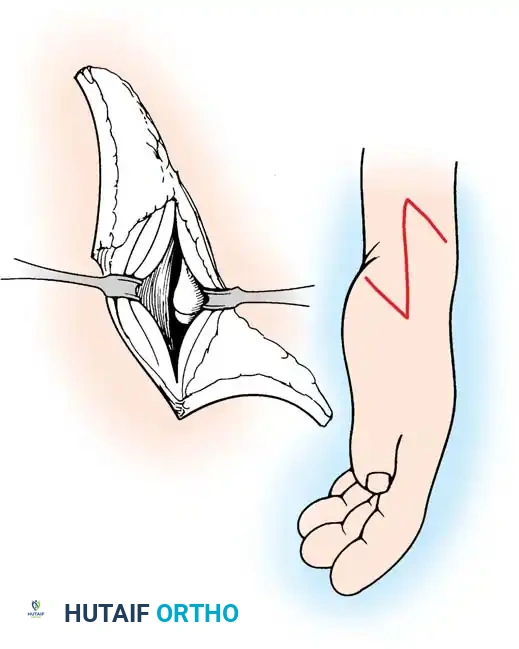
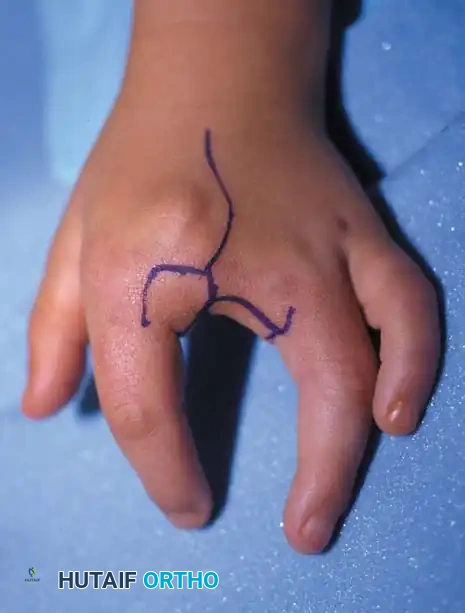
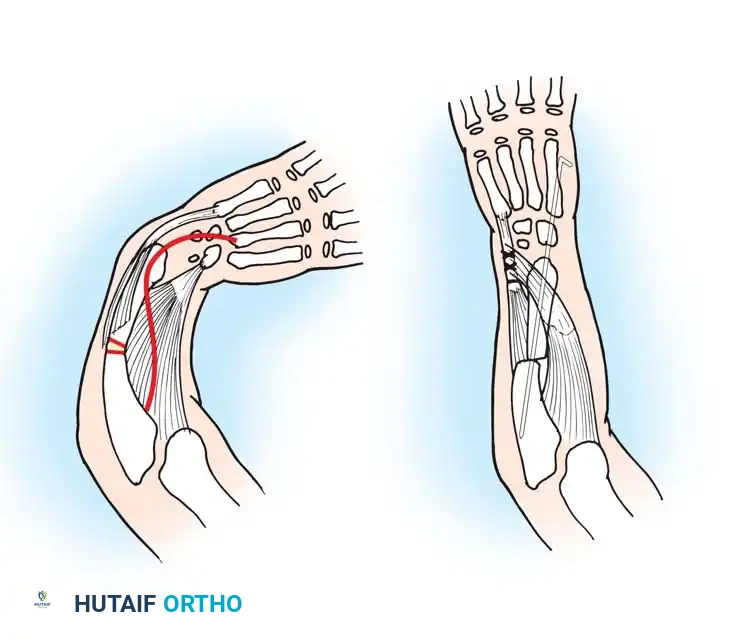
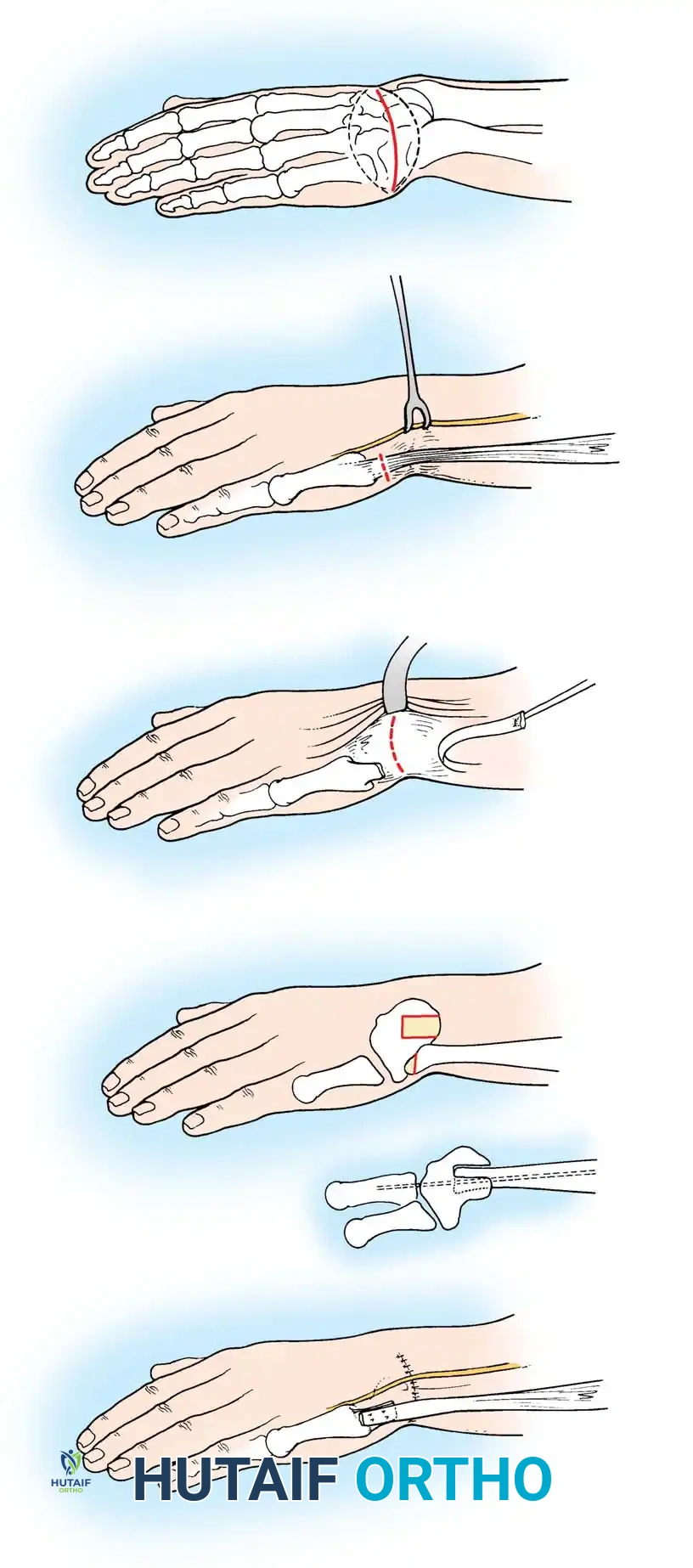
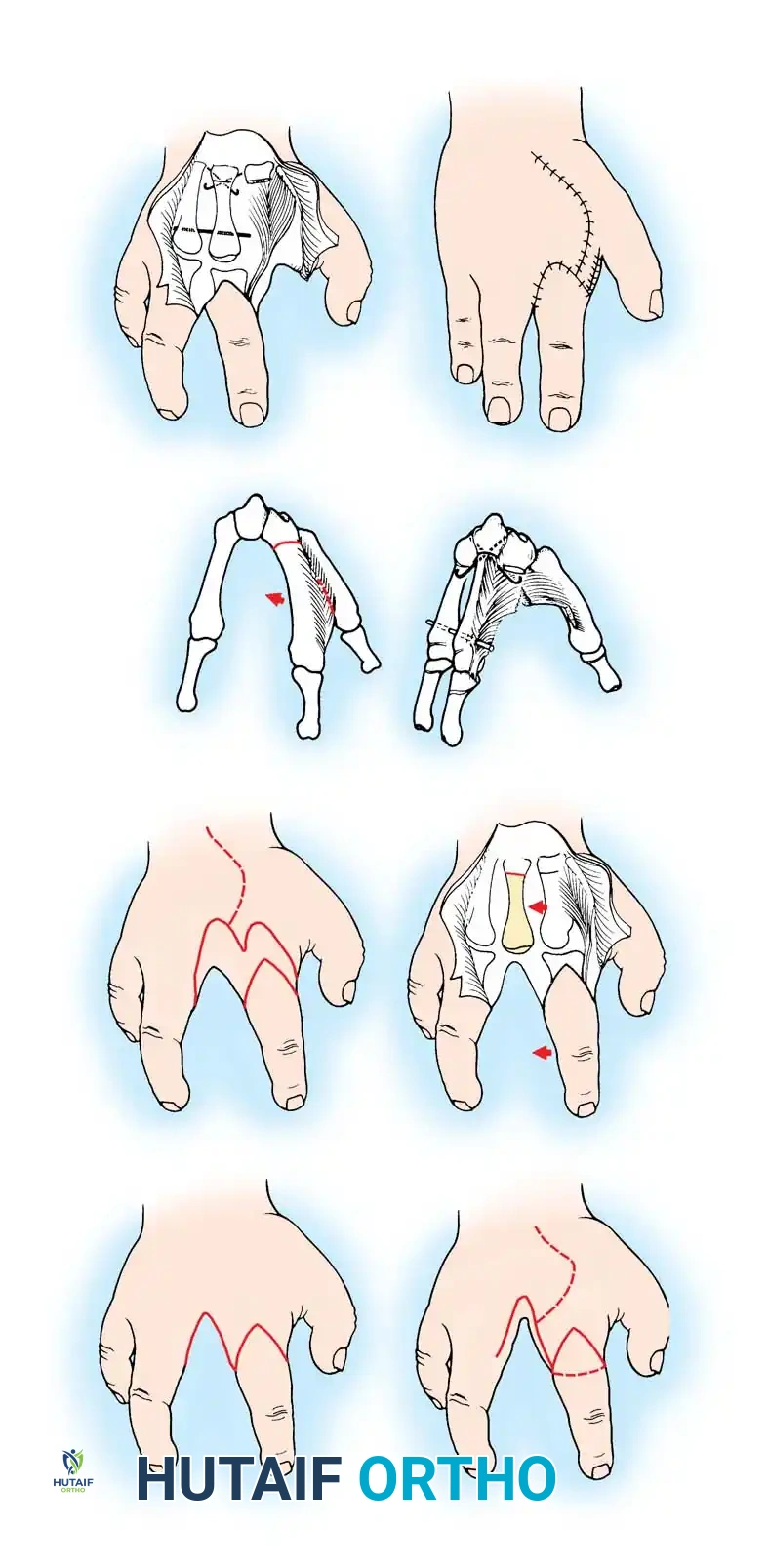
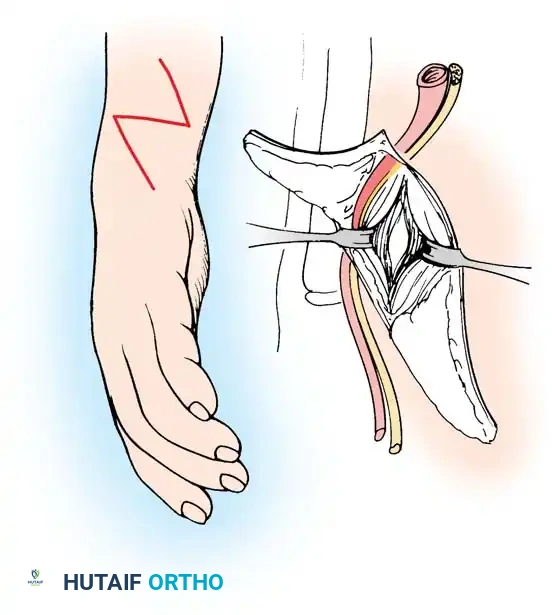
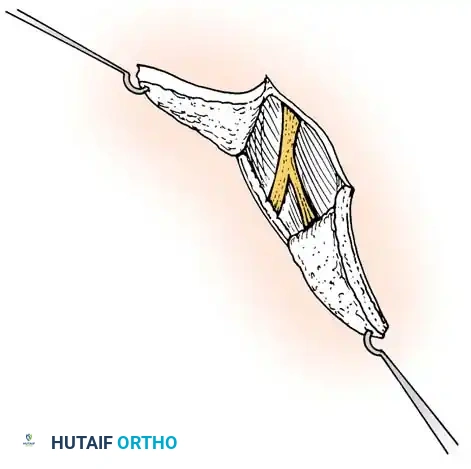
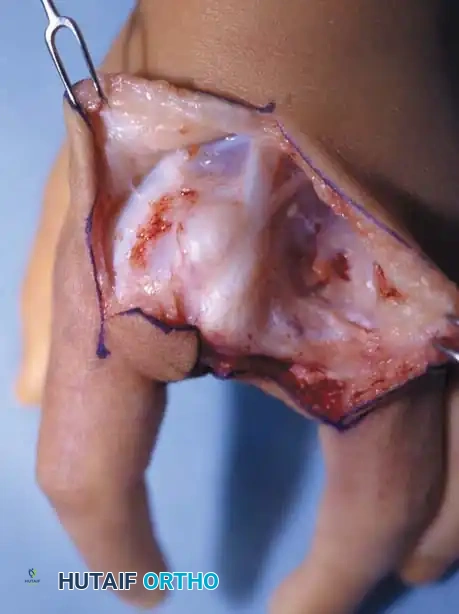
When surgical intervention is deemed absolutely necessary, the techniques employed require meticulous handling of the unique congenital soft tissue envelope. The Krukenberg procedure remains the most historically significant and functionally transformative operation for bilateral below-elbow deficiencies. The goal is to convert the forearm into a sensate forceps by separating the radius and ulna. The surgical approach begins with a longitudinal incision on the volar aspect of the forearm, curving distally over the stump, and continuing proximally on the dorsal aspect. The skin flaps must be elevated with robust subcutaneous fat to ensure viability.

The deep dissection involves identifying and separating the flexor and extensor muscle masses. The pronator teres is preserved if possible, as it provides powerful active closure of the radial and ulnar "prongs." The interosseous membrane is incised longitudinally from distal to proximal, taking extreme care to identify and ligate the anterior and posterior interosseous vessels to prevent catastrophic hematoma. The median nerve is typically routed with the radial prong to provide sensation to the opposing surface, while the ulnar nerve remains with the ulnar prong. Once the radius and ulna are separated, the muscle bellies are wrapped around their respective bones to provide padding. The most challenging aspect is skin closure; the opposing surfaces of the radius and ulna must be covered with sensate, full-thickness skin. This often requires complex local tissue rearrangement, Z-plasties, or full-thickness skin grafting for the lateral, non-contact surfaces.

In the modern era, Targeted Muscle Reinnervation (TMR) is increasingly utilized in the pediatric congenital population to optimize myoelectric prosthetic control. The surgical technique involves identifying the terminal branches of the major peripheral nerves (median, ulnar, radial) within the stump. These nerves, which in a congenital anomaly taper into the distal soft tissue, are carefully dissected proximally. The surgeon then identifies redundant or expendable muscle bellies within the hypoplastic forearm mass. The native motor nerve to the target muscle is transected, and the terminal stump nerve is coapted to the target muscle's motor entry point using microsurgical techniques (typically 9-0 or 10-0 epineurial sutures and fibrin glue). Over several months, the nerve reinnervates the muscle, creating an amplified electromyographic (EMG) signal that can be detected by surface electrodes in the prosthetic socket, allowing for intuitive control of a bionic hand.

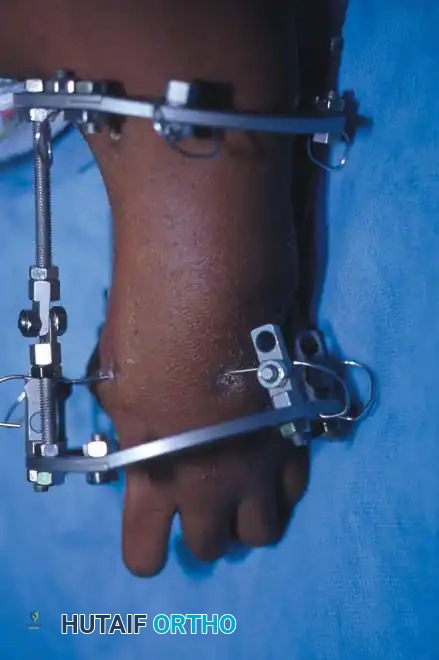
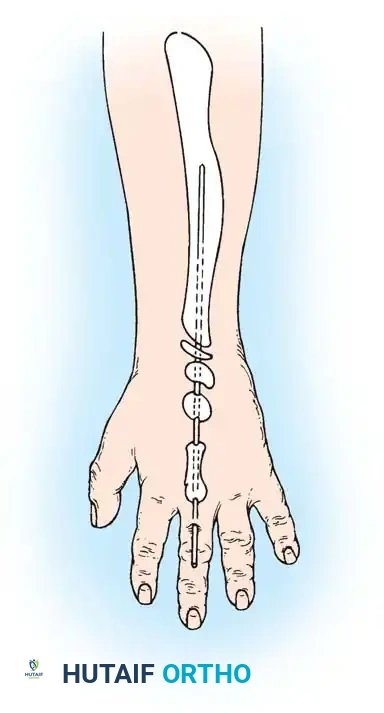
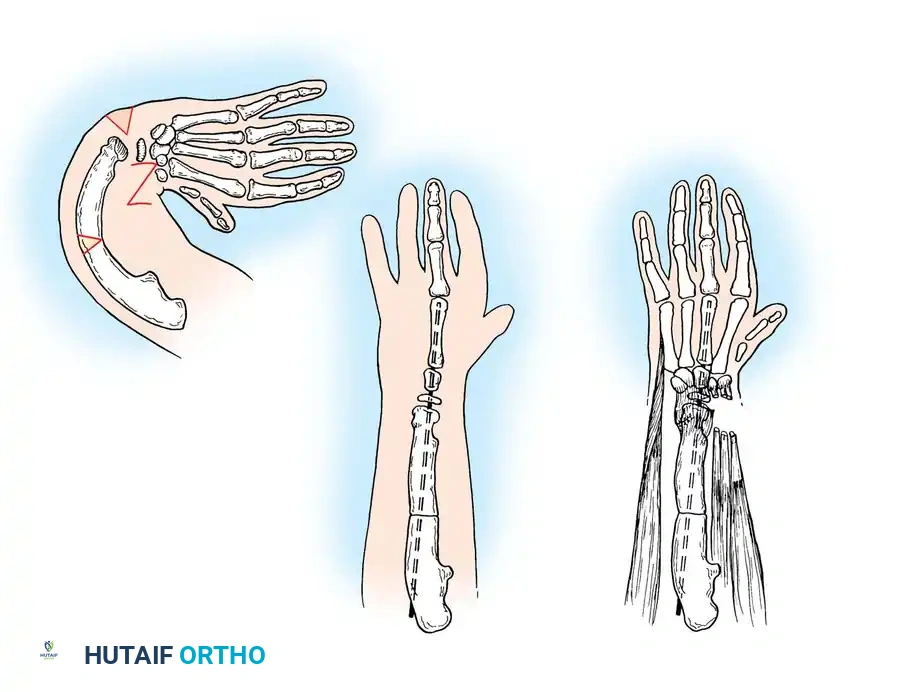
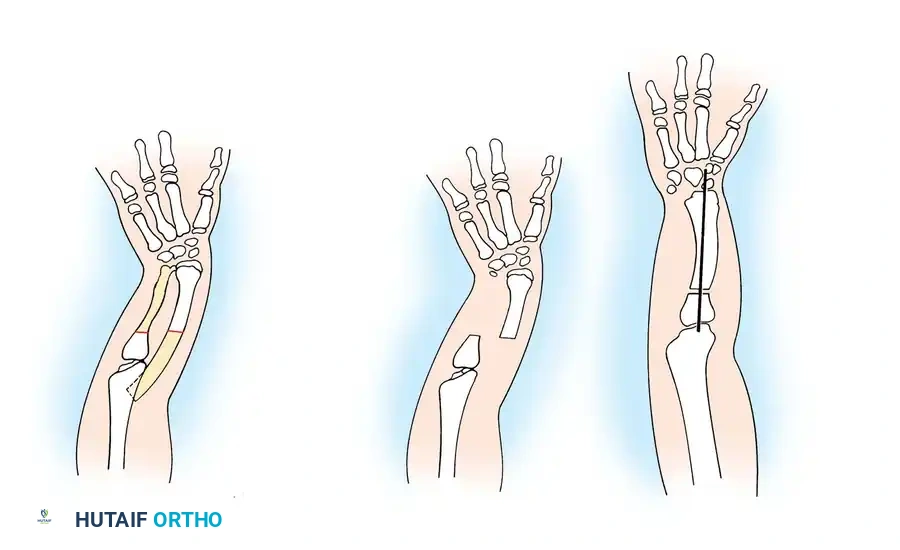
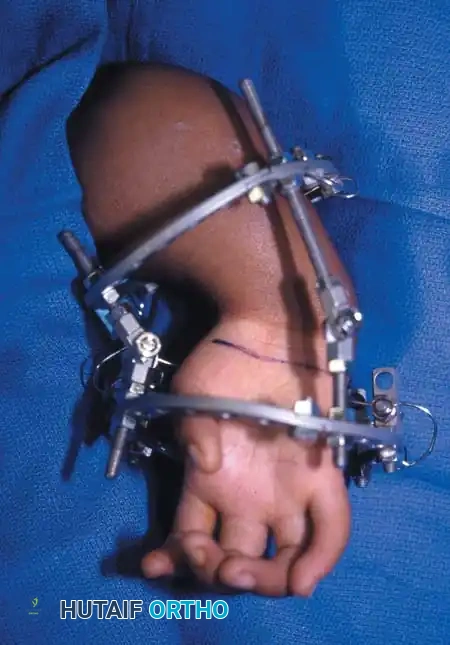
For distraction osteogenesis in severe short below-elbow deficiencies, the surgical approach relies on minimally invasive principles to preserve the periosteal blood supply. A unilateral or circular external fixator is applied using half-pins or fine wires. Pin placement must be confirmed fluoroscopically to ensure bicortical purchase while avoiding the distal physis (if present) and the neurovascular bundles. A percutaneous or mini-open corticotomy is performed using a drill-hole technique and an osteotome, avoiding the use of a power saw to prevent thermal necrosis. After a latency period of 5 to 7 days, distraction is initiated at a rate of 0.75 to 1.0 mm per day, divided into three or four increments. The consolidation phase typically requires twice the duration of the distraction phase. Rigid fixation must be maintained until continuous cortical bone is visible on at least three of four cortices on orthogonal radiographs.
Complications, Incidence Rates, and Salvage Management
Complications in the management of congenital transverse deficiencies arise primarily from prosthetic interface issues, as surgical interventions are rare. However, when surgery is performed, the complication profile is unique to the pediatric and congenital population. Non-operative complications center around prosthesis rejection, which is highly prevalent in unilateral cases if fitting is delayed beyond the age of 2 years. Children rapidly develop unilateral compensatory strategies, and a late-fitted prosthesis is often viewed as a heavy, insensate hindrance rather than an aid. Skin breakdown, contact dermatitis, and allergic reactions to socket materials (e.g., plastisol, silicone) occur in approximately 15-20% of prosthetic users and require immediate modification of the socket interface and dermatological management.
Surgical complications, though rare, can be severe. Terminal bone overgrowth, a notorious complication in pediatric traumatic amputations where the appositional bone growth outpaces the soft tissue envelope, is paradoxically less common in true congenital transverse deficiencies. Because the congenital stump is capped with a thick cartilaginous envelope, the bone rarely spikes through the skin. However, if a surgical revision or bone cut is made (e.g., during a Krukenberg procedure or shortening), the risk of terminal overgrowth skyrockets to nearly 30% in children under 12. Management of overgrowth requires surgical revision, often utilizing a synthetic cap (e.g., silicone or UHMWPE) or an autologous osteocartilaginous graft (e.g., from the iliac crest or fibula) to seal the medullary canal and halt the appositional spiking.
In distraction osteogenesis, complications are frequent and demand vigilant postoperative care. Pin tract infections occur in up to 40% of patients and are usually managed with oral antibiotics and local pin care. More severe complications include premature consolidation of the regenerate bone (requiring re-corticotomy), delayed union or non-union (requiring bone grafting and prolonged fixation), and axial deviation of the lengthened segment. Furthermore, the soft tissue envelope may resist lengthening, leading to flexion contractures of the elbow or wrist, necessitating aggressive physical therapy or surgical release.

Below is a summary table of common complications, their incidence, and salvage strategies.
| Complication | Estimated Incidence | Etiology/Risk Factors | Salvage Management & Prevention |
|---|---|---|---|
| Prosthesis Rejection | 30-50% (Unilateral) | Late fitting (>2 years); Heavy myoelectric devices in toddlers | Early fitting protocol (3-6 months); Emphasize lightweight passive devices initially |
| Contact Dermatitis / Skin Breakdown | 15-20% | Poor socket fit; Hyperhidrosis; Material allergy | Socket modification; Silicone liners; Topical corticosteroids; Temporary cessation of wear |
| Terminal Bone Overgrowth | <5% (Native); ~30% (Post-surgical) | Surgical transection of diaphyseal bone in growing child | Autologous capping (epiphyseal transfer); Synthetic capping; Revision amputation |
| Pin Tract Infection (During Lengthening) | 30-40% | Inadequate pin care; High soft tissue tension | Oral antibiotics; Chlorhexidine pin care; Rarely requires pin removal |
| Premature Consolidation | 5-10% | Slow distraction rate; Highly osteogenic pediatric periosteum | Surgical re-corticotomy; Adjust distraction protocol |
Phased Post-Operative Rehabilitation Protocols
In the context of congenital transverse deficiencies, "rehabilitation" is synonymous with the lifelong, phased integration of prosthetics and adaptive occupational therapy. The protocol is strictly governed by the child's natural neurodevelopmental milestones. A child’s manual and bimanual skills develop in a predictable, orderly sequence, and prosthetic fitting must complement, rather than obstruct, this timeline. The multidisciplinary clinic—comprising the orthopedic surgeon, prosthetist, occupational therapist, and social worker—must evaluate the child regularly to graduate the prosthetic complexity in tandem with cognitive and motor development.
Phase 1: Birth to 9 Months (The "Sit to Fit" Stage)
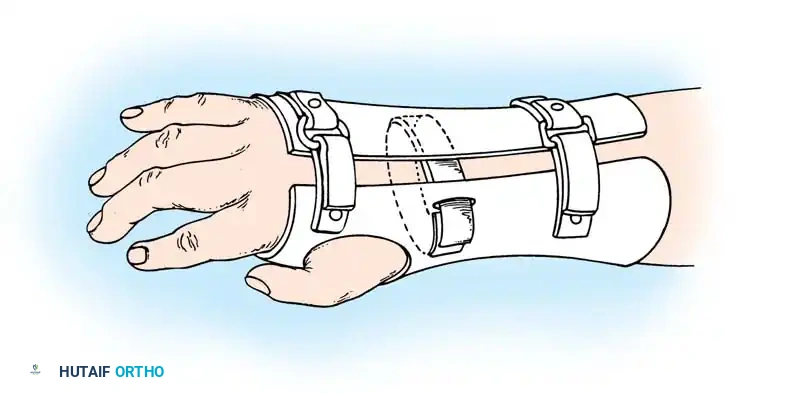
During the first six months of life, prehension is achieved primarily via bilateral palmar grasp, and the child is developing core stability. The prosthetic protocol dictates that a passive plastic mitten prosthesis is introduced once the child achieves independent sitting balance (typically between 3 to 6 months). This is the critical window for incorporating the prosthesis into the child's developing body image. The passive mitten provides a stable surface for sitting, assists in crawling, and allows the child to pull to a stand. At this stage, the prosthesis is lightweight and purely for gross bimanual stabilization and spatial awareness.
Phase 2: 12 to 18 Months (Active Terminal Devices)
Between 12 and 18 months, a child's cognitive capacity evolves to understand cause and effect, and single-hand grasp develops, followed by thumb-to-finger pinch. Notably, the cognitive ability to grasp precedes the voluntary ability to release. At this stage, the passive mitten is exchanged for an actively opened, plastisol-covered split hook or a Child Amputee Prosthetic Program (CAPP) terminal device. The device is operated via a figure-of-eight harness linked to contralateral shoulder biscapular abduction. Occupational therapy is intensive during this phase, focusing on training the child to use the harness to open the device, grasp large objects, and voluntarily release them.
Phase 3: 2 to 4 Years (Myoelectric Integration)
As the child reaches preschool age (2 to 4 years), a myoelectric prosthesis may be considered. Studies have shown these devices to be highly useful and appropriate for young children, offering superior cosmesis and intuitive grip control without the restrictive harnessing required for body-powered devices. The occupational therapist uses biofeedback games to train the child to isolate the flexor and extensor muscle groups in the residual limb to generate reliable EMG signals. The transition to a myoelectric device requires significant family commitment, as the devices are heavier, require daily charging, and need frequent socket adjustments as the child grows.
Phase 4: School Age and Beyond (Specialized Adaptations)
For children aged 5 and older, the focus shifts to independence in activities of daily living (
Clinical & Radiographic Imaging Archive