Mastering Intra-articular Scapular Fracture Fixation: A Real-Time Operative Guide

Key Takeaway
This masterclass details open reduction and internal fixation of intra-articular scapular fractures. We'll cover comprehensive surgical anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative execution from the surgeon's viewpoint. Expect extensive pearls, pitfalls, and post-operative rehabilitation protocols. This guide is designed for fellows to master complex glenoid fracture management.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we are tackling one of the most formidable challenges in orthopedic trauma: the intra-articular scapular fracture. These injuries represent a unique intersection of complex three-dimensional anatomy, demanding surgical exposures, and unforgiving biomechanical requirements. Scapular fractures as a whole are relatively rare, comprising approximately 0.4% to 1% of all fractures and 3% to 5% of shoulder girdle injuries. However, intra-articular variants—specifically those involving the glenoid fossa and glenoid rim—account for roughly 10% of these cases and carry a disproportionately high risk of long-term morbidity if mismanaged.
The patho-epidemiology of intra-articular scapular fractures is inextricably linked to high-energy trauma. The scapula is heavily shielded by a robust muscular envelope and the thoracic rib cage; therefore, fracturing its articular surface typically requires massive force vectors. Motor vehicle collisions, motorcycle accidents, and falls from significant heights are the most common mechanisms. Because of the energy required to produce these fractures, the incidence of concomitant injuries is staggeringly high. Up to 80% to 90% of patients will present with associated life-threatening trauma, including ipsilateral rib fractures, pneumothorax, pulmonary contusions, closed head injuries, and severe neurovascular compromise to the ipsilateral upper extremity. As orthopedic surgeons, we must maintain a high index of suspicion for these associated injuries and work closely with our trauma surgery colleagues during the initial resuscitation phase.
The primary objective in managing these complex fractures is the restoration of glenohumeral articular congruity and the re-establishment of the Superior Shoulder Suspensory Complex (SSSC). The SSSC is a critical osteoligamentous ring consisting of the glenoid process, the coracoid process, the coracoclavicular ligaments, the distal clavicle, the acromioclavicular joint, and the acromial process. Disruption of this ring, particularly when coupled with intra-articular step-off or gap formation, inevitably alters the biomechanics of the shoulder. Failure to achieve an anatomic or near-anatomic reduction leads to rapid, irreversible post-traumatic osteoarthritis, chronic glenohumeral instability, and profound functional deficits.
Historically, the pendulum swung heavily toward non-operative management for almost all scapular fractures, driven by the perceived morbidity of the surgical approaches. However, modern advancements in advanced cross-sectional imaging, a deeper understanding of functional outcomes, and the refinement of muscle-sparing surgical approaches have drastically shifted our paradigm. Today, we recognize that leaving a significantly displaced intra-articular glenoid fracture to heal in a malreduced position condemns the patient to a predictably poor outcome. Surgical intervention, when executed with precision, is not merely an option—it is the standard of care for preserving the longevity and function of the native shoulder joint.
Detailed Surgical Anatomy and Biomechanics
Mastery of intra-articular scapular fracture fixation begins and ends with an intimate understanding of the surrounding surgical anatomy. The scapula is a flat, triangular bone that serves as the dynamic foundation of the shoulder girdle, suspended primarily by muscular attachments rather than rigid bony articulations. The articular segment, the glenoid cavity, is a shallow, pear-shaped fossa that provides a highly constrained, yet incredibly mobile, articulation with the humeral head. The articular cartilage is thinnest centrally (the "bare area") and thickest peripherally, with an average depth of approximately 5 mm. The glenoid is typically retroverted between 2 and 7 degrees relative to the plane of the scapular body, a critical metric to remember when directing lag screws from anterior to posterior or vice versa.
The osseous architecture of the scapula dictates our fixation strategy. The central body of the scapula is paper-thin and translucent, offering absolutely no purchase for standard cortical or cancellous screws. Therefore, effective internal fixation relies entirely on identifying and utilizing the dense cortical "pillars" of the scapula. The four primary zones of reliable bone stock are the lateral border (the strongest pillar, extending from the inferior glenoid neck to the inferior angle), the scapular spine, the base of the coracoid process, and the acromion. When templating our constructs, plates must be contoured to span from the articular fragments to these dense cortical pillars to achieve absolute stability.
Navigating the muscular intervals to access these pillars requires a profound respect for the regional neurovascular structures. The posterior approach, which is the workhorse for most glenoid fossa fractures, places the suprascapular and axillary nerves at significant risk. The suprascapular nerve (C5-C6) branches from the upper trunk of the brachial plexus, passes through the suprascapular notch (inferior to the transverse scapular ligament), innervates the supraspinatus, and then courses around the base of the scapular spine through the spinoglenoid notch to innervate the infraspinatus. Retraction of the infraspinatus must be meticulous to avoid a traction neuropraxia at the spinoglenoid notch.
Similarly, the axillary nerve (C5-C6) and the posterior circumflex humeral artery exit the axilla through the quadrangular space, bordered by the teres minor superiorly, the teres major inferiorly, the long head of the triceps medially, and the surgical neck of the humerus laterally. As the axillary nerve wraps around the inferior capsule of the glenohumeral joint, it lies mere millimeters from the inferior glenoid rim. Any dissection or retractor placement inferior to the glenoid neck must be performed under direct visualization, keeping instruments strictly extra-capsular and subperiosteal to prevent devastating iatrogenic denervation of the deltoid and teres minor.
Exhaustive Indications and Contraindications
The decision to operate on an intra-articular scapular fracture requires a careful synthesis of radiographic parameters, patient physiology, and functional demands. We do not operate on radiographs alone; however, precise geometric criteria have been established to guide our surgical decision-making. The overarching goal is to prevent articular step-off that would lead to point-loading on the cartilage, and to prevent gap formation that would destabilize the humeral head.
For anterior glenoid rim fractures (typically Goss-Ideberg Type Ia), surgical intervention is strongly indicated if the fracture fragment encompasses 25% or more of the anterior articular surface. Loss of this critical anterior buttress predictably leads to recurrent anterior glenohumeral instability. For posterior rim fractures (Goss-Ideberg Type Ib), the threshold is slightly higher; surgery is indicated if 33% or more of the posterior surface is involved. Regardless of the percentage of involvement, any rim fracture with greater than 5 to 10 mm of displacement should be considered for open reduction and internal fixation (ORIF).
For transverse or oblique fractures through the glenoid fossa (Goss-Ideberg Types II through VI), the indications are centered on articular congruity. An articular step-off of 5 mm or more is universally accepted as an absolute indication for surgery. Furthermore, if the humeral head fails to lie concentrically within the glenoid cavity on the true AP or axillary radiographs—indicating dynamic subluxation—surgical stabilization is mandatory. We also consider surgery for significant angular displacement of the glenoid neck (greater than 40 degrees) or medial translation (greater than 15 to 20 mm), especially if part of a double disruption of the SSSC (e.g., a "floating shoulder").
Contraindications must be weighed heavily, given the magnitude of the surgical approaches. Absolute contraindications include patients who are medically unstable for prolonged anesthesia, those with severe traumatic brain injuries where functional recovery of the limb is impossible, and the presence of active infection or devastating soft tissue degloving over the planned surgical incisions. Relative contraindications include severe osteopenia (which severely limits hardware purchase), pre-existing severe glenohumeral osteoarthritis, and non-ambulatory patients with low functional demands where the risks of surgery outweigh the theoretical benefits of articular restoration.
| Category | Indications for Operative Fixation | Contraindications (Absolute & Relative) |
|---|---|---|
| Glenoid Rim | >25% anterior surface involvement | Absolute: Medically unstable for prolonged anesthesia |
| >33% posterior surface involvement | Absolute: Active local soft tissue infection / open wound | |
| >5-10 mm fragment displacement | Absolute: Severe traumatic brain injury with no limb function | |
| Glenoid Fossa | >5 mm intra-articular step-off | Relative: Severe osteoporosis precluding hardware purchase |
| Humeral head subluxation / non-concentricity | Relative: Pre-existing advanced glenohumeral osteoarthritis | |
| Glenoid Neck | >40 degrees angular displacement | Relative: Extreme soft tissue swelling/blistering (delay surgery) |
| >15-20 mm medial translation | Relative: Low-demand, non-ambulatory patient |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock upon which successful intra-articular scapular fixation is built. This process begins with an exhaustive imaging protocol. While standard trauma radiographs (true AP, scapular Y, and axillary views) provide a foundational understanding of the injury pattern, they are grossly insufficient for definitive surgical planning. The complex, overlapping bony architecture of the shoulder girdle obscures the fine details of articular step-offs and comminution.

Therefore, a high-resolution computed tomography (CT) scan with two-dimensional multiplanar reformats and three-dimensional (3D) surface rendering is absolutely mandatory. The 3D reconstructions allow the surgeon to mentally "rotate" the scapula, identifying the precise location of the primary fracture lines, the presence of intercalary fragments, and the optimal vectors for lag screw placement. Furthermore, digital subtraction of the humeral head from the 3D model provides an unobstructed en face view of the glenoid fossa, allowing for precise quantification of the articular defect.

Once the imaging is analyzed, virtual or physical templating is performed. The surgeon must select the appropriate surgical approach based on the fracture morphology. Anterior rim fractures dictate an anterior deltopectoral approach, while posterior rim and the vast majority of fossa fractures require a posterior approach (either the classic Judet or the modified Judet). Hardware selection typically involves 2.7 mm or 3.5 mm pelvic reconstruction plates, which can be contoured in three dimensions to match the complex topography of the scapular pillars. Pre-contoured, anatomically specific locking plates are also available and can be highly advantageous in comminuted or osteopenic scenarios.
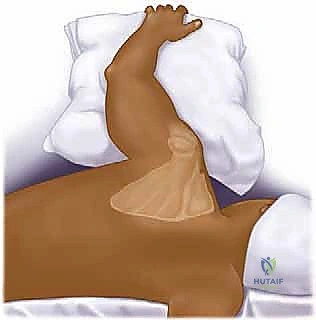
Patient positioning is critical for both surgical exposure and intraoperative fluoroscopy. For posterior approaches, the patient is placed in the lateral decubitus position on a radiolucent table. A beanbag is utilized to secure the torso, and the patient is rolled posteriorly approximately 15 to 20 degrees. This slight posterior tilt allows the scapula to fall away from the thoracic cage, maximizing the working space. The ipsilateral arm is prepped free and draped over a sterile Mayo stand or held by an assistant, allowing for dynamic manipulation of the shoulder joint to assess reduction and stability.


Conversely, for anterior approaches targeting the anterior glenoid or coracoid, the beach chair position is preferred. The patient is elevated to 45-60 degrees, with the head securely immobilized. The arm is again prepped free. Regardless of the position chosen, the C-arm fluoroscopy unit must be brought into the field prior to draping to ensure that true AP, axillary, and lateral views can be obtained without obstruction from the table or positioning devices.

Step-by-Step Surgical Approach and Fixation Technique
The Surgical Approach: Posterior and Anterior Corridors
The choice of surgical approach is dictated entirely by the fracture morphology mapped out on the preoperative 3D CT scan. For the vast majority of intra-articular glenoid fossa fractures (Goss-Ideberg Types II-VI) and posterior rim fractures, a posterior approach is utilized. The classic Judet approach involves a massive, expansile L-shaped incision along the scapular spine and medial border, elevating the entire infraspinatus muscle belly. However, due to significant morbidity and devascularization, we heavily favor the modified Judet approach or targeted muscle-sparing intervals.
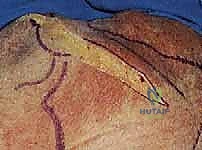
For the modified posterior approach, a linear incision is made directly over the lateral border of the scapula, extending from the posterior corner of the acromion distally toward the inferior angle. The deep fascia is incised, and the internervous plane between the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve) is developed.

This interval provides direct access to the lateral scapular pillar and the posterior glenoid neck. If superior extension is required to access the superior glenoid or scapular spine, the interval between the posterior deltoid and the infraspinatus can be utilized, taking great care to identify and protect the suprascapular nerve as it traverses the spinoglenoid notch.

For anterior glenoid rim fractures (Goss-Ideberg Type Ia) or fractures involving the coracoid base, the standard deltopectoral approach is employed. An incision is made from the coracoid process extending distally toward the deltoid tuberosity. The cephalic vein is identified and typically retracted laterally with the deltoid. The clavipectoral fascia is incised, and the conjoined tendon is retracted medially. The subscapularis is then identified. To access the anterior glenoid, a vertical tenotomy of the subscapularis is performed approximately 1.5 to 2 cm medial to its insertion on the lesser tuberosity, or a lesser tuberosity osteotomy can be performed. The underlying capsule is incised to expose the articular fracture.

Fracture Exposure and Provisional Reduction
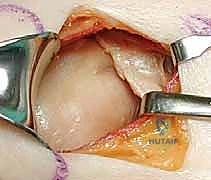
Once the fracture site is exposed, a meticulous hematoma evacuation and debridement of interposed soft tissue or periosteum must be performed. In intra-articular fractures, visualizing the articular surface is paramount. This can often be achieved by placing a Schanz pin into the humeral head and applying lateral traction, effectively distracting the glenohumeral joint. Alternatively, a Fukuda retractor can be carefully placed within the joint space.

Reduction of the articular fragments is technically demanding. Dental picks, small periosteal elevators, and pointed reduction forceps (Weber clamps) are used to manipulate the fragments. The reduction must be assessed both under direct visualization of the articular surface and via fluoroscopy. Once an anatomic reduction of the articular surface is achieved, it is provisionally stabilized with multiple 1.6 mm or 2.0 mm Kirschner wires (K-wires). These wires should be placed peripherally so as not to interfere with the planned trajectory of the definitive lag screws.
Definitive Fixation Construct
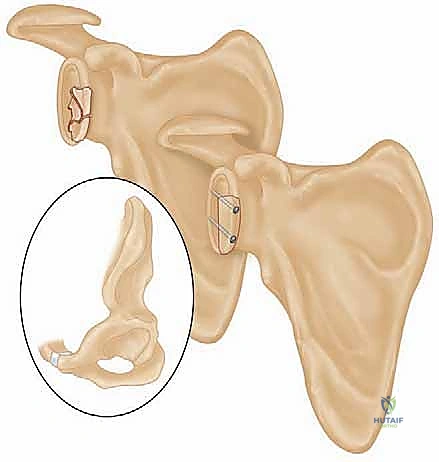
The philosophy of fixation for intra-articular scapular fractures relies on the principles of absolute stability for the articular surface and buttress plating for the metaphyseal/diaphyseal extensions. Following provisional K-wire fixation, definitive articular reduction is achieved using 2.7 mm or 3.5 mm cortical lag screws. These screws are directed from the intact peripheral bone, across the fracture plane, and into the dense subchondral bone of the articular fragment. Extreme care must be taken to ensure these screws do not penetrate the articular cartilage; fluoroscopic confirmation in multiple planes is mandatory.


Once the articular block is reconstituted, it must be securely attached to the axial skeleton of the scapula. This is accomplished by applying a contoured plate along the lateral border of the scapula. A 2.7 mm or 3.5 mm reconstruction plate is meticulously bent to match the curve of the lateral pillar.
The plate functions in a buttress mode, neutralizing the shear forces that act upon the glenoid neck during shoulder motion. In cases of severe comminution or osteopenia, locking plates provide superior pull-out strength.

If the fracture extends into the scapular spine or acromion, a second plate may be required along the superior pillar to create an orthogonal construct. After final tightening of all screws, the joint is taken through a full range of motion to ensure no crepitus or hardware impingement exists, and final fluoroscopic images are saved.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, operative management of intra-articular scapular fractures carries a distinct complication profile. The surgeon must be prepared to identify and manage these issues promptly to optimize patient outcomes. Nerve injury is arguably the most feared complication, given the proximity of the suprascapular and axillary nerves to the surgical field.
Suprascapular nerve palsy occurs in approximately 2% to 5% of cases, typically secondary to aggressive retraction of the infraspinatus or direct injury at the spinoglenoid notch. Axillary nerve injury is less common but more devastating, resulting from errant dissection inferior to the glenoid neck. Most of these injuries are neuropraxias that resolve with time and supportive care; however, if a nerve is known to be transected intraoperatively, immediate primary repair or nerve grafting is indicated.
Hardware-related complications, including screw penetration into the joint or symptomatic plate prominence, occur in 5% to 10% of cases. Intra-articular hardware leads to rapid chondrolysis and requires urgent reoperation for removal. Post-traumatic osteoarthritis is a late complication, occurring in up to 20% of patients despite anatomic reduction, driven by the initial chondral injury at the time of impact.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Suprascapular Nerve Palsy | 2% - 5% | Retraction injury at spinoglenoid notch | Observation, EMG at 3 months; tendon transfers if permanent |
| Axillary Nerve Palsy | 1% - 3% | Dissection inferior to glenoid neck | Observation; nerve exploration/grafting if no recovery |
| Intra-articular Hardware | 3% - 5% | Poor fluoroscopic visualization | Urgent arthroscopic or open hardware removal |
| Post-Traumatic Osteoarthritis | 10% - 20% | Initial cartilage impaction, malreduction | NSAIDs, injections; Total Shoulder Arthroplasty (TSA) |
| Infection (Deep) | 1% - 2% | Poor soft tissue envelope, hematoma | Urgent I&D, culture-specific IV antibiotics, retain stable hardware |
| Nonunion | < 1% | Inadequate fixation, smoking | Revision ORIF with bone grafting |
In cases where post-traumatic osteoarthritis becomes severely symptomatic and refractory to conservative management, salvage procedures are required. If the rotator cuff remains intact and functional, an anatomic total shoulder arthroplasty (TSA) can be performed. However, if the prior trauma or surgical approaches have compromised the rotator cuff, or if there is severe glenoid bone loss, a reverse total shoulder arthroplasty (rTSA) is the salvage procedure of choice to restore stability and elevation.
Phased Post-Operative Rehabilitation Protocols
The success of a beautifully executed surgical fixation can be entirely undone by an inappropriate rehabilitation strategy. The post-operative protocol must strike a delicate balance between protecting the fragile osteosynthesis and preventing devastating shoulder stiffness (adhesive capsulitis). Rehabilitation is typically divided into four distinct phases, tailored to the patient's specific fracture pattern and the rigidity of the fixation achieved intraoperatively.
Phase I: Protection and Early Passive Motion (Weeks 0-4)
Immediately post-operatively, the patient is placed in an abduction sling to remove tension from the repaired muscular intervals and the fracture site. Cryotherapy is utilized aggressively to manage edema. During this phase, absolute protection of the construct is the priority. However, to prevent capsular contracture, gentle passive range of motion (PROM) is initiated within safe zones determined by the surgeon. Typically, forward flexion is limited to 90 degrees, and external rotation is limited to neutral. Active motion of the elbow, wrist, and hand is highly encouraged to prevent distal edema and stiffness.
Phase II: Active-Assisted Range of Motion (Weeks 4-8)
As early callus formation begins and the soft tissues heal, the sling is gradually weaned. The focus shifts to active-assisted range of motion (AAROM). Patients utilize pulleys, wand exercises, and wall-walks to increase their arc of motion. Forward flexion is progressed to 140 degrees, and external rotation is advanced as tolerated. Submaximal isometric exercises for the deltoid and rotator cuff can be initiated, provided they do not induce pain at the fracture site. Radiographs are typically obtained at the 6-week mark to confirm maintenance of reduction and assess for early bony union.
Phase III: Active Motion and Early Strengthening (Weeks 8-12)
Once clinical and radiographic evidence of union is established, typically around 8 to 10 weeks, the patient progresses to full active range of motion (AROM) in all planes. The emphasis now shifts to restoring the dynamic stabilizers of the shoulder. Progressive resistance exercises using elastic bands and light weights are introduced, focusing on the rotator cuff, deltoid, and periscapular stabilizers (rhomboids, trapezius, serratus anterior). Scapulothoracic rhythm must be normalized to prevent impingement syndromes.
Phase IV: Advanced Strengthening and Return to Activity (Months 3-6+)
In the final phase, rehabilitation becomes highly individualized based on the patient's occupational and athletic demands. Advanced strengthening, plyometrics, and sport-specific drills are incorporated. Heavy lifting and contact sports are generally restricted until at least 6 months post-operatively, and only after a CT scan confirms complete osseous consolidation of the intra-articular fracture lines. Patients must be counseled that maximal medical improvement may take up to 12 to 18 months, and mild residual deficits in terminal range of motion are common.
Summary of Landmark Literature and Clinical Guidelines
The evolution of our understanding and management of intra-articular scapular fractures is deeply rooted in several landmark orthopedic studies. A historical perspective is essential for appreciating the current standard of care.
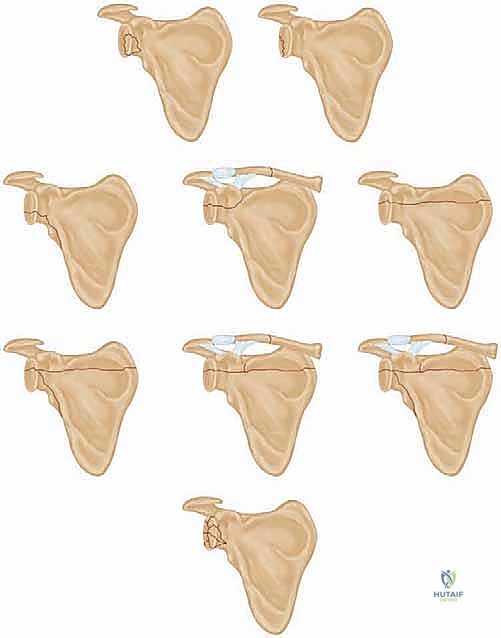
The foundational classification system and natural history of these injuries were elegantly described by Ideberg et al. in 1995. In their massive retrospective review of over 300 scapular fractures, they categorized glenoid fractures based on anatomic patterns and highlighted the poor outcomes associated with non-operative management of significantly displaced intra-articular variants. This study established the Goss-Ideberg classification that remains the lingua franca for orthopedic surgeons today.
Subsequently, Kavanagh et al. published critical guidelines defining the acceptable limits of displacement. Their biomechanical and clinical observations established the widely accepted criteria for operative intervention: >5 mm of articular step-off or significant subluxation of the humeral head. They demonstrated that step-
